
Figures & data
Figure 1. Anteroposterior (left) and lateral (right) view of the thoracolumbar spine (T11 to L3) on postoperative radiographs after an AO type B2.3 fracture of L1. Bisegmental posterior instrumentation from T12 to L2 and anterior spondylodesis from T12 to L1 using an autologous rib graft was performed. The image shows the rib strut grafts in situ, arranged like a palisade.
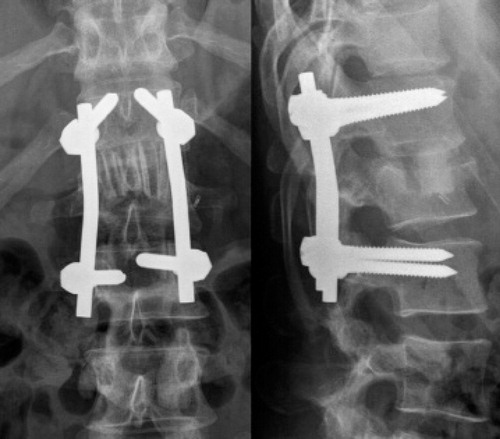
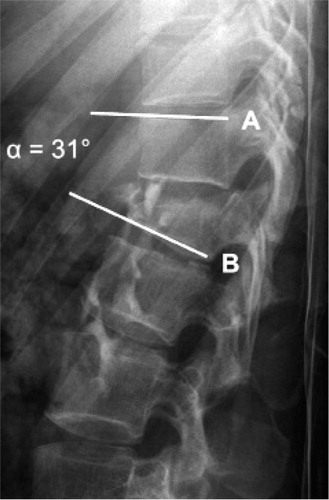
Figure 2. Lateral view of the thoracolumbar spine on a conventional radiograph after an AO type B1.2 fracture of L1. The segmental angle (α) was determined by measuring the angle between the line (B) parallel to the lower endplate of the fractured vertebra and the line (A) parallel to the upper endplate of the adjacent proximal vertebra (Keynan et al. Citation2006).
Individual patient characteristics, Cobb angles, and outcomes after posterior bisegmental instrumentation and monosegmental spondylodesis combined with anterior monosegmental spondylodesis using an autologous rib graft
Figure 3. Box plots of segmental angles preoperatively and postoperatively, 6 months and 12 months postoperatively, and 4.0 months (95% CI: 4.9–14.0) after implant removal, i.e. 28.0 months (95% CI: 26.2–36.7) postoperatively, and 1.5x interquartile range (whiskers). Values are median (lines), 95% CI (boxes), and range (bars). a significantly different from 6- and 12-month values (p < 0.001).
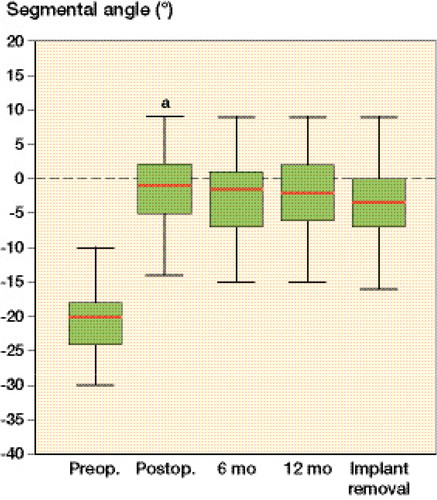
Figure 4. Postoperative image after an AO type B2.3 fracture of L1. Anterior spondylodesis resulted in solid fusion 2 years postoperatively, and the posterior instrumentation was therefore removed. The autologous rib grafts were incorporated and partially remodeled. There were no signs of lucency or resorption.
