Abstract
Although more than one method of abortion has been available for many years, in most countries the provider chooses the method and may be skilled in one method only. This paper discusses choice and acceptability of medical abortion from the perspective of both women and abortion providers and argues that choice of method is important for both. Safety, efficacy, number of visits, how the method works, how long it takes for the abortion to be complete and cost all affect acceptability. Medical abortion is considered more natural because it happens in women's own bodies and can take place at home before nine weeks of pregnancy; surgical abortion with vacuum aspiration is simple and over quickly. Unless the costs of both methods are similar, however, women and providers will tend towards whichever is the cheaper option, limiting choice. Medical abortion is effective from when a woman misses her period through 24 weeks of pregnancy, and more women and providers need to be made aware of this. In legally restricted situations, complications tend to be less serious and easier to treat with early medical abortion than after unsafe invasive methods. Ideally, both medical and surgical methods should be available, but each can be provided without the other.
Résumé
La plupart des pays disposent de plus d'une méthode d'avortement depuis des années ; pourtant, le praticien choisit la méthode et n'est parfois formé que pour une seule méthode. Cet article examine le choix et l'acceptabilité de l'avortement médicamenteux du point de vue de la femme et du praticien, et avance que le choix de la méthode est important pour les deux. La sécurité, l'efficacité, le nombre de visites, le fonctionnement de la méthode, le délai avant que l'avortement ne soit complet et le coût sont des facteurs influençant l'acceptabilité. L'avortement médicamenteux est jugé plus naturel car il se produit dans le corps de la femme et peut avoir lieu à la maison avant la neuvième semaine de grossesse ; l'avortement chirurgical par aspiration est simple et vite terminé. moins que le coût des deux méthodes ne soit semblable, les femmes et les praticiens préfèrent l'option la moins chère, limitant le choix. L'avortement médicamenteux est efficace de la septième à la vingt-quatrième semaine il faut que beaucoup de femmes et de praticiens l'apprenent. En cas de restrictions légales, les complications de l'avortement médicamenteux précoce tendent à être moins graves et plus faciles à traiter, même si les femmes ont pris elles-mêmes les médicaments, que celles des méthodes invasives non médicalisées. Dans l'idéal, les deux méthodes devraient être disponibles, mais chacune peut être proposée sans l'autre.
Resumen
Aunque por muchos años ha existido más de un método abortivo, en la mayoría de los países quien elige el método es el prestador de servicios, posiblemente capacitado para efectuar un sólo método. Este artículo trata la elección y aceptación del aborto con medicamentos, desde el punto de vista tanto de las mujeres como de los prestadores de servicios de aborto, ya que el método elegido es importante para ambos. La seguridad, la eficacia, el número de consultas, el modo de acción del método, el plazo en que demora completarse el aborto y el costo, todos estos afectan la aceptación. El aborto con medicamentos se considera más natural ya que ocurre en el cuerpo de la mujer y puede realizarse en el hogar antes de la novena semana de embarazo; el aborto quirúrgico con la aspiración endouterina es sencillo y rápido. Sin embargo, a menos que los costos de ambos métodos sean similares, las mujeres y los proveedores tienden a limitar sus opciones al escoger la opción menos costosa. El aborto con medicamentos es eficaz entre las 7 y 24 semanas de embarazo. embarazo y más mujeres y prestadores de servicios tienen que saberlo. En situaciones legalmente restringidas, las complicaciones tienden a ser menos graves y más fáciles de manejar en el aborto con medicamentos temprano, aun si las mujeres usan los fármacos por su cuenta, que después de métodos invasivos inseguros. Lo ideal sería que hubiera métodos tanto médicos como quirúrgicos disponibles, pero cada uno puede realizarse sin el otro.
For several decades now, a growing range of contraceptive methods has been available and choice and acceptability of method are considered values in themselves. With abortion, choice and acceptability of method have received much less priority. Although more than one method of abortion has been available for many years now,Citation1Citation2 in most countries it is still the provider who chooses the method and providers are often not knowledgeable or skilled in more than one method. In many cases, they rely on outdated methods. Medical abortion is rapidly affecting this picture, however.
