Abstract
This paper reports on a community-based study in 2001—02 in a rural district of Tamil Nadu, India, among 97 women who had had recent abortions, to examine their decision-making processes, the types of facility they attended and the extent of post-abortion complications they experienced. The 36 facilities they attended, both government and private, were ranked by 18 village health nurses, acting as key informants, as regards safety and quality of care. Three categories — qualified and safe, intermediate or unqualified and unsafe — were identified. Most of the providers were medically trained, and 75 of the 97 women went to facilities that were ranked as high or intermediate in quality. Government abortion services were mostly ranked intermediate in quality, and criticised by both women and village health nurses. There has been a substantial decrease in the numbers of traditional and unqualified providers. However, about 30% of the women experienced moderate to serious post-abortion complications, including women who went to facilities ranked high. We recommend that government facilities, both the district hospital and primary health centres, should improve their quality of care, that unqualified providers should be stopped from practising, and that all providers should be using the safer methods of vacuum aspiration and medical methods to reduce post-abortion complications.
Résumé
Une étude communautaire réalisée dans un district rural du Tamil Nadu, Inde, auprès de 97 femmes ayant récemment avorté a examiné leurs processus de décision, les types d’installations fréquentées et les complications après l’avortement. Les 36 centres, publics et privés, utilisés par les femmes étaient gérés par 18 infirmières de village qui servaient d’informatrices clés pour la sécurité et la qualité des soins. Trois catégories — soins qualifiés et s rs, intermédiaires ou non qualifiés et non s rs — ont été identifiées. La plupart des prestataires avaient suivi une formation médicale et 75 des 97 femmes s’étaient rendues dans des centres de qualité élevée ou intermédiaire. Les services publics d’avortement étaient généralement de qualité intermédiaire, et critiqués par les femmes et les infirmières de village. Le nombre de prestataires traditionnels et non qualifiés avait nettement diminué. Néanmoins, près de 30% des femmes avaient souffert de complications modéréesàgraves après l’avortement, mÁme celles qui étaient allées dans des centres bien classés. Nous recommandons que les centres publics, aussi bien l’hÁpital de district que les centres de soins de santé primaires, améliorent la qualité des soins ; les prestataires non qualifiés devraient Átre interdits de pratique et tous les praticiens devraient utiliser des techniques plus s res comme l’aspiration et les méthodes médicamenteuses pour réduire les complications après l’avortement.
Resumen
Este articulo informa sobre un estudio comunitario realizado en un distrito rural de Tamil Nadu, la India, en 97 mujeres que habáan experimentado un aborto reciente a fin de analizar sus procesos de toma de decisión, los tipos de establecimientos de salud que consultaron y el grado de complicaciones postaborto que presentaron. Los 36 establecimientos de salud, tanto gubernamentales como privados, fueron clasificados por 18 enfermeras del poblado, como informantes clave, respecto a la seguridad y calidad de la atención. Se establecieron tres categoráas: calificado y seguro, intermedio o no calificado e inseguro. La mayoráa de los prestadores de servicios tenáan formación médica, y 75 de las 97 mujeres acudieron a establecimientos de calidad alta o intermedia. Los servicios gubernamentales, clasificados principalmente como de calidad intermedia, recibieron cráticas tanto de las pacientes como de las enfermeras. Se ha visto una considerable disminución en el número de proveedores tradicionales y no calificados. No obstante, un 30% de las mujeres presentaron complicaciones postaborto de moderadas a graves, incluidas las mujeres que asistieron a los establecimientos de alta calidad. Recomendamos que los establecimientos de salud gubernamentales, mejoren su calidad de atención, sea prohibida la práctica de los proveedores no calificados y todos los proveedores utilicen los métodos más seguros de aspiración y métodos con medicamentos para disminuir las complicaciones postaborto.
