
Figures & data
Figure 1. Study flow chart as executed in the emergency service of the hospital of Genk, Belgium. AMI, acute myocardial infarction; H-FABP, heart-type fatty acid binding protein.
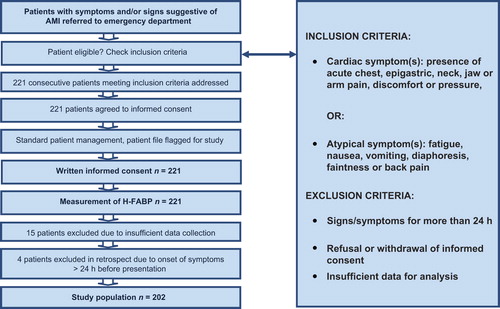
Table 1. Outcome definitions as used by the expert panel.
Table 2. Patient characteristics.
Figure 2. Receiver operating characteristic (ROC) curve of high sensitivity troponin and H-FABP, optimal cut-off point for H-FABP using ACS as outcome. ACS, acute coronary syndrome; H-FABP, heart-type fatty acid binding protein; hs-cTnT high sensitivity cardiac specific troponin T; ROC curve, receiver operating characteristic curve.
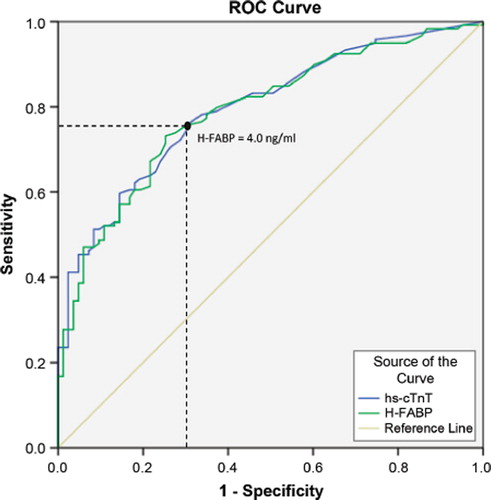
Table 3. Sensitivity and specificity of H-FABP for ACS at different cut-off values between positive and negative. Sensitivity and specificity of H-FABP for ACS at different cut-off values are given for all patients presenting complaints with a duration of 0–24 h and for all patients presenting complaints with a duration of 3–24 h at presentation. NPV is estimated for a population representative for primary care (incidence of ACS = 22%). Sensitivity, specificity and NPV for hs-cTnT with a cut-off of 14 pg/ml are given for comparison.
Table 4. Sensitivity and specificity of hs-cTnT and H-FABP. Sensitivity and specificity of hs-cTnT (cut-off 14 pg/mL) and H-FABP (cut-off 4 ng/mL) for AMI at different time intervals after onset of complaints.
Table 5. Sensitivity of hs-cTnT and H-FABP. Sensitivity and median plasma concentrations (25th, 75th percentile) of hs-cTnT (cut-off 14 pg/ml) and H-FABP (cut-off 4 ng/ml) for STEMI, nSTEMI, all AMI (STEMI and nSTEMI), unstable angina and all ACS (AMI and unstable angina) at presentation, for all patients presenting complaints with a duration of 0–24 h and 3–24 h respectively.
Table 6. Predictive values and likelihood ratios. PPV and NPV of hs-cTnT (cut-off 14 pg/ml) and H-FABP (cut-off 4 ng/ml) for AMI and ACS at time intervals of 0–24 h and 3–24 h after onset of complaints in a primary care setting with an incidence of AMI of 17% and ACS of 22%. PLR, NLR and OR of hs-cTnT (cut-off 14 pg/ml) and H-FABP (cut-off 4 ng/ml) for AMI and ACS at time intervals of 0–24 h and 3–24 h after onset of complaints.