Figures & data
FIGURE 1. Patient 1 presenting with chronic scleritis of the right eye: Panel A: B-ultrasonography of the right eye showing temporal and nasal thickening of the sclera. Panel B: UBM demonstrating nodular anterior nodular scleritis of the right eye. Panel C: Scleral biopsy of patient 1, x100 magnification. Lymphoplasmocytic B cells infiltration of the sclera. IgG4 immunostaining showing 50% of IgG4 + plasmocytes without any signs of fibrosis or vascularitis. Panel C: IgG4 staining showing important IgG4 deposit >50%. Panel D: Hematocylin eosin sections demonstrating massive lymphoplasmocytic infiltration.
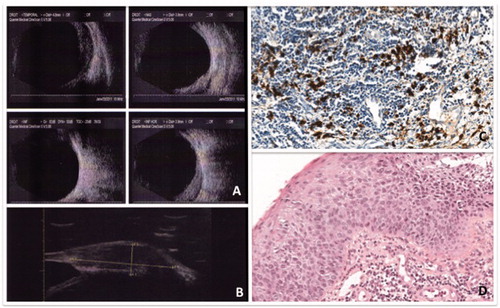
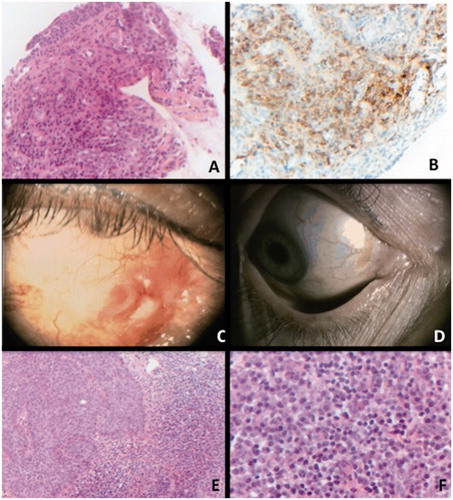
FIGURE 2. Conjunctival biopsy of case 2. Panel A: Haematoxylin eosin staining, x200 magnification. Presence of a lymphoplasmocytic infiltration of the conjunctiva. Panel B: IgG4 immunostaining, x200 magnification.Diffuse staining is observed in the sample, composed with 85% of plasmocytes. Panel C: Clinical picture of patient 2 demonstrating conjunctival inflammation relapsing with in situ carcinoma after steroids treatment. Panel D: Complete regression of the carcinoma after 2 cycles of topical mytomicin. Panel E: Conjunctival biopsy of case 2 after apparent relapse of inflammation. Haematoxylin x100 left: epithelial dystrophy without crossing the basal membrane (in situ carcinoma), adjacent to a large lymphoplasmocytic infiltration. Panel F: x400 magnification. Plasmocytes with typical feature of cartwheel nucleus and light appearance of cytoplasm.