When the Indian government liberalised the abortion law in 1971,Citation1 the primary motivation was to reduce the heavy toll of mortality and morbidity from unsafe abortions that had prevailed under the older, restrictive legislation.Citation2 The new legislation placed medical termination of pregnancy squarely under the control of medical doctors, and included provisions for training of medical doctors in abortion techniques. It also required certification of both doctors and facilities as prerequisites for abortion to be legal.Citation2
During the 1970s and 80s, there was a rapid rise in the recorded numbers of legally performed abortions to about 600,000 per year in 1986—88 when they then levelled off. Most researchers and health personnel in India believe the actual numbers of abortions are a great deal higher. Recent studies estimate that 6—7 million induced abortions occur annually in India.Citation3 The National Family Health Surveys in the 1990s estimated an abortion ratio of 1.9 to 100 live births, which is much lower than the estimates from many small scale, cross-sectional surveys, where abortion ratios ranged from 3.4—14 to 100 live births.Citation4 The difference between these estimates suggests that despite the legalisation, most abortions in India are still performed under technically illegal circumstances. In the Indian situation, the illegality is due to the lack of government certification or proper reporting by the provider or the facility.
Recent papers have suggested that most illegal abortions are carried out by unqualified providers, traditional birth attendants or pharmacists, especially in rural areas, and are therefore dangerous in terms of both morbidity and mortality,Citation5 Citation6 Citation7 thus equating illegality with lack of safety. Others have found that many rural women, especially in western and southern parts of India, are seeking abortions from qualified doctors and clinics, many of which are not certified.Citation3, Citation8, Citation9 The Abortion Assessment Project India, carried out in six different states, recently found that nearly two-thirds of private abortion providers in both registered and unregistered facilities have the requisite training to provide abortion services.Citation10
Methodology and participants
Our research, carried out in 2001—02, examined women’s access to abortion services, and the characteristics of those services, in a rural district (Dharmapuri) in Tamil Nadu. Dharmapuri is a less developed district, with a population of approximately 2.8 million inhabitants. Health and demographic indicators are quite low compared to most other parts of Tamil Nadu. The district has a contraceptive prevalence rate of 45%, compared to around 55% for the state as a whole. The infant mortality rate is 50 per 1,000 live births (all-Tamil Nadu = 40) and female literacy is 45%.Citation11 Citation12 Citation13
Married women who had had abortions within the previous six months were identified and interviewed with the help of village health nurses (VHNs). VHNs maintain records of all married, pregnant women in their service areas. Previous research revealed that the VHNs had excellent knowledge of abortion-seeking among village women, as well as of abortion providers, as they frequently assist women to get abortions.Citation9 A total of 97 women were recruited from villages in the service areas of four primary health centres (PHCs). The locations ranged from peri-urban to remote.
Initially, the women were identified by the VHNs in their service villages and asked if they would consent to be interviewed by the visiting researcher. After the VHN had obtained informal consent, the interviewer (first author) explained the project to each woman and that participation was entirely voluntary and could be terminated at any time. The in-depth, partially structured interviews usually lasted about 90 minutes. In some cases a second meeting with the woman was arranged to fill in further details about abortion decision-making and its consequences.
The 97 women were from families whose socio-economic status ranged from a few wealthy landowning families to poor, landless agricultural labourers. In approximately one-third of cases, the family owned some agricultural land. Twelve of the women were engaged in income-generating activities such as running a small restaurant, tailoring and rope-making. More than half were literate (53), and one-fourth had higher secondary education of nine years or more. They appeared to be representative socio-economically of the population of the district generally.Citation13
The 97 women had gone to a total of 36 different abortion providers, which included the district and sub-district hospitals, a few primary health centres (PHCs) and a wide range of private facilities. In order to assess the qualities of the abortion providers, we wrote the names of each of the 36 providers/facilities on separate index cards and asked 18 VHNs, who acted as key informants, to sort them into categories of high, medium and low quality of care, with particular attention to safety, as evidenced in post-abortion complications. We chose VHNs as key informants because their work puts them in frequent contact with different public and private health facilities and because they are well informed about post-abortion complications experienced by women. Most of the VHNs categorised the providers into five or six levels of quality. Although we asked them to rate the providers in terms of safety, they also mentioned other qualities, such as having “good hands” or many years of experience or good training. They also described the different types of facilities and equipment.