In most countries, the transition to services in which both surgical and medical abortion are available is moving far more slowly than it should be, due mainly to restrictive laws, policies that have not kept up with best practice, lack of training for providers, provider unwillingness to re-train and inavailability of vacuum aspiration equipment and/or medical abortion drugs. Even where abortion remains legally restricted, however, women are getting access to medical abortion pills, mainly misoprostol, and if necessary using them without clinical support. Although this situation is far from optimal, it has meant that even poor women in these countries no longer have to accept more dangerous invasive methods, resulting in a reduction in mortality from unsafe abortions.Footnote*
This paper focuses on choice and acceptability issues related to medical abortion from the perspective of both women and providers. It is based on a sample of recent papers found on Medline on these issues from a range of countries, both developed and developing, and information presented at a conference in October 2004 on medical abortion, organised by the International Consortium for Medical Abortion (ICMA).Footnote*
Medical abortion: choice of regimen
One of the most confusing aspects of medical abortion is that so many different regimens have been tried and used, more or less successfully. In fact, more than one regimen may be effective at a particular stage of pregnancy. In addition, due to lack of information, there has been a lot of experimentation, both on the part of clinicians in research settings and clinical practice, and by women self-administering misoprostol. The doses and regimens recommended in the UK Royal College of Obstetricians and Gynaecologists National Clinical Guidelines 2004 are based on a review of the literature and took into account efficacy, adverse effects and cost.Citation2Footnote*
In legally restricted settings, where misoprostol is used alone, many women purchase the drugs over the counter or get them from a provider who may or may not be up to date on the best regimens. In Latin America, the most common regimen women are thought to use, according to participants at the ICMA conference in 2004, is 400mcg orally and 400mcg vaginally, sometimes with repeat doses, but some women are said to have used one 200mcg tablet every hour until the abortion is complete. There may be a wider range of efficacy with such different regimens.
Medical or surgical: aspects of choice and acceptability for women
Choice of abortion method is important for both women and providers. Medical abortion can be used from the time a woman misses her period until 24 weeks LMP. Medical abortion can make abortion, earlier, more accessible, safer, less traumatic, less medicalised and less expensive whether abortion is legal or legally restricted. When offered the choice between medical abortion and vacuum aspiration, most women express an initial preference for one or the other method. In a Norwegian study comparing the two methods up to nine weeks of pregnancy, for example, 69% of the 226 participating women expressed a preference.Citation4 In a study in Scotland, prior to abortion at 10-13 weeks of pregnancy, 80% of women had a preference, of whom 72% preferred medical abortion while 28% chose aspiration abortion with general anaesthesia. Those who had had a preference prior to abortion were also more likely to say they would choose the same method in future: 70% of those who had medical abortion and 79% who had surgical abortion said they would opt for the same method in future.Citation5
The range of women's reasons why medical abortion was acceptable can be summarised from a study in the US of women from different ethnic backgrounds. US Asian women were more than twice as likely as others to choose medical abortion because they believed it was safer. White women were twice as likely to select it because they considered it more natural. More educated women wanted to avoid surgery. White and African-American women and women with more education felt significantly more comfortable taking one or both of the drugs at home than aborting in the clinic. Nearly all groups found the method highly acceptable, with few differences in overall satisfaction, willingness to choose it again or recommend it to others.Citation6
In studies comparing the acceptability of the two methods after early abortion, most women were satisfied with the procedure they had chosen and most (though not all) would choose it again and recommend it to others. In Germany, Sweden, the UK, Norway and Finland, the acceptability of medical abortion with mifepristone and misoprostol has been very high.Citation7Citation8Citation9Citation10Citation11 In one US study among 326 women who had had either surgical or medical abortions, if an abortion was required in future, 41.7% of those who had had surgical abortions said they would opt for medical abortion, whereas only 8.6% of those who had had medical abortions said they would choose surgical abortion.Citation12 Similarly, at a one-week follow-up visit, 75% of 28 adolescent girls in the US who had had a medical abortion found the procedure acceptable; that proportion increased to 96% by the four-week visit when they were sure that it had been successful and that they were all right.Citation13
It's more natural
An important reason why medical abortion is preferred is that it is seen as more “natural” because it happens entirely in the woman's body, whereas aspiration abortion may be preferred because it is carried out by a provider and the woman need do nothing.
