Figures & data
Figure 1. Postoperative photograph of both knees (anterior view), illustrating the large cavity following surgical incision, drainage and debridement of the abscess secondary to corticosteroid knee joint injection.

Figure 2. Illustration depicting the anterolateral entry point for knee injections; with the knee in 90 degrees of flexion, the needle entry point (just above ‘A’) should be in the palpable soft spot between the patella, lateral femoral condyle and proximal tibia (Gerdy's tubercle).
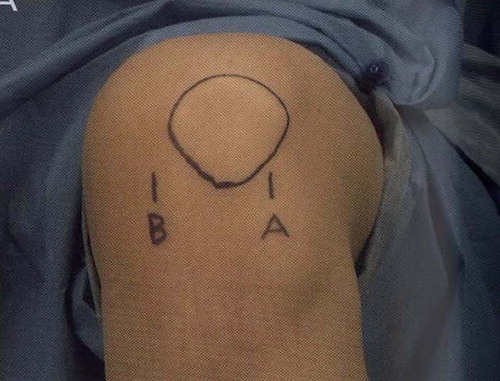
Table I. For primary care providers: when NOT to inject.