We did not inventory all the abortion providers in the district, but according to our key informants, our sample covered the full range of different types of provider in the area, although the more remote parts of the district were not represented. Based on the aggregated ratings from the 18 VHNs, we constructed a rank ordering on a five-point scale from highly qualified and safe (=1) to unqualified and unsafe (=5). After the VHNs had completed their ratings, they were asked to give reasons for their judgements in each case. Most of their descriptions were very detailed, showing that they were indeed familiar with the personal characteristics, training background and practice facilities of the providers. To simplify data analysis and presentation, we grouped providers into three categories: highly qualified and safe (19), intermediate (9) and unqualified and unsafe (8).
The highly qualified, safe abortion providers
Nineteen of the 36 abortion facilities fell into the category of highly qualified and safe, but none of the government facilities were included in this top category. Their average rankings ranged from 1.33 to 2.71 on the five-point scale. All of these providers had medical degrees, and most were gynaecologists. Almost all of them worked in private hospitals with 15—30 beds, modern equipment, staffed by specialised medical doctors including gynaecologists, anaesthetists, surgeons and radiologists. These facilities provided childbirth services, family planning and other reproductive health services. Most had X-ray machines, and 12 had ultrasonography equipment. Their charges were also high. The usual fee for a first trimester abortion at the time of the research ranged from Rs.800—1000 (US$20). (The typical woman wage labourer in the district earned only about Rs.1000—1200 per month at the time of the study.) The cost was much higher if the pregnancy was advanced or if the woman was unmarried. In most cases D&C was the procedure used, which is typical throughout India.Citation14
Two women described two such facilities as follows:
“The operating theatre is very big, equipped with powerful lighting, and the table is very big and the sheets are very clean. There was an anaesthetist and I could see so much fancy medical equipment inside the theatre. The doctor was very polite and the theatre staff are equally good and kind to the patients. Doctor “kku rasianna kai” (The doctor has lucky hands). I was asked to change my clothes and they provided me with a neatly pressed hospital gown that I had to wear before I got on the table. The theatre surgeon was very polite and kind. Although I got restless waiting for a long time, still I was pleased with the overall treatment that was given to me. I did not have any complications after getting abortion and sterilisation.”
“The doctor is extremely polite and does not discriminate among patients. I like this doctor. I went to her for the first time for my childbirth. She is very impressive and gentle in treating people.”
Intermediate abortion providers
The intermediate category included some government facilities, as well as several private doctors among the nine. One or two large private hospitals similar to the facilities in the top category were also included. Other private facilities were much smaller and poorly furnished, with less equipment and resources. One PHC, a sub-district hospital and the district hospital were rated in this middle range, all certified for providing abortion services. The private providers in this category all had MBBS training, but none of them were certified to do abortions by the government, except for one large private hospital in the neighbouring district. The VHNs described the intermediate government facilities as not very clean and causing frequent post-abortion complications, and said the personnel were often impolite or even abusive towards women.
The private providers in this category were not totally unqualified, but were described by the VHNs as not having “good hands”. In general, the small clinics in this group charged much less than the high quality hospitals, around Rs.300—400 for first trimester abortion. These clinics also conducted deliveries, insertion and removal of IUDs and treatment of minor ailments, in addition to abortions. A VHN described one of the lowest rated of the intermediate providers as follows:
“SM is a male doctor and has a medical degree (MBBS). He has a very small clinic centrally located in [town]. There is only one bed and a wooden curtain to maintain visual privacy. He conducts childbirths and also abortion… He has a small name board on a rusted metal sheet. I do not refer my abortion cases to this doctor but women from [village] go to him although he causes complications because the distance from the village to his clinic is hardly 7 kms. There are frequent buses to the town… the bus fare is only Rs.10 both ways. Secondly, it is a market place for meat, clothes, food, grains, etc. Women have the pretext of going to the market to buy things for the house and also get an abortion. Poor people can easily afford [his fees]. He has a full-time nurse to assist him with abortions.”
