Figures & data
Figure 1. Flow chart of the entire donor limb procurement process.
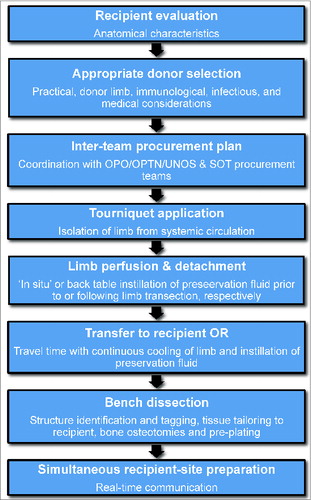
Figure 2. Chart outlining practical, donor limb specific, and immunological/medical considerations in proper donor selection.
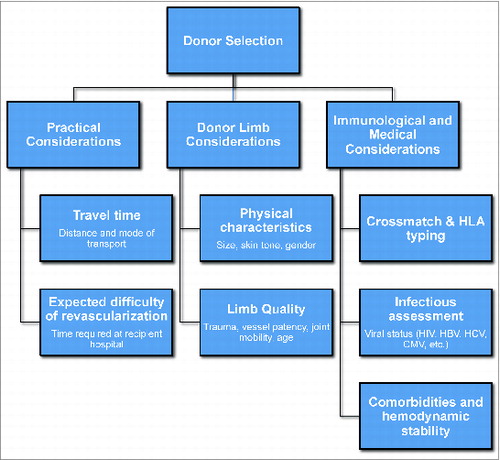
Figure 3. Pathways for donor limb harvest. (A) Prior to solid organ procurement, (B) Post- solid organ procurement, and (C) Simultaneously with solid organ procurement.
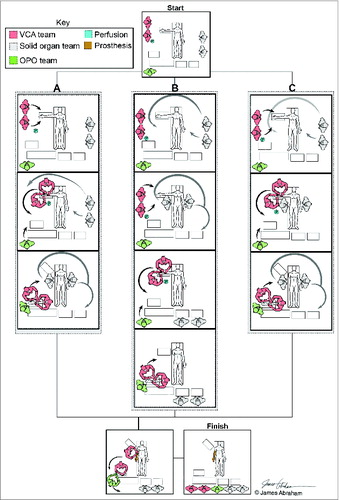
Figure 4. Tourniquet application. (A) The tourniquet may be placed at mid-humeral (for elbow transection) or proximal arm (for mid-humeral transection) dependent on recipient anatomical requirements (B) The pressure of the tourniquet should be sufficient to isolate the limb segment from the systemic vasculature.
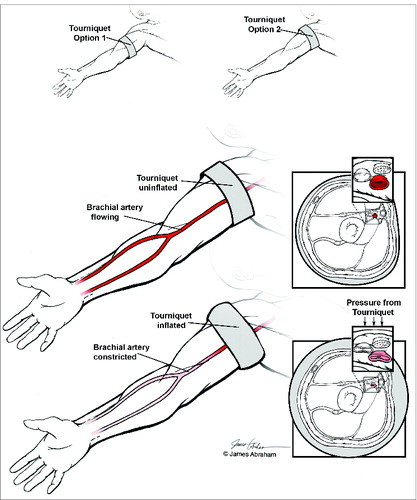
Figure 5. Preservation fluid instillation. (A) ‘In situ’ instillation: While the limb remains attached an infusion catheter is inserted into the brachial artery via arteriotomy. (B) Back table perfusion: Following rapid transection, the donor limb is transferred to the back table where preservation fluid is instilled. Forceps are used to open the arterial lumen.
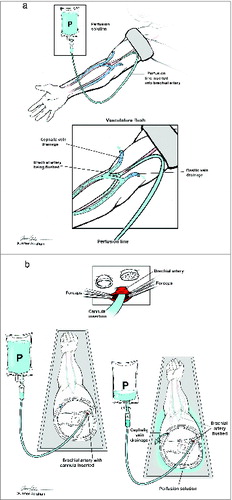
Figure 6. Possible levels of transection during upper extremity recovery. For forearm/hand transplantation, disarticulation at the level of the elbow is sufficient. For more proximal requirements, transection is typically at the level of the mid-humerus.
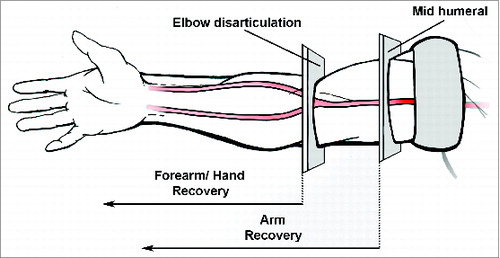
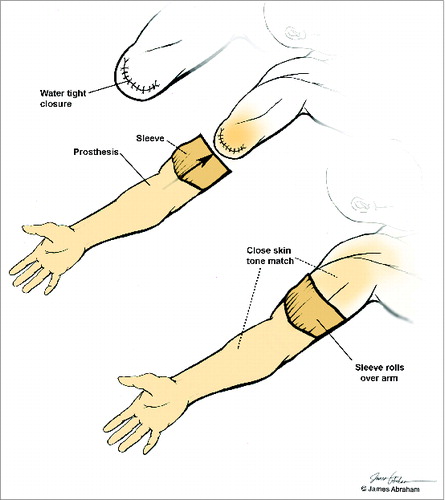
Figure 7. Fitting of the donor prosthesis. The donor stump is closed to achieve a water-tight seal. The sleeve on the proximal segment of the prosthesis is rolled over the stump.