Abstract
This study examines changes in levels and patterns of maternal mortality in Pernambuco, Brazil, in 1994 and 2003. The research was carried out in five sub-regions of Pernambuco using the Reproductive Age Mortality Survey (RAMOS) method and based on death certificates of women of reproductive age registered in the local System of Information on Mortality. In-depth interviews with family members were also conducted for the abortion-related deaths. Of the 1,258 female deaths investigated, 54 maternal deaths were identified, corresponding to a maternal mortality ratio of 77 per 100,000 live births. The estimated level of under-reporting (46%) corresponds to an upward adjustment factor of 1.9. The illegal status of abortion in Brazil remains an important contributory factor for the abortion-related deaths. Approximately 94% of the maternal deaths were judged to be avoidable with improvements in health care. Maternal mortality declined by 30% over the ten-year period but the level of misclassification of maternal deaths remains. Improvements in maternity care for women and reporting of maternal deaths are still urgently needed.
Résumé
Cette étude examine les changements des niveaux et des catégories de mortalité maternelle dans cinq sous-régions de Pernambuco (Brésil) en 1994 et 2003. La recherche a utilisé la méthode RAMOS (étude des femmes en âge de procréer) et s’est basée sur les certificats de décès de femmes en âge de procréer enregistrés dans le système local d’information sur la mortalité. Des entretiens approfondis ont également été menés avec des membres de la famille pour les décès liés à un avortement. L’enquête a permis d’identifier 54 décès maternels sur les 1258 décès de femmes étudiés, ce qui correspond à un taux de mortalité maternelle de 77 pour 100 000 naissances vivantes. On évalue à 46% le niveau de sous-estimation des cas, ce qui correspond à un facteur d’ajustement à la hausse de 1,9. L’illégalité de l’avortement au Brésil continue de contribuer sensiblement aux décès liés à l’avortement. Environ 94% des morts maternelles ont été jugés évitables par des améliorations des soins de santé. La mortalité maternelle a diminué de 30% en dix ans, mais le niveau de classement erroné des décès maternels est demeuré le même. Il est encore nécessaire d’améliorer sans délai les soins obstétricaux et la déclaration des décès maternels.
Resumen
En este estudio se examinan los cambios en los niveles y patrones de mortalidad materna en Pernambuco, Brasil, en 1994 y 2003. La investigación fue realizada en cinco subregiones de Pernambuco utilizando el método de la Encuesta de Mortalidad en Edad Reproductiva (RAMOS) y con base a las actas de defunción de mujeres en edad reproductiva registradas en el sistema local de Información sobre la Mortalidad. En los casos de muertes relacionadas con aborto, se realizaron entrevistas a profundidad con familiares. De las 1,258 muertes investigadas, se identificaron 54 muertes maternas, lo cual se corresponde a una razón de mortalidad materna de 77 por cada 100,000 nacidos vivos. El nivel aproximado de subregistro (46%) se corresponde a un factor de ajuste al alza de 1.9. La condición ilegal del aborto en Brasil continúa siendo un importante factor contribuyente a las muertes relacionadas con el aborto. Aproximadamente el 94% de las muertes maternas fueron consideradas evitables con mejorías en la atención médica. La mortalidad materna disminuyó en 30% durante el plazo de 10 años, pero el nivel de mal clasificación de muertes maternas continúa siendo el mismo. Aún es imperativo mejorar la atención de maternidad y el registro de muertes maternas.
The overall maternal mortality ratio for Latin American and Caribbean countries was estimated to be 190 deaths per 100,000 live births in 2000, and was associated with direct obstetric causes, complications from abortion and AIDS. The Americas present the largest inequality in maternal mortality in the world; while in Canada the maternal mortality ratio in 1996 was 4 per 100,000 live births, in Haiti it was 523.Citation1Citation2
The use of maternal mortality as a development indicator, and its importance on the international agenda associated with women’s movement campaigns, drew attention to this subject among Brazil’s health policymakers. Since the 1990s, national and local initiatives have tried to obtain a better estimate of maternal mortality and control its magnitude. However, there is still a large gap between the ratio estimated by WHO in 2000, 260 per 100,000 live births and the more recent ratio estimated by the Minister of Health of 54 per 100,000 live births in 2004.Citation3 A study conducted in 26 Brazilian capitals found a ratio of 74 per 100,000 live births in 2002, and a level of misclassification of 28%,Citation4 which varied by region.