Women like the fact that with medical abortion, even if they have to stay to abort in the clinic after taking misoprostol, they are dressed and sitting up, whereas with aspiration abortion they are lying down and exposed, with their feet in stirrups. The latter is not problematic with a sympathetic provider, but not all providers are sympathetic and many women have experienced ridicule, insults and taunting when they seek abortions, as reported recently in Argentina,Citation14 leaving them unwilling to repeat the experience if there is another choice.
Avoidance of a surgical procedure and anaesthesia
For many women, the avoidance of a surgical procedure, even a simple aspiration procedure, and of anaesthesia, especially where general anaesthesia is still being used, are central reasons why medical abortion is preferable. On the other hand, there are women who do not want to experience the abortion at all, for whom aspiration abortion with general anaesthesia is their first choice, in spite of the added risks of general anaesthesia. Most of the time, however, general anaesthesia is not necessary for vacuum aspiration abortion up to 15 weeks except, for example, in some cases of fetal malformation or if the woman has complications. It is still used mainly by providers who are not used to interacting with a woman who is awake while they are doing the abortion.
Safety and efficacy
Two of the most important aspects of any abortion procedure are its safety and efficacy. Aspiration abortion after seven weeks of pregnancy has the advantage that it rarely needs repeating. Medical abortion with mifepristone and misoprostol also has a low failure rate and can be provided very early, as soon as a woman has missed her period, which is one of its biggest advantages.
Up to seven weeks, medical abortion is usually more effective than early aspiration, which can be incomplete because the gestational sac can be missed. The risk of failure with early aspiration abortion before seven weeks is around 2.3 per 1,000 procedures.Citation2 The complete abortion rate with early medical abortion varies between studies but was as high as 98% in a large case series report of 4,132 women up to nine weeks of pregnancy.Citation15 Medical abortion is more commonly reported to be 94-96% effective, with 3-5% incomplete abortions and 1-3% ongoing pregnancies with the recommended dosages and regimens. Women with an ongoing pregnancy must have a surgical evacuation.
Whatever the setting, women choosing medical abortion need to be aware that 2-6 out of 100 may need an aspiration procedure at follow-up, either because the pregnancy is ongoing or because of bleeding that is heavier or goes on longer than is tolerable. For some, this makes the method unacceptable. For others, medical abortion has other characteristics that still make it preferable.
From 2001 through the first quarter of 2004 in the US, 95,163 mifeprisone-misoprostol abortions were provided by Planned Parenthood Federation clinics. Overall, only 2.2 per 1,000 women (95% CI 1.9-2.5) experienced a complication, most commonly heavy bleeding. Mortality was estimated to be 1.1 per 100,000, based on one death (95% CI 0.3-5.9).Citation16Citation17
Globally, up to 2005, some 22 million women in China and four million women in the rest of the worldCitation18 have had safe medical abortions. The fact is that abortion is one of the most common and also one of the safest medical procedures that exists.Citation2
Blood loss and the need for surgical back-up
Whether an abortion is surgical or medical, uterine blood loss is the same. However, women experience this as a difference because with the surgical method most of the blood and the products of pregnancy are suctioned out, whereas medical abortion is like having a heavy menstrual period with the bleeding tapering off after the products are expelled. Blood loss is then about the same with both methods, but with medical abortion bleeding tends to last more days than with aspiration abortion.Citation19
With most women the bleeding takes its course and stops; a small number ask for an aspiration procedure to finish it. Excessive bleeding (haemorrhage) does happen in a small number of women.Citation20Citation21 Bleeding is considered excessive if the blood soaks more than two sanitary pads per hour for two or more hours. Aspiration (or curettage) is necessary to stop excessive bleeding, but for treating incomplete abortion, where bleeding is not excessive, it may not be medically necessary as often as it is used. Some clinicians recommend trying an additional dose of misoprostol first. Research suggests that as medical abortion providers gain experience, they are less likely to intervene surgically, and when they do, it is later in the process when actual need is higher.Citation22Citation23
Pain and other adverse effects
Pain is a temporary effect of both medical and surgical abortion. With first trimester pregnancies, there is usually pain during the aspiration procedure, for which local anaesthesia is sufficient though in some clinics general anaesthesia is still used. With medical abortion, there is usually pain from uterine contractions for several hours, stronger than menstrual cramps, usually strongest in the 3-4 hours after the misoprostol is administered, for which analgesic tablets are usually sufficient.
