Figures & data
Figure 1. Patient disposition. Patients were included in the analysis if they were 18–65 years old and had an ACS-related hospitalization during the study dates. Patients were required to have 12 months of continuous enrolment and pharmacy data prior to and following the index hospitalization. Of the more than 12,500 patients included in the analysis, 24% had a history of DM. ACS, acute coronary syndrome; DM, diabetes mellitus.
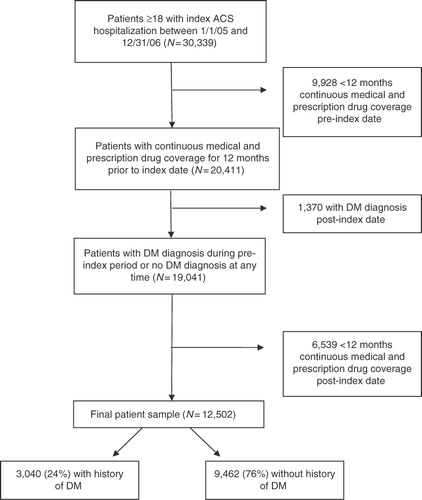
Table 1. Demographic and clinical characteristics of ACS patients with and without diabetes mellitus (N = 12,502).
Table 2. Resource utilization in patients with and without diabetes mellitus* (N = 12,502).
Figure 2. Mean total index hospitalization costs for ACS patients with DM versus without DM (US$ 2008). Total direct index hospitalization costs were significantly greater for patients with DM compared to those without DM among all ACS patients and regardless of the type of revascularization patients received during the index hospitalization. ACS, acute coronary syndrome; CABG, coronary artery bypass graft; DM, diabetes mellitus; PCI, percutaneous coronary intervention.
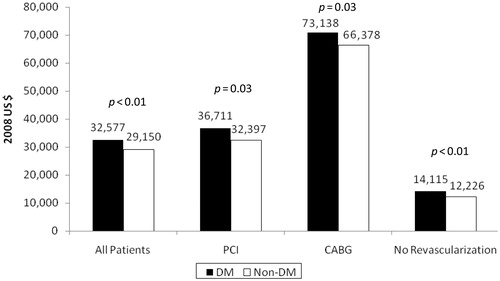
Figure 3. Mean total direct all-cause and ACS-related costs during the 12 months following the index ACS-related hospitalization in patients with and without diabetes mellitus (N = 12,502). Total direct all-cause costs were significantly greater for patients with DM compared to those without DM. Patients with DM had significantly higher all-cause pharmacy, outpatient, and rehospitalization costs compared to those without DM. Similar findings were seen with ACS-related total costs. Patients with DM had significantly higher pharmacy and rehospitalization costs compared to those without DM. However, ACS-related outpatient costs were higher for those without DM compared to those with DM. *p < 0.01; †p < 0.05. ACS, acute coronary syndrome; DM, diabetes mellitus.
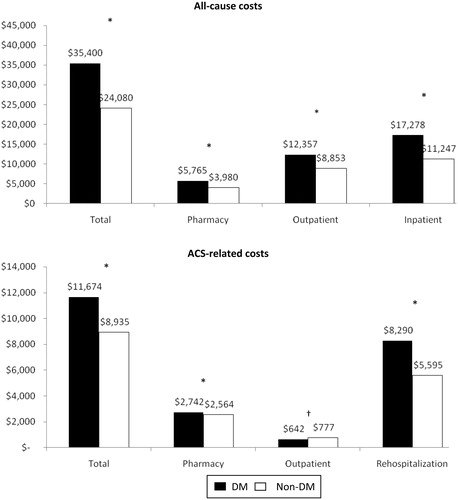
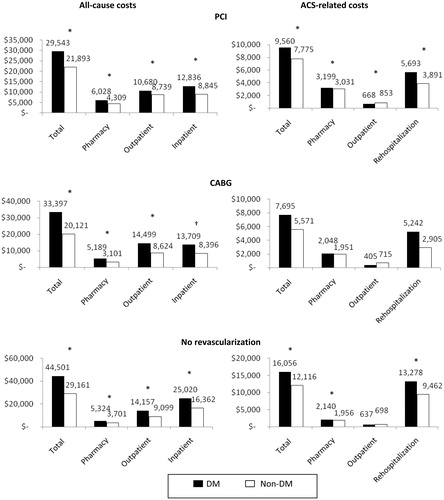
Figure 4. Mean total direct all-cause and ACS-related costs during the 12 months following the index ACS-related hospitalization in patients with and without diabetes mellitus by revascularization technique received (N = 12,502). All-cause and ACS-related healthcare costs for the 12-month period following the index hospitalization data were stratified by the type of revascularization procedure received during the index ACS-related hospitalization. Regardless of index revascularization procedure received, ACS patients with DM had significantly greater all-cause total healthcare costs compared to those without DM. Total ACS-related healthcare costs were generally greater for patients with DM compared to those without DM. However, in patients who underwent CABG during the index hospitalization, ACS-related total costs were not significantly different between patients with DM and those without DM. *p < 0.01; †p < 0.05. ACS, acute coronary syndrome; CABG, coronary artery bypass graft; DM, diabetes mellitus; PCI, percutaneous coronary intervention.
Drug classes and specific medications included in pharmacy costs.