Figures & data
Figure 1. Clinical course of the patient during the first admission. A: Initial clinical appearance. The anterior surface of the trunk exhibits a deep burn. B: Appearance after the first series of debridement and skin grafting. C and D: Multiple ulcers in the grafted skin and donor sites.

Figure 2. Clinical course after the second admission. A and B: Initial appearance on the second admission. Multiple recurrent ulcers are scattered in the grafted skin (A) and donor sites (B). C: Close-up view of the recurrent ulcers. D: Progression of the lesions. The lesions started as pustules (1), which then transformed to form a crust (2). When the crust was removed, a fresh ulcer appeared (3). E: Recent appearance of the patient after treatment with oral corticosteroids. The ulcers were restricted to limited areas; no ulcers are seen in this field.

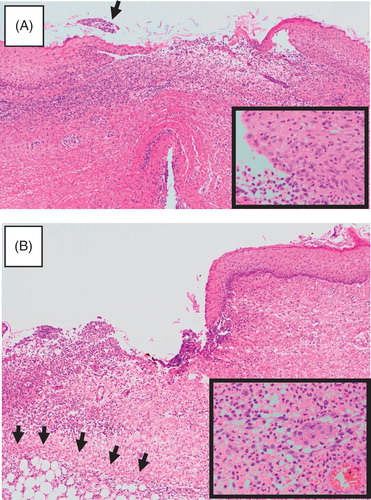
Figure 3. Histological findings of a recurrent ulcer. A: Early lesion. A pustule was biopsied, although it broke during handling. Heavy infiltration is seen in the upper dermis. A crust is already noted (arrow). Inlet: A close-up view of the epidermis at the periphery of the pustule, showing many neutrophils. B: Advanced lesion. The periphery of an ulcer was biopsied. Note the sharply demarcated border and heavy infiltration that extends to a part of the fat layer (arrows). Fibrosis is already seen on the right side. Inlet: A close-up view of the infiltration, showing neutrophils to predominate.
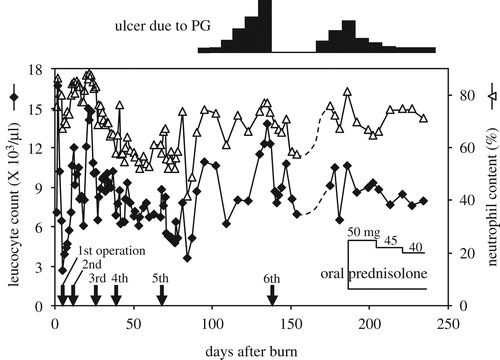
Figure 4. Clinical course of the present case. Trends in the leukocyte count (♦) and neutrophil content (△). Operations are indicated by arrows; the oral prednisolone dose is shown within the panel. The extent of ulcers due to PG is indicated above the panel.