Figures & data
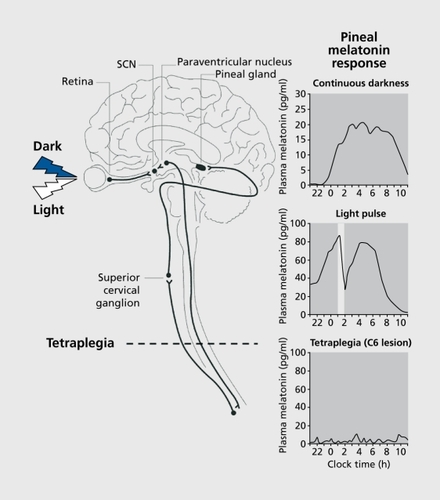
KneisleyLW.MoskowitzMA.LynchHJ.Cervical spinal cord lesions disrupt the rhythm in human melatonin excretion.J Neural Transm.1 97813(suppl)311323 ZeitzerJM.AyasNT.SheaSA.BrownR.CzeislerCA.Absence of detectable melatonin and perservation of Cortisol and thyrotropin rhythms in tetraplegia.J Clin Endocrinol Metab.2000852189219610852451 LockleySW.Human circadian rhythms: influence of light on circadian rhythmicity in humans. In: Squire LR, ed.New Encyclopaedia of Neuroscience, Oxford, UK: Elsevier. In press.