In one review of women having a medical abortion up to 22 weeks of pregnancy with mifepristone followed by repeated doses of misoprostol, the analgesia requirement was significantly higher for women of younger age, higher gestation, longer induction-to-abortion interval and with increased number of misoprostol doses used, while women with a previous live birth were significantly less likely to require analgesia. Of the total 4,343 women included in the review, 72% required analgesia and 28% did not. Of the 72% who did, 97% used oral analgesia, most of the rest required opiates.Citation24
The most common adverse effects reported by patients after taking misoprostol in one study among 376 women up to 49 days LMP, were pain or cramps (93.2%), nausea (66.6%), weakness (54.7%), headache (46.2%) and dizziness (44.4%). These effects usually go away within several hours. Overall acceptability of the regimen was high in this study, with 63.3% of women reporting that it was very satisfactory and an additional 23% reporting that it was satisfactory.Citation25
Home vs. clinic
Privacy and confidentiality are easily achieved and easily violated with both medical and surgical methods of abortion, depending on how the individual provider and health system treat women. Some women want their partner, a member of their family or a friend to be present. Others prefer to be on their own and for no one else to know what is happening.
Most studies in which women have had a choice between home and clinic use with medical abortion up to nine weeks have expressed a strong preference (80% or higher in most studies) for using the misoprostol and aborting at home.
“I liked the tablets. See, I did not need to stay in the hospital. With curetting I would have spent two days there. I told my mother-in-law I was going to the market. I did not abort at the hospital although I waited for 3 hours. I was scared, would mother-in-law come to know? How many days I bled.... I was going to the toilet every hour to check. See, we don't have our own toilet. I felt embarrassed. But it happened when she was out. A little pain was there but that much is to be tolerated. Whatever you would have done, pain is always there. Everything has turned out well. I am very happy now. I will definitely use this method again.” Citation26
In a study among 1,601 women in eight sites in Vietnam, for example, home administration of misoprostol was preferred by 87% of the women.Citation27 In Tunisia, among 321 women in four sites, 96% had a complete abortion, and women expressed a strong preference for home use of misoprostol, because it was more confidential (34%), easier (28%) and required fewer clinic visits (28%).Citation28
Home use of misoprostol should always be an option up to nine weeks, but some women may be uncertain whether they can cope and would prefer to stay in the clinic. In the UK, where home use of misoprostol is not yet available, a study in England and Scotland asked women who had had a medical abortion in a hospital clinic whether they felt they could have coped at home with the bleeding and pain involved. 71% of 320 women said there was nothing that happened during the abortion that they would have been unable to cope with at home though fewer, 36% of 342, said they would have opted to use misoprostol at home, had that choice been available.Citation29 In a French study where 339 women used misoprostol at home, about 5% phoned the midwife with questions, and 5% went back to their providers for a consultation before their follow-up appointment.Citation20 Access to 24-hour advice by phone for women aborting at home can greatly reduce anxiety.
Some women may have home circumstances that would make home use of misoprostol highly problematic. For those who do not want anyone at home to know they are having an abortion, e.g. young unmarried women in many cultures, the privacy of being in the clinic is paramount. Furthermore, the household situation - e.g. if there is no indoor toilet or running water, or no menstrual pads available - can also make aborting at home difficult.
On the other hand, in legally restricted settings, home use of medical abortion has tremendous advantages in not needing to find a provider and to avoid being reported to the police. The disadvantages can be not knowing what to expect or what constitutes a complication, feeling isolated or afraid or without access to help. Providers in these settings have asked, what can we do to ensure that women use a safe and efficacious dosage? The obvious answer seems to be to get information out to women in any way possible. Overall, the anecdotal information is that women do cope, and do seek help when it is needed, which is why mortality rates appear to be going down.
Time factors
The distance women have to travel to a clinic, how much time off work or away from home they can get, and the number of clinic visits and procedures involved all matter to women, not only because of the time and travel involved but also the cost.
