Figures & data
Figure 1. The rise of spinal fusion procedures for degenerative conditions in the USA between 1988 and 2001. Note the rapid increase after 1996, when fusion cages were approved. (Courtesy from Mr Richard A Deyo, J Am Board Fam Med 2009; 22: 62–68, reproduced with permission).
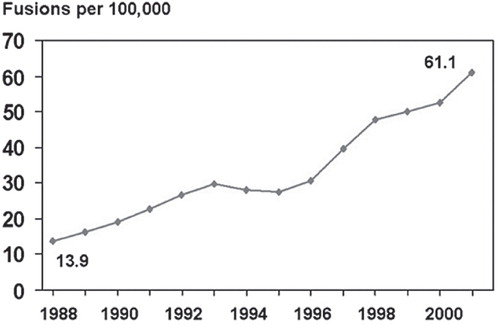
Figure 2. Immobilisation test by a thoracolumbosacral orthosis, e.g., a plaster cast. Extension of the cast with a thigh piece is optional and assumed to better immobilise the lumbosacral joint.
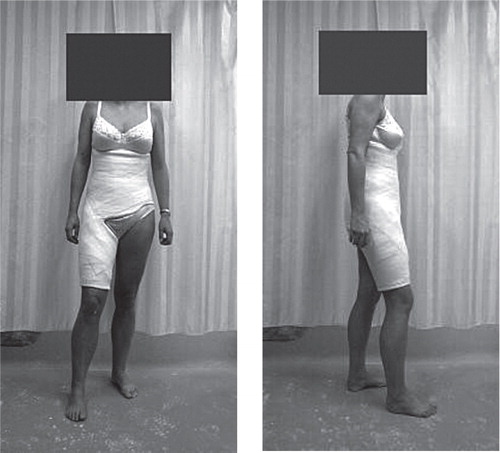
Figure 3. Provocative discography is performed under sterile conditions and with biplanar fluoroscopic control. The intended disc space is injected with contrast agent to provoke usual back pain. In addition, the amount of degeneration can be visualized on plain radiographs or CT scan.
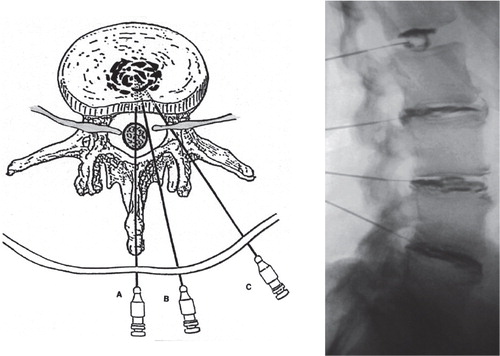
Figure 4. Temporary external transpedicular fixation trial: By externally fixing two vertebrae, one or more vertebral motion segments can be immobilised, thus simulating the effect of a spinal fusion.
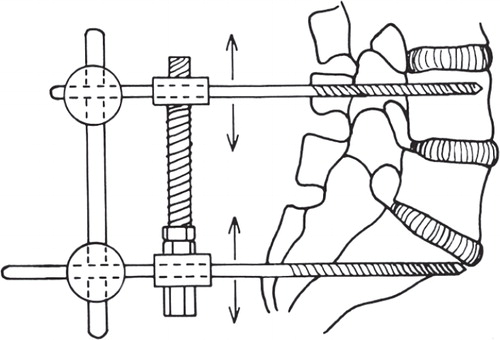
Table 1. Orthosis study: Patient variables for both treatment groups
Table 2. Adjacent level discography: Diagnosis of all analysed patients (numbers)
Table 3. TETF: Descriptives and mean VAS scores for pain in the patient groups with a negative and those with a positive external fixation test result
Table 4. QUADAS for prognostic studies: criteria to assess risk of bias
Table 5. Survey: Characteristics of the 62 respondents
Table 6. Survey: Respondents’ opinion to what extent patient-specific prognostic factors influence their clinical decision making in the treatment of CLBP. The numbers listed are percentages of valid responses
Table 7a. Survey: Respondents’ opinion on predictive tests for clinical decision making. The numbers listed are valid responses and respective percentages
Table 7b. Survey: The use of predictive tests by the surgeons in clinical practice. The numbers listed are valid responses and their respective percentages
Figure 5. Survey: The importance of listed factors in clinical decision making (presented as mean ± SD) as rated by the respondents on a scale from 0 (no importance) to 10 (maximal importance). Abbreviations: MRI = magnetic resonance imaging, TETF = temporary external transpedicular fixation.
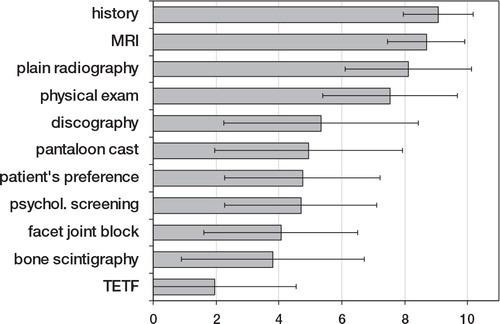
Table 8. Motion analysis: Patient characteristics and angles of lumbosacral sagittal rotation (degrees) in the unrestricted condition and in both plaster cast conditions, while performing spinal flexion-extension, pelvic tilt, and walking
Figure 6a. The differences (Delta) in range of sagittal rotation from both plaster casts to the range obtained in each patient in the condition with no support, during spinal flexion-extension. Note that a negative delta represents an immobilising effect.