Women’s explanations of why they chose particular providers were often accompanied by negative comments about the government facilities.
Even the District Hospital was ranked only as intermediate quality
The District Hospital is supposed to be the highest level, best-equipped government medical service in the district. Normally many women would be expected to go there for their abortions, particularly the poorest, because the services are supposed to be free of cost. The VHNs described a number of problems with the District Hospital, however, and some were quite emotional about it. Some VHNs gave it ratings of “3” but several, such as these two VHNs, rated it in the lowest category:
“The hospital people openly demand money for providing any service. I have taken some of my abortion cases and the staff abused the women in my presence. Imagine if they were to go alone how they would be treated. The doctors are negligent and cause complications and their follow-up care is very poor. In the past many poor women who could not afford to pay went to the government hospital and within 24 hours they developed complications. When they went back to the provider they were very slow in giving admission, and made the patients wait. We are fed up with the government hospital.”
“The services are no good and therefore women do not like this facility. More go to the private facilities. Women do not seem to have any faith in the government institutions. We are afraid to refer abortion cases there because the doctors are not responsible and the poor women do not know how to assert their rights. In the past some cases went there and ended up with complications. When we went back to the provider she said that she did not do the abortion and was blaming the other gynaecologist.”
Several of the women in the villages made similar statements about the District Hospital in explaining why they would not go there for abortions or other reproductive health services.
Unqualified and unsafe abortion providers
The bottom end of the spectrum of abortion services included a medical doctor, a government facility, a pharmacist and several unqualified, untrained practitioners. Some of these providers had very small clinics in congested marketplaces or in crowded interior lanes. Except for two providers in this group, all were using allopathic methods, particularly dilatation and curettage (D&C) with medications such as prostaglandin gel and antibiotics. The facilities were considered unhygienic by the VHNs, who said the practitioners lacked both qualifications and skills, and had minimal medical experience or training. The most usual pathway to the profession seemed to be apprenticeship to another abortionist.
Malathi (pseudonym) was a typical example; she was a well-known abortionist, and was thought to cause many serious post-abortion complications. She was educated only to the 6th or 7th standard, and had been doing abortions in a middle-sized market town for more than 20 years. She had acquired the skills to do D&C by assisting a medical doctor. After he got very old and gave up his practice, Malathi took over his clinic and continued providing services. Many women, particularly from the poorer rural villages, went to her, and she was doing seven or eight abortions a day. Her fees were very low compared to the qualified private doctors, only Rs.200—300 (US$6) for first trimester abortion. Generally women who could not afford higher fees went to her. She was believed to have caused at least three deaths in the past five years. Eight of the women we interviewed had gone to her for abortions, several of whom suffered moderate to serious post-abortion complications.
Traditional abortion providers
Two of the providers in our sample carried out abortions using traditional methods and preparations. One of them used the stem of a chicken feather to apply some kind of vegetable material into the cervix to induce abortion. The other used the traditional “stick abortion” using yerukkam kutchi (a wild plant, calatropis gigantia), which exudes a white, milky sap that is an effective irritant and abortifacient. In the past “stick abortions” were common throughout much of India,Citation2, Citation15 but the VHNs in Dharmapuri and other areas in Tamil Nadu report that this practice has almost died out.Citation9, Citation16
Women’s decision to seek abortion and selection of provider
In the majority of cases the 97 women were the main decision-makers regarding their own abortions, and 20 of them went on their own to have their pregnancies terminated without consulting their husbands or other family members. This is contrary to widespread descriptions of women’s subservience and lack of decision-making powers in Indian households. The women we interviewed generally felt that the husband should be consulted, and his approval obtained for getting an abortion. Nonetheless, many of them took the initiative to discuss the pregnancy and arrange the abortion.
