Fabrice DuvalCentre Hospitalier, Rouffach, France (Fabrice Duval, Jean-Paul Macher); University of California, San Diego, California, USA (Barry D. Lebowitz)Correspondence[email protected]
,
Barry D. LebowitzCentre Hospitalier, Rouffach, France (Fabrice Duval, Jean-Paul Macher); University of California, San Diego, California, USA (Barry D. Lebowitz)
&
Jean-Paul MacherCentre Hospitalier, Rouffach, France (Fabrice Duval, Jean-Paul Macher); University of California, San Diego, California, USA (Barry D. Lebowitz)
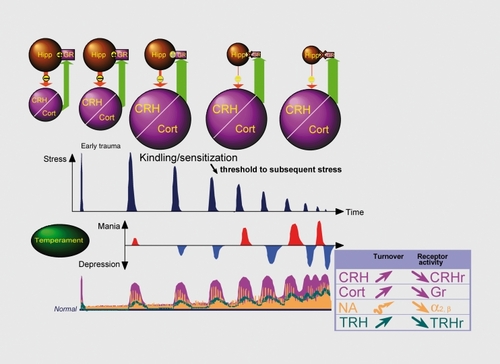
Figure 1. Major depression is a multifactorial disorder including predisposing temperament and personality traits, exposure to traumatic and stressful life events and biological susceptibility The kindling/sensitization hypothesis may explain some of the key aspects of depression: (i) the first lifetime episodes are more strongly associated with major life stress than are successive recurrences, (ii) the severity and duration of the nontreated episodes increase with clinical course, and (iii) the interval between episodes decreases with the duration of the illness. Damage to the hippocampus, as a result of the reduction in cellular density and glucocorticoid receptors, impairs the negative feedback system that dampens HPA activation. Since decreased hippocampal volume has been correlated with duration of depressive illness and CRH has a critical role in long-term effects of early-life stress on hippocampal integrity and function, it has been suggested that chronic hypercortisolemia, associated with alterations in neuroplasticity and neurogenesis, may underlie the vulnerability to subsequent depressive episode. On the other hand, hypercortisolemia may underlie dysregulation of the noradrenaline, dopamine, serotonin, and acetylcholine systems. TRH is a key central nervous system homeostatic modulator. In depression, TRH hypersecretion may be regarded as a compensatory mechanism in order to correct neurotransmitter alterations (especially those involving the serotonin and catecholamine systems). HPT, hypothalamic-pituitary-adrenal; CRH, corticotropin-releasing hormone; Cort, cortex; Hipp, hippocampus; NA, noradrenaline; TRH, thyrotropin-releasing hormone.
Table II. Specific depression subscales derived from the HAM-D by the microanalytic approach. SRI, Serotonin reuptake inhibitor; NRI, Noradrenaline reuptake inhibitor; DRI, Dopamine reuptake inhibitor; MAOI, monoamine oxidase inhibitor