How long the process takes is an important difference between aspiration and medical abortion. Aspiration can be done in 10-15 minutes or less, and where local anaesthesia has been used, the woman need not remain in the clinic for very long at all. This is a big advantage; the abortion is over very quickly. With medical abortion through nine weeks, the woman need only be given the mifepristone pill and be instructed on taking the misoprostol pills at home. For example, 96% of women aborted completely 4.3 hours after they were given misoprostol in an Australian study among 100 women up to seven weeks (dosage 200mg mifepristone orally and 800mcg misoprostol orally).Citation30
Number of clinic visits
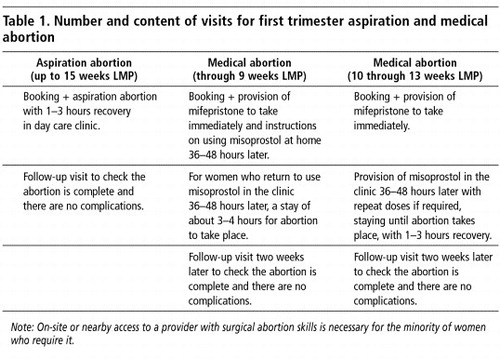
It is often said that the number of visits required for aspiration abortion is less than for medical abortion, but this need not be the case. Both procedures can be over-medicalised and extra visits required unnecessarily. As Table 1 shows, stripped down to the essentials, both types of abortion could involve only two clinic visits in all, or three if misoprostol is taken at the clinic, with additional visits in both cases only if there are complications.
Many clinics and clinicians will not provide either method at the booking visit, however. Apart from “that's just not how we do it” , the only real reason why it might be preferable for a woman to have to come back for an abortion is that she may change her mind and decide she doesn't want the abortion after all. A small but important number of women do do this (David Paintin, obstetrician-gynaecologist, UK, personal communication). However, women could be offered the choice of returning several days later. Those who need more time to think it over will likely opt to come back another day. For the rest, waiting seems unnecessary.
Cost
Misoprostol alone is very low cost and has ease-of-access advantages for developing country settings. According to most of the developing country participants at the ICMA conference in 2004, misoprostol is likely to be used on its own for early medical abortion in settings where registration of mifepristone in the foreseeable future is unlikely. On the other hand, as one clinician from Latin America noted, if women take repeat doses of misoprostol, it may end up being more expensive than one 200mg pill of mifepristone and a smaller dose of misoprostol.
A comprehensive study on the cost of medical abortion in the public health system in South Africa, one of few such studies in a developing country to date, utilised an economic model with alternative management pathways, based on 1,000 patients. Variables included type of provider, primary or secondary level clinic, two or three visits, pregnancy tests, different regimens, home use of misoprostol, pain relief, possible ultrasound, possible phone calls to a counsellor for advice, complete abortion or not, treatment of complications or not, human resources, overheads, training for providers and information materials for women. The main cost drivers were found to be dosage of mifepristone (200 vs. 600mg),Footnote* due to the high price of mifepristone, type of provider involved (doctor vs. mid-level provider), whether the clinic was in a primary or secondary level facility, and the currency exchange rate, which was an issue because the drugs had to be imported.Citation31
Identifying the main cost drivers shows how costs might be reduced without reducing quality of care, e.g. locally produced, generic mifepristone and misoprostol, use of a 200mg dose of mifepristone, provision in primary care clinics with mid-level providers up to nine weeks and mid-level providers in secondary level facilities after nine weeks, with back-up from obstetrician-gynaecologists. A study in India showed that neither hospital beds, operating theatre or ultrasound were required for medical abortion,Citation32 which is important for cost reduction and keeping the process simple. Similar cost reduction studies for surgical methods are needed.
Unless the costs of surgical and medical abortions are broadly similar, many women will feel they need to choose the cheaper option, which limits choice. Where the health service is covering the cost, or health insurance companies control treatment options, similarly, clinicians and managers will also tend towards the cheaper option. However, neither method should be forced on women for this reason.
At the same time, because medical abortion does not require the use of an operating theatre or surgical skills, except in a small minority of cases, thereby drastically reducing the number of clinicians with these skills involved, all health systems may tend towards medical abortion in future. Indeed, in Norway this is already happening according to the obstetrician-gynaecologist who first introduced the method there, who said that at a growing number of clinics women are only offered medical abortion and must specifically request a surgical procedure instead (Prof. Dr. Ole-Erik Iversen, personal communication, February 2005).
For those who believe that women have a right to a choice of abortion method in principle, given how different the two forms of abortion are, such a tendency may be hard to counter unless the cost and human resource parameters of both methods are brought more closely in line with each other.