Of the 97 women, 75 had gone to highly qualified and safe (47) or intermediate (28) providers while 22 had utilised the unqualified or unsafe providers, of whom four had gone to the traditional practitioners. One of these four women was the wife of an extremely poor cobbler; the other three appeared to be marginalised, illiterate women with little knowledge of the district’s health facilities.
Extent of post-abortion complications
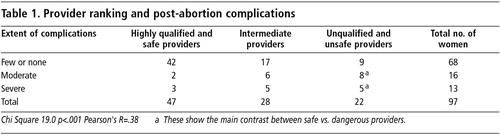
We asked the women about any health problems they experienced immediately after their abortions and grouped the complications described into three categories: serious, moderate and few or no complications. As shown in , about two-thirds of the women reported few or no problems following abortion. We rated the problems as moderate if the woman reported continued bleeding, some fever and other symptoms involving at least a day of bed rest. In these cases, some women took medications (including antibiotics and analgesics), but did not go to a medical practitioner. We rated the complications as serious if the woman reported severe bleeding, fever, pain and other symptoms that lasted seven days or more, requiring one or more visits to a medical practitioner. In most of the serious cases, the abortion was incomplete. Some women were of the opinion that the providers (especially the intermediate and low-rated providers) purposely did this, so that the woman would have to come back and pay more for removal of the products.
It is, of course, impossible to judge the actual degree of morbidity based on women’s self-reports, but the reported level of complications is unacceptably high compared with industrialised countries, where the rates of serious complications are generally around 1% and rates of any reported complications are 10% or less.Citation17
Which providers caused more complications?
The data in are presented as a triangulation, or cross-checking, between the ratings from VHNs and the experiences of the women interviewed. These demonstrate that the abortion providers who were rated as unqualified and unsafe by the VHNs caused much higher rates of post-abortion complications.
The data in demonstrate that the VHNs were well-informed concerning the various abortion providers, as their assessments are congruent with the frequency of post-abortion problems reported by the women for the different providers.
It is worth noting that most of the government facilities were rated in the intermediate category, and half the women who went to government facilities reported suffering moderate or severe post-abortion complications (data not shown).
Women’s knowledge of abortion providers and awareness of the risks of abortion
Many of the VHNs reported that women in their villages were very well informed about local abortion providers. However, the cost of getting an abortion from the well-equipped and qualified providers was a serious challenge to family resources. Nonetheless the majority of women (and their husbands) were willing to pay the costs, even in cases where they were forced to get a loan from relatives or other sources. The decision to spend money on private, higher-cost providers was usually explained in terms of the lower risk of post-abortion complications.
Many women thought that abortion should preferably take place no later than 45 days LMP. Almost all of the women were aware of the higher risk of complications with late terminations. They were also acutely aware that providers charged higher fees the more advanced the pregnancy was.
Three-quarters of the women in our sample had their abortions in the first trimester, a figure that is similar to findings of other studies in India.Citation3, Citation18 On the other hand, in recent research in Rajasthan, Iyengar and IyengarCitation14 reported that 88% of their abortion patients were under 12 weeks pregnant. Although some people have questioned rural women’s ability to recognise the early stages of pregnancy, research in India and elsewhere has indicated that women are generally quite accurate in their estimates of length of pregnancy.Citation19
Discussion and conclusions
This study has concentrated on rural women because they are often described as having less access to safe abortion services, compared with their urban counterparts. It also focused entirely on married women. The proportion of unmarried women among abortion seekers in India is relatively small, but they are particularly vulnerable to dangerous abortions from unqualified providers because of their concerns about cost and secrecy, the tendency to delay seeking services and the unwillingness of qualified providers to help them.Citation4, Citation20 More attention needs to be paid to their situation.
The data from our study show that, contrary to many pessimistic portrayals, rural married women in this district of Tamil Nadu have access to relatively safe abortions from a variety of qualified providers. In about half of the cases the providers were women gynaecologists with well-equipped private facilities. Both VHNs and the women gave high ratings to these providers in matters of safety and quality of care. However, more than half of private abortion providers were not registered for abortion services with the Tamil Nadu government.
