
Figures & data
Table I. Epidemiologic data for a cost analysis from a prospectively followed cohort of AN persons with chronic hepatitis B virus infection, 1983–2012
Table II. Base-case model assumptions for estimating the costs for hepatocellular carcinoma screening
Table III. Comparing the costs of 2 hypothetical screening scenarios for hepatocellular carcinoma (HCC) – Alaska, 1983–2012a
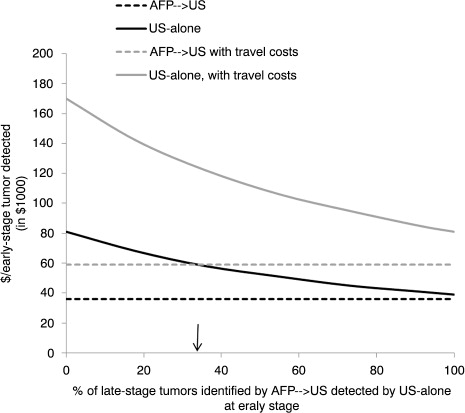
Fig. 1. Sensitivity analysis: Impact of varying the percentage of hepatocellular carcinoma tumours that were identified by AFP→US at a late stage and potentially identified by US-alone at an early stage in hepatitis B virus infected AN persons.*†‡§¶ Abbreviations: AFP, alpha-fetoprotein; US, ultrasound; ↓, indicates base-case assumption *Screening assumed to start for men at age ≥40 years and for women at age ≥50 years. †AFP→US assumes patients received screening for HCC by serum AFP measurements initially and switched to ultrasound if AFP >10 ng/mL; screening method resembles the Alaska Native Health System hepatocellular carcinoma screening program. ‡The number of additional tumours that might have been detected at an early stage (i.e. single tumour ≤5 cm in diameter or ≤3 tumours ≤3 cm in diameter) by an US-alone method is unknown; therefore, sensitivity analysis determined the cost/early-stage tumour detected by assuming US-alone method identified 0–100% of the tumours identified by AFP→US at a late stage. §Direct costs of screening discounted at 3%/year (reference year 2012) over a 30-year time horizon. ¶Assumes 60% of patients lived in a village without ready US access and required transportation to US facility.
Appendix Table I. Demographic and clinical characteristics of the cohort participants with history of hepatitis B virus (HBV) infection and those who developed hepatocellular carcinoma (HCC) – Alaska, 1983–2012.a