Second trimester medical and surgical abortion
The large majority of women have abortions before 12 weeks of pregnancy. There are many reasons for delays in seeking and obtaining an abortion in different countries, and some women find themselves in complex circumstances that do not allow for early abortion. The risk of complications and deaths from unsafe abortion methods is higher in the second trimester of pregnancy. However, with safe methods in the second trimester, abortion is still very safe and issues of choice and acceptability still apply.
Vacuum aspiration is a straightforward procedure up to 15 weeks of pregnancy. In contrast, dilatation and evacuation (D&E), the surgical method used from 16-28 weeks of pregnancy under general anaesthesia, requires excellent skills. Most providers do not have the skills to do D&E, however, as they do not see enough case or are simply not willing to learn. In an attempt to randomise women to D&E or medical abortion in a US setting where D&E was the norm, only 18 of 47 eligible women were enrolled, as the other 29 women preferred D&E. Compared with D&E, mifeprisone-misoprostol abortion caused more pain and adverse effects, although none was serious.Citation33 In settings where D&E is not available, which are by far the majority, medical abortion is still far better than older, riskier methods.Citation1
Medical abortion after 13 weeks LMP can be managed by a trained mid-level provider under the supervision of an obstetrician-gynaecologist or other physician, and has greatly improved in recent years with mifeprisone-misoprostol. It takes far fewer hours to abortion than in the past when other prostaglandins were being used alone. In one study, the median induction-to-abortion time was less than six hours for parous women and eight hours for nulliparous women, and more than 70% of the women went home the same day.Citation34 Of 999 women at 13-21 weeks of pregnancy in another study in Scotland, two women aborted after administration of mifepristone and 97.1% aborted successfully within five doses of misoprostol. Surgical intervention was carried out for 8.1%. Women with no previous pregnancy, no previous live birth and at 17-21 weeks of pregnancy required more misoprostol. Younger women and women with a previous live birth were more likely to have a successful abortion. The induction-to-abortion interval was significantly longer with increasing gestation, increasing age and no previous live birth. Surgical intervention was more likely to be required with increasing age.Citation35
Choice and acceptability: provider and health system perspectives
Medical abortion may help to overcome negative provider attitudes because the provider does not have to do the abortion. For providers, it is a matter of giving information, dispensing pills, monitoring progress and giving support, with surgical skills required only for the small number of failed procedures and excessive or prolonged bleeding. On the other hand, surgical methods require not only equipment and aseptic conditions, but also skills and experience. Some providers want skills and to gain experience and not merely to hand out pills.
In legally restricted settings, medical abortion has the advantage that it is more difficult to prove a medical practitioner gave the woman anything, and perhaps most importantly for both women and providers, most complications are less serious and easier to treat than with unsafe invasive methods. This was the view of many participants at the ICMA conference in 2004. However, like women in these settings, pharmacists and providers may lack access to up-to-date information. Thus, conflicting opinions regarding safety, efficacy, cost, potential for self-medication and acceptability emerged from focus group discussions with general practitioners and obstetrician-gynaecologists in Honduras, Mexico, Nicaragua and Puerto Rico who were aware of medical abortion.Citation36
The most cost-effective provision of medical abortion is through primary health care, with trained mid-level providers. Given the salary costs and scarcity of obstetrician-gynaecologists in resource-poor countries, GPs, nurse-midwives, family planning nurses or other mid-level providers are the most appropriate ones to provide and manage most abortions, both medical and surgical up to 15 weeks, and there is an equally compelling argument for them doing so in developed countries too.Citation37
Most countries that have liberal abortion laws allow those who disagree with abortion on conscience grounds not to participate in abortions, except in emergencies. However, choice as to whether to provide abortions does not apply in the same way to health systems. On public health grounds alone, health systems have a duty to ensure that abortion is safe. Moreover, conscience clauses should not be abused in the public health system to force women to go to a private clinic.
Contrary to what many seem to believe, a full surgical abortion service is not necessary for medical abortion to be provided. The same level and type of care is necessary as is required for treating miscarriages, that is, for approximately 2-6 women out of every 100 who have a medical abortion. Ideally, both medical and surgical methods should be available, but where this is not possible each can be provided without the other.
One of the most reassuring aspects of the findings in studies on medical abortion is that most women and providers all over the world find it acceptable or highly acceptable, and countries can feel confident that they will be offering a safe, effective method. Given the differences between medical and surgical methods, choice and acceptability are important aspects of quality of care and goals worth achieving.