These differing estimates are likely a result of the different methodologies applied. While the WHO used indirect techniques, Laurenti et al used the RAMOS method, and the Minister of Health used national vital statistics, without any adjustments.Citation1,3,4 This shows the difficulties in assessing maternal mortality for a large and unequal country like Brazil. Finding a better approach represents a major challenge because some regions stand midway between African countries with precarious health systems and developed countries, while others have better vital statistics and quality of health care, e.g. the south and southeast of Brazil.
There has been only one study on maternal mortality for the State of Pernambuco. It was carried out in 1994 using the RAMOS method. It found a ratio of 103 in the Metropolitan region and 195 per 100,000 live births in the Sertão region.Citation5 The level of misclassification reached 30%. Pregnancy-induced hypertension, haemorrhage and abortion complications were the most common causes of death, and the direct causes of death accounted for approximately 80% of all maternal deaths.
This study generated integrated policy interventions in Pernambuco, coordinated by the Women’s Health Department, using a set of national and local strategies; these took into account the geographical distribution of maternal deaths across the state and the main causes of death. Physicians and nurses from the hospitals and out-patient clinics of the State Health Administrative Regions (GERES) were trained in obstetric emergences, and maternal mortality surveillance was initiated.Citation6 Public sector abortion services permitted by law were also instituted,Citation7 Footnote* along with treatment for incomplete abortions using vacuum aspiration. Yet, after almost a decade, women of reproductive age in Pernambuco are still exposed to avoidable causes of death and there are no precise data on the incidence or trends in maternal mortality since 1994. The exceptions are the cities of Recife and Camaragibe, both in the Metropolitan Region, which have monitored and analysed their data more systematically.Citation8Citation9
This investigation aimed to overcome research obstacles in measuring maternal mortality in the Northeast of Brazil and strengthen the vital registration system by estimating the level of maternal mortality and of misclassification on death certificates in the regions of Pernambuco, comparing the findings with those from 1994. It also aimed to understand the role of women’s status and health care provision in these deaths.
Study design and population
This study used the International Classification of Diseases (ICD-10).Citation10 It defines an early maternal death as the death of a woman while pregnant, during an abortion or within 42 days of termination of pregnancy, from any cause related to or aggravated by pregnancy or its management, but not by accidental or incidental causes, and late maternal death between 43 days and one year after delivery or abortion. The term “abortion” is used in Brazil for both spontaneous miscarriage and induced abortion.
Both quantitative and qualitative data were collected and analysed. The RAMOS method, the quantitative approach used, is based on the identification of maternal deaths among all deaths of reproductive age women through records from hospitals, autopsy services and home interviews.Citation1 In-depth interviews of relatives of the deceased women and medical staff represented the qualitative approach.
The fieldwork was carried out in Pernambuco from June 2003 to September 2004. Pernambuco is in the Northeast of Brazil. Its population in 2003 was 8.2 million, including 2.7 million women aged 10-49 years.Citation11 The state has five political and administrative regions: Metropolitan, Mata, Agreste, Sertão and São Francisco. Each region contains administrative health regions (GERES), with a total of 10 GERES in 2003.
As regards socio-economic indicators, 22% of the population over age 15 had no formal education and 49% earned less than half of Brazil’s minimum wage. Metropolitan Region, the most developed and urbanised sub-region, contained 45% of the state population, and had the best coverage and quality of health facilities. The Sertão (GERES IX), had the worst coverage and quality of the obstetric care, and the Agreste (GERES V) the worst coverage and quality of the vital registration system.Citation11–13
The total fertility rate in Pernambuco in 2003 was about 2.1. 97% of births take place in hospital,Citation11–13 and the caesarean section rate (38%) was above of the WHO recommendations, even in the public sector (in the private sector it can reach 90%). There was no official family planning policy, a high prevalence of female sterilisation (45% of women in union in 2001 in Recife), a precarious quality of antenatal care and just two clinics doing abortions permitted by law, located in the state capital.Citation11Citation14
Regarding national data on mortality, in 2003 the level of coverage for Pernambuco was estimated at 77%, below the national level of 84%. The Metropolitan Region had the best coverage. Pernambuco had the lowest proportion of unspecified causes of death (19%) in the Northeast; the national average was 14%.Citation13 In 1995, the Maternal Mortality Committee of Pernambuco was set up and female mortality surveillance was initiated in 1997, and by 2003, two regional and four municipal Maternal Mortality Committees had also been started. However, in 2002 only 42% of total deaths of women of reproductive age had systematically been investigated.Citation12
The study area was one administrative health region (GERES) in each region of Pernambuco, the same ones as those selected for the 1994 study. The criteria used then were the presence of an organised vital registration system and a referral hospital to attend births.
