Abstract
Alternative strategies to increase access to reproductive health services among internally displaced populations are urgently needed. In eastern Burma, continuing conflict and lack of functioning health systems render the emphasis on facility-based delivery with skilled attendants unfeasible. Along the Thailand–Burma border, local organisations have implemented an innovative pilot, the Mobile Obstetric Maternal Health Workers (MOM) Project, establishing a three-tiered collaborative network of community-based reproductive health workers. Health workers from local organisations received practical training in basic emergency obstetric care plus blood transfusion, antenatal care and family planning at a central facility. After returning to their target communities inside Burma, these first-tier maternal health workers trained a second tier of local health workers and a third tier of traditional birth attendants (TBAs) to provide a limited subset of these interventions, depending on their level of training. In this ongoing project, close communication between health workers and TBAs promotes acceptance and coverage of maternity services throughout the community. We describe the rationale, design and implementation of the project and a parallel monitoring plan for evaluation of the project. This innovative obstetric health care delivery strategy may serve as a model for the delivery of other essential health services in this population and for increasing access to care in other conflict settings.
Résumé
De nouvelles stratégies sont nécessaires sans délai pour élargir l’accès des personnes déplacées aux services de santé génésique. Au Myanmar oriental, la persistance du conflit et le manque de systèmes de santé en état de marche empêchent de mettre l’accent sur les accouchements en maternité avec une assistance qualifiée. Le long de la frontière avec la Thaïlande, des organisations locales appliquent une initiative novatrice, le projet des agents de santé maternelle et obstétricale mobile (MOM), qui établit un réseau à trois niveaux d’agents communautaires de santé génésique. Les agents de santé des organisations locales ont suivi une formation pratique aux soins obstétricaux d’urgence ainsi qu’aux transfusions sanguines, aux soins prénatals et à la planification familiale dans un établissement central. De retour dans leur communauté à l’intérieur du Myanmar, ces agents de santé maternelle du premier niveau ont appris à un deuxième niveau d’agents de santé locaux et à un troisième niveau d’accoucheuses traditionnelles à assurer un sous-ensemble limité de ces interventions, en fonction de leur formation. Dans ce projet, une communication étroite entre les agents de santé et les accoucheuses traditionnelles encourage l’acceptation des services de maternité et leur couverture dans toute la communauté. Nous décrivons la raison d’être, la conception et l’application du projet ainsi qu’un plan parallèle pour l’évaluer. Cette stratégie innovante de prestation des soins obstétricaux peut servir de modèle pour d’autres services de santé essentiels et pour élargir l’accès aux soins dans d’autres situations de conflit.
Resumen
Se necesitan con urgencia otras estrategias para ampliar el acceso a los servicios de salud reproductiva entre las poblaciones desplazadas internamente. En Birmania oriental, debido al conflicto continuo y la falta de sistemas de salud en buen estado de funcionamiento, resulta inviable poner énfasis en la prestación de servicios en establecimientos con asistentes calificados. A lo largo de la frontera entre Tailandia y Birmania, organizaciones locales implementaron un piloto innovador, el Proyecto de Trabajadores de Salud en Cuidados Obstétricos Móviles (MOM, por sus siglas en inglés), y así establecieron una red colaboradora de tres niveles de trabajadores comunitarios en salud reproductiva. Los trabajadores de salud de organizaciones locales recibieron capacitación práctica en cuidados obstétricos de emergencia, así como transfusión sanguínea, atención antenatal y planificación familiar, en un establecimiento central. Después de regresar a sus respectivas comunidades en Birmania, estos trabajadores de primer nivel en salud materna capacitaron a un segundo nivel de trabajadores de salud locales y a un tercer nivel de parteras tradicionales para que proporcionaran un subconjunto limitado de estas intervenciones, de acuerdo con su nivel de capacitación. En este proyecto en curso, la comunicación estrecha entre los trabajadores de salud y las parteras tradicionales fomenta aceptación y cobertura de los servicios de maternidad por toda la comunidad. Describimos las justificación, el diseño y la implementación del proyecto y un plan de monitoreo paralelo para la evaluación del proyecto. Esta innovadora estrategia de prestación de servicios obstétricos puede servir de modelo para la otros servicios de salud esenciales en esta población y para ampliar el acceso a la atención médica en otros ámbitos en conflicto.
