Figures & data
Figure 1. The Müller classification of long bone fractures.
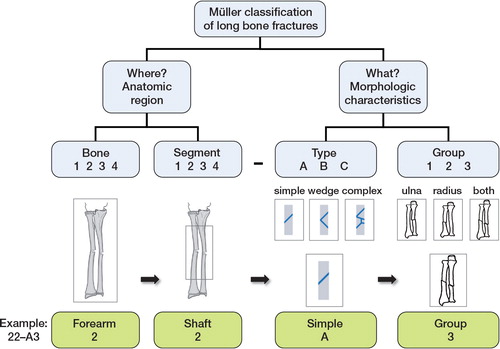
Table 1. Overall agreement, reliability, and accuracy for all signs of the Müller comprehensive classification of long bone fractures in childhood fractures
Table 2. Agreement, reliability, and accuracy according to each sign in the Müller classification of long bone childhood fractures. Only the codes that were given the same classification code at the previous signs were considered when the next sign was calculated
Figure 2. The rule of the square: “The proximal and distal segments of long bones are defined by a square whose sides are the same length as the widest part of the epiphysis” (Müller et al. Citation1990). Müller classification: The width defined by both bones. The reference line defined as the most distal (or proximal) part of the bone. Li-La classification (and in this study): The width defined by one bone (radius). The reference line defined as the epiphyseal plate.
AO pediatric classification: The width defined by both bones. The reference line defined as the epiphyseal plate. The proximal lines of the squares define the border between the diaphysis and the metaphysis. The fracture illustrated is defined as a forearm shaft fracture according to the Müller and Li-La classifications (and in this study), and as a distal forearm fracture according to the AO pediatric classification.
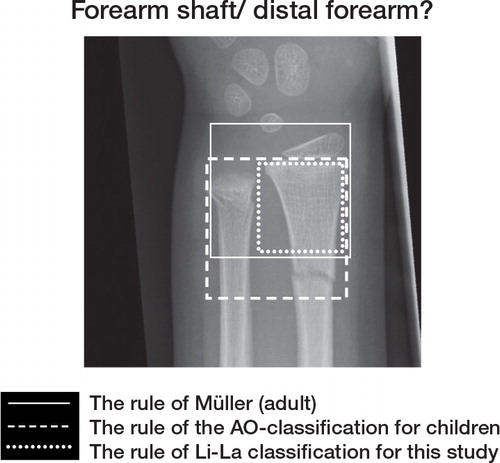
Table 3. Accuracy of the surgeons’ blinded re-coding for the most frequent bone segments according to 3 and 4 signs of the classification
Table 4. Distribution of the fractures according to the reference dataset