Instruments and data collection
Three questionnaires were field tested in 2001 for 64 deceased women of reproductive age outside of the study population, and the Confidential Questionnaire of Female Deaths was validated and modified.Citation9 They were used in this order:
| • | Confidential Questionnaire of Female Deaths (Q1) – used to list and classify all female deaths aged 10-49 in 2003 in the regions and general information registered where the deaths occurred. | ||||
| • | Confidential Questionnaire of Maternal Mortality (Q2) – information about possible (misclassified) cause of maternal death and declared (definitive underlying cause of maternal death) maternal deaths at hospitals or autopsy services from medical and autopsies records. | ||||
| • | Confidential Questionnaire of Household (Q3) – based on the verbal autopsy technique, and used to interview relatives or others associated with the deceased women.Citation15 | ||||
Trained assistants carried out the data collection using RAMOS. Ethical issues were explained and discussed.
In order to estimate the coverage of female death registration, death certificates were sought in the public register of vital statistics; death certificates for women who lived in the regions studied but died in other cities or neighboring states were sought in the National System of Information on Mortality. The data were matched with the data from the Epidemiological Departments in order to obtain the expected number of female deaths. Death certificates of women who died in the study area but were from other regions or states were excluded.
More than one data source was consulted in order to eliminate non-maternal deaths: the combination of hospital/autopsy records and home interviews was used in 21.6% of cases, home interviews and autopsy records in 2.5%, and home interviews alone in 69.5% of cases. For the remaining 6.3%, other data sources were consulted (Family Health Programme,Footnote* media, women’s organisations). The fieldwork took 16 months. The proportion of refusals, from home interviews, was less than 0.2% for all female deaths investigated.
Data processing
An expert group of the Maternal Mortality Committee of the state Pernambuco and the city of Recife (composed of physicians, nurses, epidemiologists and representatives of the obstetrics departments and women’s movement) analysed the deaths from the five sub-regions. The conclusion of each case using all the data collected was obtained by consensus.
Maternal mortality levels and misclassification estimates were calculated using the statistics on female population for the sub-regions aged 10–49, estimated by the IBGE (Brazilian Statistics Bureau); the live births were taken from the National System of Information on Live Births (SINASC/DATASUS), which reached 90% of coverage for the state in 2003.Citation13 In order to compare the maternal mortality ratios for 1994 and 2003 and also to correct incomplete registration of live births for the former year, the estimates for 1994 were recalculated using the live births from 1994 obtained from SINASC in 2005.
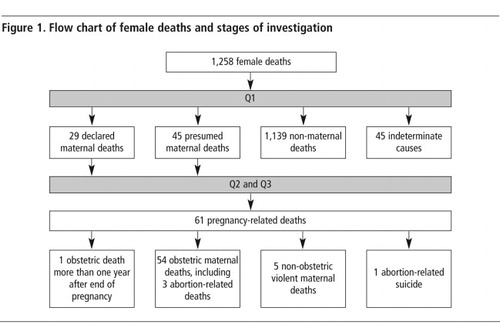
Sixty-one pregnancy-related deaths were identified across the five sub-regions (). Five were non-obstetric violent deaths and one was an abortion-related suicide, which were excluded from the analysis because they were non-obstetric deaths. One was a death that occurred more than a year after the pregnancy had ended, and although it was an obstetric death, it was excluded because it occurred after one year. For international comparison, the maternal mortality ratio was calculated only with deaths up to 42 days after delivery. Late maternal deaths (10 cases, 18%) were included because they had been counted in the previous study. Thus, 54 maternal deaths, of which three were abortion-related, were included in the analysis.

The qualitative analysis was conducted using both interviews and the medical records. Relatives of each deceased woman were contacted and an interview scheduled in their home towns. Husbands, fathers, sisters, mothers, friends and mothers-in-law were interviewed. They were asked to confirm socio-demographic and reproductive health data, and asked for specific information on the circumstances of the death and how they perceived the whole process from antenatal care until the death.
The 54 deaths represent the study population; thus, it can be assumed that these deaths represent all maternal deaths of women who lived and were registered in those health regions during 2003 but not a sample of the maternal deaths of the State of Pernambuco. Therefore, statistical tests for significant differences across areas and sub-populations were not performed.