Acknowledgements
This paper is based on a presentation entitled “Why medical abortion is important: issues of choice and acceptability” at Medical Abortion: An International Forum on Policies, Programmes and Services, 17-20 October 2004, Johannesburg, and a presentation entitled “Medical Abortion: Policy, Service Delivery and Product Issues” at a meeting with Scandanavian development ministry and NGO representatives, organised by RFSU, 26 January 2005, Stockholm.
Notes
* There are few published data “proving” this reduction in mortality is taking place, but a wide range of providers from developing countries who are in a position to see these trends agreed it was, at the ICMA conference in 2004.
* Medical Abortion: An International Forum on Policies, Programmes and Services, 17-20 October 2004, Johannesburg.
* See Medical Abortion: A Fact Sheet in this journal issue.
* The dosage of 200mg is as effective as 600mg and is on the WHO Essential Medicines List.Citation3 There is no reason why 600mg should be given any longer. However, many countries approved mifepristone with a regimen of 600mg, before this information was available, and others have followed their lead in spite of the newer findings, which suits the manufacturers as well. The change to 200mg has therefore been slow.
References
- World Health Organization. Safe Abortion: Technical and Policy Guidance for Health Systems. 2003; WHO: Geneva, 28.
- Royal College of Obstetricians and Gynaecologists. The Care of Women Requesting Induced Abortion. National Evidence-Based Clinical Guidelines. London: RCOG, September 2004. Summary at: <www.rcog.org.uk/resources/Public/pdf/abortion_summary.pdf. >. Accessed 27 August 2005.
- WHO Essential Medicines Library. At: http://mednet3.who.int/EMLib/DiseaseTreatments/MedicineDetails.aspx?MedIDName=443@mifepristone-misoprostol. >. Accessed 27 August 2005.
- L Bjorge. Early pregnancy termination with mifepristone and misoprostol in Norway. Acta Obstetrica Gynecologica Scandinavica. 80(11): 2001; 1056–1061.
- PW Ashok, A Kidd, GM Flett. A randomized comparison of medical abortion and surgical vacuum aspiration at 10-13 weeks gestation. Human Reproduction. 17(1): 2002; 92–98.
- S Clark. Is medical abortion acceptable to all American women?. Journal of American Medical Women's Association. 55(3 Suppl): 2000; 177–182.
- A Hemmerling, F Siedentopf, H Kentenich. Emotional impact and acceptability of medical abortion with mifepristone: a German experience. Journal of Psychosomatic Obstetrics and Gynaecology. 26(1): 2005; 23–31.
- C Fiala, B Winikoff, L Helstrom. Acceptability of home-use of misoprostol in medical abortion. Contraception. 70(5): 2004; 387–392.
- E Abdel-Aziz, IM Hassan, H Al-Taher. Assessment of women's satisfaction with medical termination of pregnancy. Journal of Obstetrics and Gynaecology. 24(4): 2004; 429–433.
- Iversen OE, Midboe G, Johnsen SL, et al. [Medical abortion-the first Norwegian experiences]. Tidsskrift Nor Laegeforen 2003;Sep:123. [In Norwegian].
- H Honkanen, H von Hertzen. Users' perspectives on medical abortion in Finland. Contraception. 65(6): 2002; 419–423.
- JT Jensen. Acceptability of suction curettage and mifepristone abortion in the United States: a prospective comparison study. American Journal of Obstetrics and Gynecology. 182(6): 2000; 1292–1299.
- RH Phelps. Mifepristone abortion in minors. Contraception. 64(6): 2001; 339–343.
- C Steele, S Chiarotti. With everything exposed: cruelty in post-abortion care in Rosario, Argentina. Reproductive Health Matters. 12(24 Suppl.): 2004; 39–46.
- PW Ashok, A Templeton, PT Wagaarachchi. Factors affecting the outcome of early medical abortion: a review of 4132 consecutive cases. BJOG. 109(11): 2002; 1281–1289.
- JT Henderson, AC Hwang, CC Harper. Safety of mifepristone abortions in clinical use. Contraception. 72(3): 2005; 175–178.
- US Food and Drug Administration. FDA Alert for Health Professionals: Mifepristone, 22 July 2005. At: <http://www.fda.gov/cder/drug/InfoSheets/HCP/MifepristoneHCP.pdf. >. Accessed 29 August 2005.