Our data are in line with those from the Abortion Assessment Project—India, which also found that large numbers of abortions take place in facilities that are not registered with the government,Citation21 and that there were only small differences in the technical and infrastructural aspects between certified and non-certified facilities.Citation3 These data, taken together, strongly suggest that a considerable proportion of illegal, unreported abortions are conducted by qualified, relatively safe providers who are nonetheless still widely using D&C, an outdated abortion technique, thus perpetuating higher than necessary rates of post-abortion complications.Citation21
The numbers of private doctors, clinics and hospitals in the district rose from 148 at the end of the 1980s to 287 in 2001 (Personal communication, Assistant Director of Public Health, Dharmapuri District, 2001). Forty of those private facilities were medium to large hospitals, all of which provided abortion services.Citation12 This increase in the number of private doctors is part of a broader trend of increased medical services in Tamil Nadu.Citation9, Citation22 Footnote*
A second factor affecting women’s increased knowledge of and access to abortion services is the large increase in institutional childbirths, which by 1999 had reached 60% among rural families in Dharmapuri.Citation13 This has added to women’s familiarity with available health facilities. The women’s knowledge of abortion facilities was also evidenced by the fact that many of the women in our sample travelled considerable distances for their abortions, including several to neighbouring districts or over the state border to Karnataka.
Unfortunately, government facilities have not developed the same levels of quality of services as found in the private clinics, because of lack of equipment, poor facilities and other factors. The negative aspect of our findings includes the fact that government services were given quite low ratings by most of our informants, in terms of their treatment of patients and the likelihood of post-abortion complications. The perception of poor quality of care in government PHCs and hospitals was a major reason why most women chose private practitioners if they could afford the costs. These findings are similar to abortion research results in other parts of India. Citation4 Citation9 Citation14 Citation21
Hospital recovery room, Latur, India, 2002

Recommendations
Our data suggest the following changes in the provision of abortion services in both the public and private sectors in this district, which are relevant for most parts of India:
| • | The continued high rates of post-abortion morbidity will not be reduced until modern, safer abortion technology is widely adopted. The continued use of D&C for abortions by both government and private doctors should be strongly discouraged, and the much safer vacuum aspiration techniques and medical abortion should be widely adopted. | ||||
| • | Government facilities at the district hospital level and among the better equipped PHCs should improve their services in terms of better communication with patients, confidentiality and counselling, as well as in technical matters, which can be done without large additional funding. | ||||
| • | As has been suggested in many recent policy statementsCitation24 the process of certification of private clinics should be transparent, timely and enforceable, so that qualified practitioners and facilities are brought into a regulated system of abortion services that includes regulation of fees, to ensure that all women can afford to have a safe abortion. | ||||
| • | Unqualified and unsafe practitioners should gradually be forced to stop providing abortion services through careful application of existing laws. It is our hypothesis that in most parts of India, women can gain access to qualified abortion facilities, or would be able to do so if more government facilities were actually to provide the services. | ||||
Acknowledgements
This paper is based on the doctoral dissertation of the first author, who was funded by scholarships from the University of Melbourne. She is grateful to the Key Centre for Women’s Health in Society for support given throughout her doctoral work. The authors also thank the Tamil Nadu Government Ministry of Health and Family Welfare for granting permission to carry out this research. Special gratitude is expressed to the women of Dharmapuri district, who shared their intimate reproductive histories during the fieldwork. Sincere thanks also to the VHNs and other community health personnel, who were forthcoming with detailed information about abortion providers and other reproductive health services in the district.
Notes
* A bulletin from the Directorate of Medical and Rural Health Services estimates that in 2004 there were approximately 30,000 private practitioners in Tamil Nadu, exclusive of government doctors.Citation23
References
- Government of India. The Medical Termination of Pregnancy Act. Act No.34 of 1971, Acts of Parliament, 1971 Ministry of Law, Justice and Community Affairs, 1973.