Even though the data were collected in the five GERES, in the results they were aggregated into the follow three major regions to be more consistent: Metropolitan, Mata/Agreste and Sertão/São Francisco.
Limitations of the research
Period mortality studies become more robust if at least three years of data can be collected; the data set used here referred to a single year. In addition, since maternal deaths are rare events, to gather a large data set in Pernambuco would have needed more than a year of investigation. Some medical records could not be located easily, a few were reported as lost and many were incomplete. The autopsy services were limited to GERES I and GERES VIII and were not as helpful as was expected. Despite the fact that all data sources available were used, it is impossible to be sure that only 54 maternal deaths occurred in the five sub-regions. Finally, the relatively small number of maternal deaths permitted the use of descriptive statistics as the only way to analyse the data. Ideally, multivariate methods would be used.
Results
summarises the process of investigation and the results obtained using the three instruments. Of 1,264 female deaths of reproductive age investigated, six were excluded because it was unknown which GERES they came from. Of the 1,258 deaths, 45 (3.5%) were classified as unsolved cases, while 74 (6%) occurred during pregnancy or within a year of pregnancy (29 were definite and 42 presumed maternal deaths). One was excluded because the date of death exceeded a year. Six injury-related deaths were classified as non-obstetric maternal deaths, leaving 54 obstetric deaths according to ICD-10. Ten (18%) were late maternal deaths. Four were abortion-related deaths, three of which were obstetric deaths according to ICD-10 and one a suicide to hide the pregnancy. The suicide was misclassified as being of undetermined cause, even in the autopsy report, but was classified as an abortion-related suicide after two home interviews.
Most of the women who died (41%) lived in Recife (GERES I) and 16% in GERES VIII. Just over half (52.5%) happened in GERES I and 19.7% in GERES VIII. GERES V had 8.2% of deaths. Three women died outside the health regions studied. 92% of the deaths occurred in a health facility. 72% in a public hospital (including federal university hospitals), 24% in public conveniados hospitals (private health services that have been contracted to complement the public health system) and 4% (two deaths) in private hospitals in Recife. The deaths occurred mostly in referral maternity services with intensive care units. None occurred on the way to a health facility or on the street.
Maternal mortality estimates
The overall maternal mortality ratio for 2003 was 77 per 100,000 live births (Table 1). If only early maternal deaths were counted, the ratio would be 63 per 100,000 live births. Sertão and São Francisco major region had the highest level, followed by the Metropolitan and Mata/Agreste major regions. The overall lifetime risk of maternal death was one woman in 512 during the reproductive lifespan in 2003. It was one in 209 in Sertão/São Francisco and one in 656 in Metropolitan major regions.

In 2003, the System of Information on Mortality reported 29 maternal deaths, and the study identified 25 more, generating a misclassification of 46%, which corresponds to an adjustment factor of 1.9. The crude ratio, without adjustment, would be 41 rather than 77 per 100,000 live births (Table 1).
The highest levels of misclassification of maternal deaths were found in the Metropolitan and Mata/Agreste regions, about 2.0. The main reason for misclassification was the failure of doctors to register a recent pregnancy on the death certificates. In this regard, there are two important instruments to help doctors declare the underlying cause of death: medical records and the autopsy. Although it is impossible to know whether the medical records were consulted by the physicians before declaring a female death, the quality of these records was, in general, precarious. In terms of necropsy, 32% of maternal deaths (17 cases) underwent an autopsy, of which only ten had the uterus and other reproductive organs analysed during the process.
The pregnancy status tick-box on the death certificates, included on Brazilian death certificates since 1995, was ticked in 31 cases (57.4%) of pregnancy-related deaths, depending on whether the underlying causes of death were declared or not.Citation17 Among the 29 declared maternal deaths, 21 (72%) had the box ticked. Of the 25 undeclared maternal deaths, 15 (60%) did not have the box ticked.
Causes of death and characteristics of the deceased women
Most of the women who died were 20–29 years old; two adolescents died at age 15. One woman had had two abortions, one pre-term stillbirth and two live births. She died from complications of pregnancy-induced hypertension, and according to her mother, suffered physical violence from her partner and her brother-in-law, which might have been related to her previous negative pregnancy outcomes. Pregnancy-related mortality risk was seven times higher for women under 16 years old and 12 times higher for those over 40.
Parda (racially mixed) and black women accounted for 78% of all maternal deaths. Although few deaths in black women were reported, they were five times more likely to die from maternal causes than white women, and parda women 1.7 times more likely to die than white women.
