Figures & data
Table 1. Relative mortality rates in patients with postoperative S. aureus infections by vaccination group and preoperative IL2 and IL17a levels
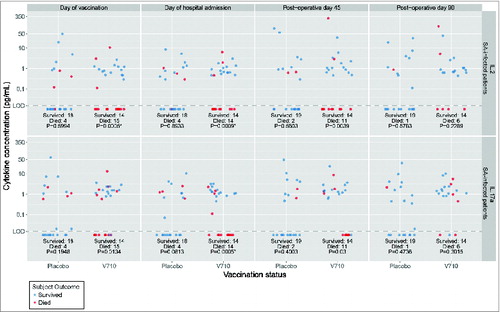
Figure 1. Log-plot of IL2 and IL17a levels over time in V710 and placebo recipients with postoperative S. aureus infections by survival versus death. Top Panels: IL2 levels. Bottom Panels: IL17a levels. Interleukin (IL) levels were measured with the Milliplex MAP human cytokine assay (EMD Millipore Corp, Merck KGaA, Darmstadt, Germany) having an approximate lower limit of quantification of 0.2–0.6 pg/mL and lower limit of detection (LOD) of ∼0.1 pg/mL. Rank values were compared between patients who survived or died in each group using Mann-Whitney tests adjusted for multiplicity with a Bonferroni correction of 40 (10 cytokines x 4 time points). Accordingly, α = 0.00125 was set as the threshold for statistical significance. The unadjusted p-values are shown at the bottom of each column and designated with an asterisk as significant when ≤0.00125. As summarized in , IL-values were arbitrarily dichotomized as detectable or undetectable. V710 recipients having preoperative IL-levels below the level of assay detection (both before and after vaccination) were more likely to succumb following postoperative S. aureus infections than similar patients with detectable levels. A comparable relationship between IL levels and death after postoperative S. aureus infections was not apparent in the placebo group, where in contrast to the V710 recipients, the mortality rate was numerically lower in placebo recipients with undetectable IL levels than in similar patients with detectable levels.