Figures & data
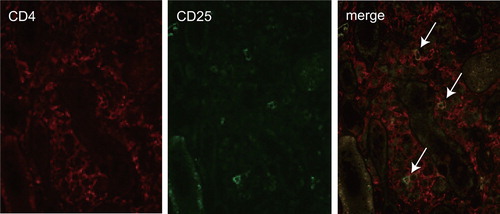
Figure 5. Double immunostaining of CD4 and CD25 in tubulointerstitial lesion. Mononuclear cells positive for CD4 (red) or CD25 (green) are detected. The merge image showed a few cells doubly positive for CD4 and CD25 in an area of interstitial cell infiltration lesion (arrows).