Women with less than three years of schooling represented 35% of the maternal deaths, 15% had no education and only 2% had more than 12 years of schooling. Regarding marital status, 42% were single and 30% married. Overall, domestic work was the most common occupation (58%), followed by agricultural work (19%).
Their previous obstetric records revealed that 41% of the women had had no pregnancies or just one. Almost 30% had had more than ten pregnancies. One woman, at 42 years old, had had 23 pregnancies, including three abortions, 19 live births and one stillbirth.
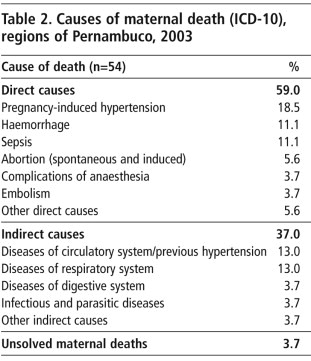
Pregnancy-induced hypertension (18.5%) was the leading cause of death (Table 2). Disease of the circulatory or respiratory system represented the second and third leading causes of death, 13% and 11%, respectively, followed by abortion-related deaths. Abortion was the most frequent cause of death in the São Francisco region and, surprisingly, all the women sought treatment for the complications; one was reported as a miscarriage, but, regardless of that, all of them received inadequate treatment at the hospitals.
In general, direct maternal deaths were more accurately classified than indirect maternal deaths. The most common misclassified causes of death were diseases of the circulatory system.
Why the women died
13% of women had received no antenatal care, but an evaluation of the quality of care for those who did receive it, using the score proposed by Kotelchuck, adapted by Leal,Citation18 suggested that it was adequate for only 21% of them.
Of the 98% hospital births, only 28% were admitted to a hospital that could deal with their complications from the start, while half the women had to try more than one hospital before they were admitted. Most had to be transferred from local to referral hospitals located outside their health region of residence. This situation was worse in the interior, but in the Metropolitan Region only 40% were admitted on their first attempt. After reaching a health facility, 37% receive assistance immediately, but 80% received it only within two hours. One woman had to wait for 30 hours in hospital to receive assistance for delivery. A full 53% of the deaths occurred in referral hospitals, mostly in Recife (Metropolitan region) and Petrolina (São Francisco region). Moreover, having access and receiving assistance did not mean effectiveness in the health care as an example from Metropolitan Region shows:
A women who was 36 weeks’ pregnant sought health care for acute respiratory problems. She went to two emergency rooms, using her own transportation, but the medical staff at both places did not feel able to attend her because she was pregnant. According to the autopsy records, she died upon arrival at the third hospital from acute cardiovascular failure due to complications of essential hypertension. She was still pregnant.
There was no different between vaginal births and caesarean sections in terms of distribution of deaths. Although it is complex to assess whether a caesarean section was appropriate or not, at least three women who died after a caesarean section had no clear medical indications. In one case, the indication recorded was “woman’s request” in the private sector. She was 17 years old and afraid to have a vaginal birth; she died hours after delivery due to anaesthesia complications. The other two caesarean sections, both in the public sector, had indications such as cephalic-pelvic disproportion and obstructed labour, but according to their relatives, both had actually wanted a tubal ligation: one died due to post-surgery sepsis and the other an embolism.
Of 47 deliveries studied (34 live births and 13 stillborns), the records showed that 81% were attended by a physician, 11% by a practice midwife and 2% by a traditional midwife (home births). Practical midwives are practical nurses that attend births at the hospitals without being trained for it. Although under-reported, most deliveries that occurred in local hospitals were, in fact, attended by these practical midwives, who unofficially stood in for the doctors during labour and vaginal birth.
Overall, 23 (46%) women needed a blood transfusion but 6 (26%) of them did not receive it due to the absence of a blood bank in the city or the hospital, delay in identifying the need or delay in blood being made available. 74% of the women who died needed to be in an intensive care unit, but 37.8% had no access to one.
Even though the women had followed all the guidelines for antenatal care and hospital birth of the Brazilian Ministry of Health, poor antenatal, delivery and emergency care were directly implicated in their deaths.
A young women, 21 years old, first pregnancy, from the Sertão region started antenatal care during the first trimester and completed nine antenatal visits in the local hospital, all attended by a practical nurse under a physician supervision. She presented signs of pregnancy-induced hypertension early in the antenatal records from 28 weeks, including high blood pressure and excessive weight gain. She was admitted to the same local hospital where she had received antenatal care. Upon arrival, her high blood pressure had increased, and she also had headache and swelling. She spent 12 hours without adequate treatment in the hospital ward. She did not receive specific medications for pre-eclampsia until after her first convulsion. She had a post-mortem caesarean section to save the baby’s life, but the baby also died.