- Winikoff B. Global overview of medical abortion. Presentation at Medical Abortion: An International Forum on Policies, Programmes and Services, 17-20 October 2004, Johannesburg.
- L Say, R Kulier, M Gulmezoglu. Medical versus surgical methods for first trimester termination of pregnancy. Cochrane Database Systematic Reviews. 25(1): 2005; CD003037.
- See for example, Faucher P, Baunot N, Madelenat P. [The efficacy and acceptability of mifepristone medical abortion with home administration misoprostol provided by private providers linked with the hospital: a prospective study of 433 patients]. Gynecology, Obstetrics, Fertility 2005;33(4): 220-27. [In French].
- See for example, Hamoda H, Ashok PW, Flett GM, et al. Medical abortion at 9-13 weeks’ gestation: a review of 1076 consecutive cases. Contraception. 2005;71(5):327-32.
- B Winikoff, C Ellertson, S Clark. Analysis of failure in medical abortion. Contraception. 54: 1996; 323–327.
- D Urquhart, A Templeton, F Shinewi. The efficacy and tolerance of mifepristone and prostaglandin in termination of pregnancy of less than 63 days gestation; UK Multicentre Study-final results. Contraception. 55: 1997; 1–5.
- H Hamoda, PW Ashok, GM Flett. Analgesia requirements and predictors of analgesia use for women undergoing medical abortion up to 22 weeks of gestation. BJOG: An International Journal of Obstetrics and Gynaecology. 111(9): 2004; 996–1000.
- CS Shannon, B Winikoff, R Hausknecht. Multicenter trial of a simplified mifepristone medical abortion regimen. Obstetrics and Gynecology. 105(2): 2005; 345–351.
- Ganatra B. Contrasts and common ground: the context of abortion in Asia. Presentation at Medical Abortion: An International Forum on Policies, Programmes and Services, 17-20 October 2004, Johannesburg.
- NT Ngoc. Is home-based administration of prostaglandin safe and feasible for medical abortion? Results from a multisite study in Vietnam. BJOG: An International Journal of Obstetrics and Gynaecology. 111(8): 2004; 814–819.
- S Hajri, J Blum, N Gueddana. Expanding medical abortion in Tunisia: women's experiences from a multi-site expansion study. Contraception. 70(6): 2004; 487–491.
- H Hamoda, HO Critchley, K Paterson. The acceptability of home medical abortion to women in UK settings. BJOG: An International Journal of Obstetrics and Gynaecology. 112(6): 2005; 781–785.
- T Ashima, A Vinita, R Shalini. Early medical abortion: a new regimen up to 49 days' gestation. Australia & New Zealand Journal of Obstetrics & Gynaecology. 45(2): 2005; 137–139.
- Cullingworth L. A cost analysis of service provision of medical abortions in the public health sector at primary and secondary level. Presentation at Medical Abortion: An International Forum on Policies, Programmes and Services, 17-20 October 2004, Johannesburg.
- B Ganatra, M Bygdeman, Phan Bich Thuy. From research to reality: the challenges of introducing medical abortion into service delivery in Vietnam. Reproductive Health Matters. 12(24 Suppl): 2004; 105–113.
- DA Grimes, MS Smith, AD Witham. Mifepristone and misoprostol versus dilation and evacuation for midtrimester abortion: a pilot randomised controlled trial. BJOG: An International Journal of Obstetrics and Gynaecology. 111(2): 2004; 148–153.
- Fiala C, Swahn ML, Stephansson O, et al. The effect of non-steroidal anti-inflammatory drugs on medical abortion with mifeprisone and misoprostol at 13-22 weeks gestation. Human Reproduction 2005; August 11 (Abstract only, e-publication).
- PW Ashok, A Templeton, PT Wagaarachchi. Midtrimester medical termination of pregnancy: a review of 1002 consecutive cases. Contraception. 69(1): 2004; 51–58.
- H Espinoza, K Abuabara, C Ellertson. Physicians' knowledge and opinions about medication abortion in four Latin American and Caribbean region countries. Contraception. 70(2): 2004; 127–133.
- C Joffe, S Yanow. Advanced practice clinicians as abortion providers: current developments in the United States. Reproductive Health Matters. 12(24 Suppl.): 2004; 198–206.