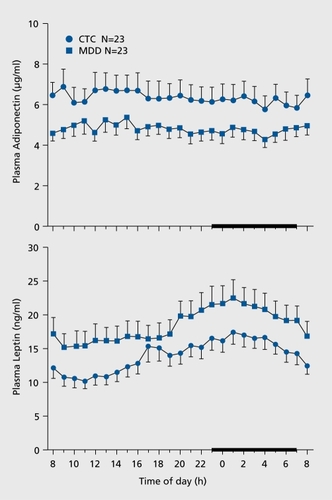
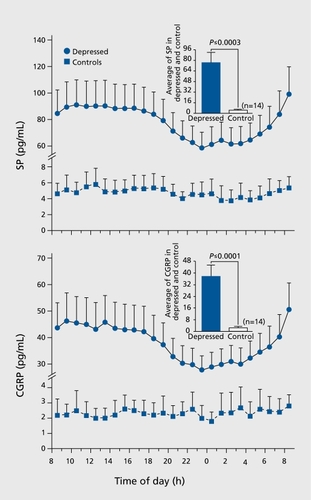
Major depressive disorder is a risk factor for low bone mass, central obesity, and other medical conditions
El trastorno depresivo mayor es un factor de riesgo para una masa ósea disminuida, obesidad central y otras condiciones médicas
Le trouble dépressif majeur est un facteur de risque de faible masse osseuse, d'obésité centrale et d'autres pathologies
Giovanni CizzaDiabetes, Obesity, Endocrine Branch, NIDDK, NIH, DHHS; Department of Laboratory Medicine, Clinical Center, NIH, DHHS, Bethesda, Maryland, USACorrespondence[email protected]