Maternal mortality ratios: 1994 and 2003
In order to compare maternal mortality estimates between 1994 and 2003 (for both years, early and late maternal deaths are included), age-specific fertility rates and age-specific mortality rates were reviewed. Overall, the total fertility rate was reduced from 2.3 children per woman in 1994 to 2.1 in 2003 for all regions studied. The largest decline occurred in older women, with an increase at younger ages, mainly among adolescents. Age-specific maternal mortality was reduced in all age groups. No maternal deaths were registered below age 15 for 2003 or over age 45 for both years. The ratio in age groups 20–24 and 25–29 fell by about 50%.
Maternal mortality ratios for 2003 by major regions remained high, but were lower than for 1994 overall, with different levels of decline per region (Table 3). The biggest decline was in Mata/Agreste followed by São Francisco. The lowest decline was in Metropolitan region.

Although the leading cause of death (pregnancy-induced hypertension) has not changed since 1994, the distribution of other causes has changed. Direct maternal deaths fell 28%, while indirect maternal deaths rose 42%. Among indirect causes, diseases of the circulatory and respiratory systems were the most frequent. Chronic and degenerative diseases such as diabetes have reached the female population of reproductive age, contributing to a new pattern of maternal deaths that demands attention to women’s health care that goes beyond obstetric assistance during pregnancy and delivery.
Discussion
The maternal mortality ratio for the three major regions for 2003 was 30% lower than in 1994,Citation5 a level similar to that estimated by Laurenti el al for the Northeast capitals in 2002 (74 per 100,000 live births).Citation4 However, the current study identified an almost 50% difference between Metropolitan and Sertão regions over the period.Citation5 The historically lower level of maternal mortality in Metropolitan region compared with other regions might explain why it has been easier to reduce maternal levels in Sertão and Mata/Agreste regions.
The level of misclassification (46%) and the consequent adjustment factor (1.9), demonstrate that for each maternal death registered in the System of Information on Mortality, almost one other case was identified in this investigation, again similar to that for the Northeast capitals in 2002 (1.76).Citation4 Misclassification of maternal deaths generally depends on the quality of national and local vital statistics and in particular, on the commitment and awareness of physicians reporting the presence of a recent pregnancy in a death certificate.
The nature, timing and place of occurrence of indirect maternal deaths are an element in the omission of a pregnancy on the death certificates; deaths in intensive care units days or weeks after a birth or abortion are also less likely to have the pregnancy reported on the death certificate. Direct maternal deaths that occur in maternity wards right after a delivery or abortion are more likely to be reported. The increased proportion of indirect causes of death in Metropolitan region could explain why misclassification was so much higher there.
Pregnancy-induced hypertension remained the leading cause of death for all regions except São Francisco, where it was replaced by abortion-related deaths. Since the 1980s, pregnancy-induced hypertension has been the leading cause of maternal death in Brazil.Citation5,19,20 Indeed, a recent analysis has confirmed that hypertensive disorders of pregnancy are the leading cause of maternal deaths in Latin America and the Caribbean.Citation21
In this investigation, multiple factors involving quality of care were responsible for 94.4% of avoidable maternal deaths. Poor antenatal care was found everywhere, but was worse in the interior. Women are being attended without the minimum recommended medical supervision,Citation22 and there is a lack of arrangements for referral of high risk antenatal cases.
Although most births take place in hospitals,Citation13 a woman in labour is not guaranteed a bed in a public hospital even if she has full antenatal care or a high risk pregnancy. In this study, most women had to seek admission to more than one hospital, a widespread problem, reported elsewhere in the country.Citation5,19 In Rio de Janeiro, for example, a third of 6,652 pregnant women in labour had to look for health care in more than one hospital.Citation23 Limited numbers of beds in neonatal and adult intensive care units was the most common reason for this problem in Metropolitan region, and too few medical staff was the most frequent reason in the interior of the State.
The relationship between caesarean section and maternal deaths has continued to be controversial. Caesarean section has been associated with maternal morbidity and mortality more so than vaginal delivery. Septicaemia, haemorrhage, pulmonary embolism, anaesthetic complications and premature births are the most frequent negative outcomes described.Citation24–28 In the Northeast, the severity of these outcomes may depend on the timing and appropriateness in each case, the health of the woman and the availability of requisite medical staff, especially in the interior, particularly anaesthetists. Our findings in two cases of death related to caesarean section is that they continue to be performed to obtain a tubal ligation, a particularly Brazilian problem.