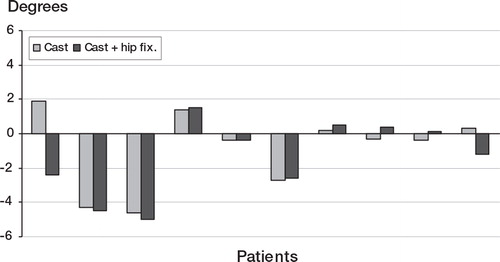
Figure 6b. The differences (Delta) in range of sagittal rotation from both plaster casts to the range obtained in each patient in the condition with no support, during pelvic tilt. Note that a negative delta represents an immobilising effect.
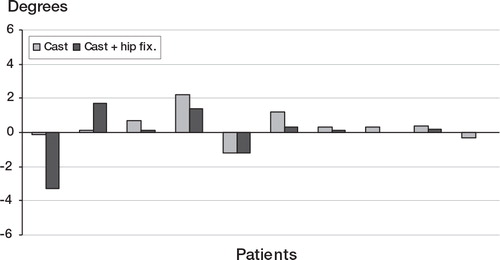
Figure 6c. The differences (Delta) in range of sagittal rotation from both plaster casts to the range obtained in each patient in the condition with no support, during walking. Note that a negative delta represents an immobilising effect.
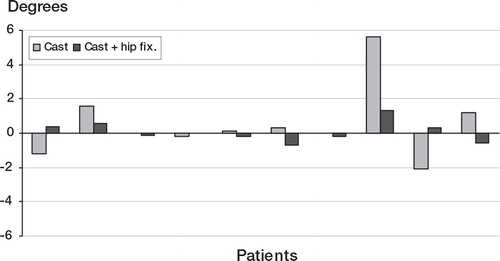
Table 9a. Orthosis: Summary of results in the 99 patients without prior spine surgery, classified by treatment and pantaloon cast test result
Table 9b. Orthosis: Summary of results in the 158 patients with prior spine surgery, classified by treatment and pantaloon cast test result
Table 10. Adjacent level discography: Cross-tabulation of the morphologic (Adams’ criteria) and the symptomatic status of the adjacent discs assessed by provocative discography in all 197 patients
Table 11. Adjacent level discography: Variables and clinical outcome of the 82 patients who underwent lumbar fusion classified by the result of provocative discography of the adjacent segments
Figure 7. Adjacent level discography: The distribution of the VAS scores before lumbar fusion and at follow-up for all fused patients with symptomatic and asymptomatic adjacent discs at preoperative discography. The VAS scores have been categorised as follows: 0–20, 21–40, 41–60, 61–80, and 81–100.
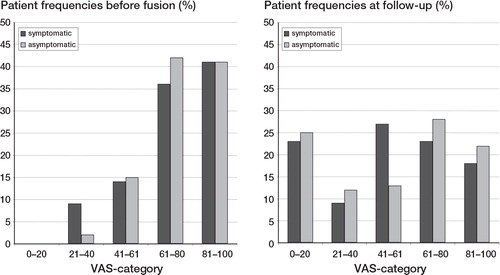
Table 12. Postdiscography discitis: Incidences in selected literature and current study by patient and by disc
Table 13. TETF: Characteristics and mean VAS scores for those patients with a negative and those with a positive test result.
Table 14. Fusion group: Numbers and percentages of patients with a negative external fixation test and those with a positive test, respectively, who had a clinically relevant improvement of 30% or more on the VAS for pain
Figure 8. Systematic review: PRISMA flow diagram of combined literature search and selection.
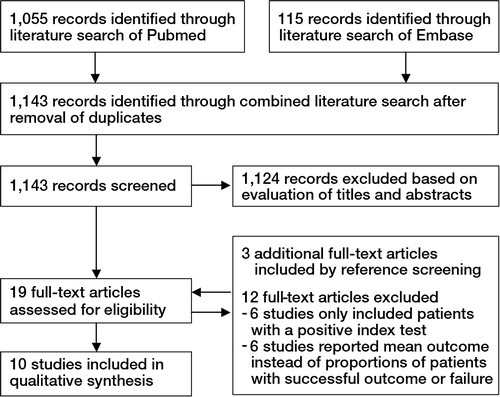
Table 15. Systematic review: Characteristics of primary prognostic studies on the clinical outcome of lumbar spinal fusion
Table 16. Systematic Review: Risk of Bias: Number of Quality Criteria of the Modified QUADAS Checklist a, that were met (+ = yes; – = no; ? = unclear)
Table 17. Systematic review: Summary prognostic accuracy of orthosis, provocative discography, and external transpedicular fixation for spinal fusion outcome