- S Chandrasekhar. India’s Abortion Experience. 1994; Allen and Unwin: London.
- Abortion Assessment Project — India. Key Findings. February 2004. At: www.cehat.org/publications. Accessed June 2004.
- B Ganatra. Abortion research in India: what we know and what we need to know. R Ramasubban, S Jejeebhoy. Women’s Reproductive Health in India. 2000; Rawat Publications: New Delhi, 186–235.
- ME Khan, S Barge, N Kumar. Abortion in India: current situation and future challenges. S Pachauri. Implementing a Reproductive Health Agenda in India: The Beginning. 1999; Population Council: New Delhi, 507–529.
- ST Mathai. Making abortion safer Journal of Family Welfare. 43(2): 1997; 71–80.
- Passano P. Legal but not available: the paradox of abortion in India. Manushi 2002; 126. At: www.indiatogether.org/manushi. Accessed September 2003.
- Joshi A, Dhapola M. Male involvement in seeking abortion services in rural Gujarat. Paper presented at Meeting of the South Asian Initiative in Reproductive Health Research. Colombo, December 1998.
- L Ramachandar, PJ Pelto. The role of village health nurses in mediating abortions in rural Tamil Nadu, India Reproductive Health Matters. 10(19): 2002; 64–75.
- Abortion Assessment Project — India. Synthesis of multi-centric facility study. At: www.cehat.org/publications. Accessed June 2004.
- Dharmapuri District. Family Welfare Programme. General Information Book. 2001.
- Dharmapuri District Family Welfare Programme. General Information Book. 2002.
- Gandhigram Institute of Rural Health and Family Welfare. Rapid Household Survey: RCH Project. Dharmapuri. Survey report prepared for the Ministry of Health and Family Welfare, New Delhi, 1999. (Unpublished).
- K Iyengar, S Iyengar. Elective abortion as a primary health service in rural India: experience with manual vacuum aspiration Reproductive Health Matters. 10(19): 2002; 54–63.
- R Chhabra, C Nuna. Abortion in India: An Overview. 1994; Ford Foundation: New Delhi.
- Lakshmi R, Barge S, Kumar N, et al. Situation Analysis of Medical Termination of Pregnancy (MTP) Services, Tamil Nadu State. Report by Centre for Operations Research and Training, Baroda, 1997. (Unpublished)
- FC Greenslade, AH Leonard, J Benson. Manual vacuum aspiration: a summary of clinical and programmatic experience worldwide. 1993; IPAS: Carrboro NC.
- Ganatra BR, Hirve SS, Walawalkar S, et al. Induced abortions in a rural community in western Maharashtra: prevalence and patterns. Presented at Workshop on Reproductive Health in India: New Evidence and Issues. Pune, March 2000.
- C Ellertson, B Elul, B Winikoff. Accuracy of assessment of pregnancy duration by women seeking early abortions Lancet. 355: 2000; 877–881.
- B Ganatra, S Hirve. Induced abortions among adolescent women in rural Maharashtra, India Reproductive Health Matters. 10(19): 2002; 76–85.
- Barge S, Khan WU, Narvekar S, et al. Accessibility and utilization. Abortion: A Symposium on the Multiple Facets of Medical Termination of Pregnancy, December 2003. At: www.cehat.org/publications. Accessed June 2004.
- Visaria L. Innovations in Tamil Nadu. Seminar: The Monthly Symposium. At: www.cehat.org/publications. Accessed June 2004.
- Directorate of Medical and Rural Health Services. Activities on Pre-Natal Diagnostic Technique (Regulation and Prevention of Misuse) Act 1994. Tamil Nadu. Accessed June 2004.
- Hirve S. Policy and practice. Paper presented at: Abortion: A Symposium on the Multiple Facets of Medical Termination of Pregnancy. December 2003. At: www.cehat.org/publications. Accessed June 2004.