Relatively better access to medical technology and blood transfusion, a high prevalence of female sterilisation and the use of misoprostol to induce abortions instead of unsafe invasive methods are responsible for the relative decrease in deaths from haemorrhage, puerperal infections and abortion complications. In addition, the work of the Maternal Mortality Committees, which has raised the avoidable nature of so many deaths in public debate, may also have helped to reduce maternal mortality in the State.
Measuring maternal mortality in a developing country setting is an important first step to reduce maternal mortality. However, it is still a challenge to carry out these measurements due to the weakness in the reporting and information systems, the misclassification of underlying causes of death, the rare nature of maternal deaths, the large sample size required and financial constraints.
The Brazilian National Pact to Reduce Maternal and Neonatal Mortality in the National Programme of Women’s Health Care,Citation22 aimed to reduce maternal mortality by 15% between 2004 and 2006.Citation3 Millennium Development Goal 5 calls for a reduction in maternal mortality by 75% between 1990 and 2015. For such goals to be achieved there is a need for major improvements in the health care system across Pernambuco. Abortion-related deaths, for instance, were associated with unequal access to family planning and neglect during treatment for incomplete abortions, but the illegality of abortion is the main issue.
Continuing efforts and investments to improve maternal mortality surveillance at local and regional levels is needed. At local levels, this requires intersectoral actions that embrace rural and urban populations, including the Family Health Programme, municipal cemeteries, office of vital statistics (cartórios), local hospitals and traditional midwives. In cities of more than 100,000 inhabitants, it needs a more complex articulation to take into account all sources of mortality data, such as the Family Health Programme, local and referral hospitals, office of vital statistics, autopsy services as well as the media and women’s health organisations. At medical schools (for medical students and physicians in training), it is necessary to highlight the importance of providing precise information on vital events both in vital statistics systems (birth and death certificates) and medical records.
To reduce maternal mortality levels, access to family planning must be provided under the Brazilian Family Planning Law (1997),Citation29 but with protection of sexual and reproductive rights. Comprehensive antenatal care and the promotion and monitoring of health care for all pregnant women are needed. A study should be launched of the shortage of beds for both low and high risk pregnant women across the State, according to WHO and Ministry of Health parameters.
Regarding abortion complications, the 2004 National Guidelines for Humanised Abortion Care,Citation23 need to be followed and legal abortion services should be provided in all GERES sites to give women the right to terminate their pregnancies in cases permitted by law. Ideally, abortion should be legalised.
Lastly, Maternal Mortality Committees should be set up in all cities with more than 100,000 inhabitants. Inter-institutional and multi-professional Maternal Mortality Committees can contribute to both the improvement of maternal health data and the reduction of maternal mortality. Holding them accountable in Pernambuco is a responsibility taken by feminist and women’s health organisations.
Mother of six with newborn baby, waiting for a boat to go home after the birth, Porto de Moz, Para, Brazil
Acknowledgements
I would like to thank the staff of the Department of Information on Mortality of the Health Secretariat of the State of Pernambuco (central and regional levels) and of Recife, Olinda and Camaragibe, for their partnership during the fieldwork and data processing; and the Maternal Mortality Committee, State of Pernambuco, for discussing all maternal deaths. This research was funded by the Mellon Foundation via the Population Research Center, University of Texas at Austin, and the Brazilian Ministry of Health via the Vigilance on Health Secretariat.
Notes
* Abortion is permitted only when pregnancy occurs after rape and when the life of the pregnant woman is at risk.
* The Family Heath ProgrammeCitation16 is the main entry to the public health system in Brazil, except for emergency care, through deccentralised health units in the community.
References
- World Health Organization United Nations Children’s Fund and United Nations Population Fund. Maternal Mortality in 2000: Estimates developed by WHO, UNICEF and UNFPA. 2005; WHO: Geneva.
- Pan American Health Organization. Regional Strategy for Maternal Mortality and Morbidity Reduction. 2002; PAHO, Report of the 26th Pan American Health Conference: Washington DC.
- Ministério da Saúde. Secretaria de Vigilância em Saúde. 2006; Saúde Brasil: Brasília.
- R Laurenti, MHP Mello Jorge, SDG Leal. A mortalidade materna nas capitais brasileiras: algumas características e estimativa de um fator de ajuste. Revista Brasileira de Epidemiologia. 7(4): 2004; 449–460.
- Valongueiro SA. Mortalidade Materna em Pernambuco: Um Estudo Quantitativo e qualitativo (Thesis) Belo Horizonte, Brasil: Universidade Federal de Minas Gerais. CEDEPLAR, 1996.
- Governo de Pernambuco. Primeiro Relatório do Sistema de Vigilância de Mortalidade Materna de Pernambuco, 1998.
- Brasil Código Penal: Decreto Lei No. 2848 de 7/12/1940, 34a ed. São Paulo: Saraiva, 1996.
- Guimarães MJ, Santos Sony. Mortalidade materna em Recife 1994–1997. Paper presented at National Meeting of Epidemiology, Rio de Janeiro, 1998.
- SA Valongueiro, A Ludermir, LAF Gominho. Avaliação de procedimentos para estimar mortalidade materna. Cadernos de Saúde Pública. 19(Suplemento 2): 2003; S293–S301.
- World Health Organization. International Classification of Diseases, 10th revision. Authorised Portuguese edition. 1993; Edusp: São Paulo.
- Brasil. Rio de Janeiro: Fundação Instituto Brasileiro de Estatística, 2000. At: <ftp://ftp.ibge.gov.br/Estimativas_Projecoes_Populacao/>.
- Governo de Pernambuco, Brasil. Secretaria de Saúde. Unidade de Informações Epidemiológicas, 2005.
- Ministério da Saúde. DATA-SUS. Sistemas de Informações em Saúde. At: <www.datasus.gov.br/>.
- Miranda-Ribeiro P, Junqueira AC, Santos TF. Saúde Reprodutiva, Sexualidade e Raça /Cor. Relatório Descritivo. Belo Horizonte, 2004.
- D Chandramohan, H Gillan, L Rodrigues. Verbal autopsy for adult deaths: development and validation in a multicentre study. Tropical Medicine and International Health. 8: 1998; 436–446.
- Ministério da Saúde. Departamento de Atenção Básica e Saúde da Família. Brasília. Brazil. At: <http://dtr2004.saude.gov.br/dab/atencaobasica.php>.
- R Laurenti, J Mello, S Gotlieb. Mortes maternas no Brasil: analise do preenchimento da Declaração de Abito. Informe Epidemiológico do SUS. 9: 2000; 43–50.
- MC Leal, GNG Silvana, KMN Ratto. Uso de índice da Kotelchuch modificado na avaliação da assistência pré-natal e sua relação com as características maternas e o peso do recém-nascido no município do Rio de Janeiro. Cadernos de Saúde Pública. 20(Suplemento 1): 2006; S63–S72.
- Tanaka, AC, Mitsuiki L. Estudo da Magnitude da Mortalidade Materna em 15 cidades brasileiras. Relatório de Pesquisa, Faculdade de Saúde Pública. São Paulo, 1999.
- AAF Siqueira. Mortalidade materna no Brasil. Revista de Saúde Pública. 18(6): 1980; 448–465.
- KS Khan, D Wojdyla, L Say. WHO analysis of causes of maternal death; a systematic review. Lancet. 367(9516): 2006; 1066–1074.
- Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. Programa Nacional de Assistência Integral à Saúde da Mulher. Brasília, 2004. At: <http://portal.saude.gov.br/portal/saude>.
- DCS Menezes, IC Leite, JM Schramm. Avaliação da peregrinação anteparto numa amostra de puérperas no município do Rio de Janeiro, Brasil 1999/2001. Cadernos de Saúde Pública. 22(3): 2006; 553–559.
- E Royston, S Armstrong. Preventing Maternal Mortality. 1989; World Health Organization: Geneva.
- RMY Nomura, EA Alves, M Zugaib. Complicações maternas associadas ao tipo de parto em hospital universitário. Revista de Saúde Pública. 38(1): 2004; 9–15.
- A Faúndes, J Cecatti. A operação cesariana no Brasil: incidência, tendências, causas, conseqüências e propostas de ação. Cadernos de Saúde Pública. 7: 1991; 150–173.
- J Potter. Unwanted caesarean sections among public and private patients in Brazil: prospective study. British Medical Journal. 232: 2001; 1155–1159.
- SG Diniz, AS Chacham. The “cut above” and the “cut below”: the abuse of caesareans and episiotomy in São Paulo, Brazil. Reproductive Health Matters. 12(23): 2004; 100–110.
- Brasil. Law No. 9263. Brasília: Diário da União, 20 August 1997.