In eastern Burma, decades of conflict between the military junta and ethnic minority groups has resulted in approximately 560,000 internally displaced persons.Citation1Citation2 In areas known as “black zones”, the junta attempts to cut off food, funding and information, and recruits through extensive human rights violations such as forced displacement, forced labour and destruction of food supplies. Over 3,000 villages in eastern Karen state have been destroyed since 1996.Citation1 These violations and associated high child and infant mortality rates have been well documented.Citation3Citation4 Such conditions present substantial logistical barriers to health care delivery through standard models (the national health system is ranked 190th out of 191Citation5), and have severely curtailed the ability of international non-governmental organisations to provide humanitarian assistance.Citation6Citation7 The 2005 withdrawal from BurmaFootnote* of the Global Fund to Fight AIDS, Tuberculosis and Malaria and other major international non-governmental organisations (Medicines sans Frontières France, International Committee of the Red Cross) highlights the need for alternative strategies to reach internally displaced persons in the border regions.Citation8
In the past decade, due to efforts led by the Inter-Agency Working Group on Reproductive Health in Crisis (IAWG)Footnote† and the Reproductive Health Response in Conflict Consortium, the international community has begun to recognise the impact that conflict has on women’s reproductive health outcomes and the need for specific interventions to address these vulnerabilities. In conflict settings, women are disproportionately affected and have poorer pregnancy outcomes than women living in stable areas.Citation9 While improvements have been made with regard to refugee care, much less progress has been made for internally displaced persons,Citation10 and reproductive health services are normally unavailable in these unstable settings.Citation10Citation11 Improving access to critical services in such settings, however, is possible. For example, the Reproductive Health Response in Conflict Consortium, in collaboration with the Averting Maternal Death and Disability Program at Columbia University, has recently demonstrated the feasibility of strengthening facility-based emergency obstetric services in 12 conflict-affected settings.Citation12
On the Thailand–Burma border, organisations such as the Karen Department of Health and Welfare and the Back Pack Health Worker Team support a range of health programmes for internally displaced persons in eastern Burma, and are cognizant of the substantial burden of adverse reproductive health outcomes occurring within their target communities. The maternal mortality ratio for this region has been estimated at approximately 1,200 per 100,000 live births,Citation13 and stands in stark contrast with neighbouring Thailand, whose maternal mortality ratio is 44.Citation14 Initial efforts to reduce the risk of maternal mortality focused on training programmes for traditional birth attendants (TBA). While these programmes provided basic materials and educational messages on clean delivery and recognition of danger signs during pregnancy, capacity to provide emergency obstetric care, a primary intervention for preventing maternal mortality and morbidity, was lacking.
Recognising this limitation and the urgent need for new approaches relevant to their setting, in August of 2005 these border-based organisations decided to pilot a unique delivery model of an integrated package of selected maternal and newborn health and family planning interventions. The project aims to increase access to proven interventions among internally displaced persons by developing capacity among a cadre of mobile maternal health workers who could provide a more comprehensive approach to reproductive health services. This Mobile Obstetric Maternal Health Workers (MOM) Project is a collaborative effort between the Johns Hopkins Center for Public Health and Human Rights in the USA, Mae Tao Clinic (a training centre for hundreds of health workers from eastern Burma), Burma Medical Association, Global Health Access Program in the USA, and local Burmese health organisations. This paper describes the rationale for this innovative model of delivering maternal health and family planning services, provides an overview of the programme structure, training and roles of the health care providers in the project, and outlines the planned monitoring and evaluation activities.
Context, key approaches and rationale of the MOM Project
The significance of the MOM Project is perhaps most evident when viewed from within the current international maternal health policy context, where it emerges as a meaningful response to unresolved problems in reaching populations in conflict settings. Leading voices in the international debate on the most appropriate strategies to improve reproductive health largely focus upon skilled attendants providing facility-based services,Citation15Citation16 e.g. in the recent Lancet series on maternal mortality and morbidity.Citation17 Increasing the proportion of women delivering in a facility with a skilled attendant and access to comprehensive emergency obstetric careCitation16 are also long-term goals for communities in eastern Burma. Meaningful efforts towards these goals, however, will only be possible after the cessation of violence and progress towards reconciliation.
For example, the Karen Department of Health and Welfare’s experience indicates that immobile facilities in the conflict zones of Burma would likely face destruction or displacement in short order. Since 1998, of the 33 clinics that Karen Department of Health and Welfare oversees, 11 have been forced to relocate, five of them between October 2006 and April 2007. Since permanent structures are more likely to be destroyed, the Department must instead operate their clinics as “mobile”, semi-permanent structures that can be rapidly dismantled when threatened by conflict. Further, a central facility model in this environment would only provide real access to care for the few thousand people residing in the immediate surrounding area. The populations served by the Department are subject to frequent displacement, with nearly one in ten displaced per year,Citation4 Citation13 and over 3,000 villages destroyed or relocated since 1996.Citation1 A mobile clinic can shift with these population movements, whereas a stationary facility would be abandoned. Additionally, security constraints, lack of infrastructure and a widely dispersed population result in extremely long transit times for patients, who mostly travel on foot. A centralised facility would require patients to overcome great obstacles to reach care. Thus, permanent facilities are unfortunately not currently a viable option in this setting.
The MOM Project has also had to provide maternal health care under circumstances where there is no foreseeable access to skilled birth attendants, as defined by the WHO, whose definitionCitation18 explicitly excludes non-accredited individuals, even if they are able to provide interventions that improve pregnancy outcomes. Consideration of roles for other types of providers not explicitly meeting this definition could reduce the acute shortage of health personnel, especially in communities with failed or non-existent health systems.Citation19Citation20 Given the substantial barriers in eastern Burma and other similar conflict settings, alternative context-specific strategies to facility-based and skilled attendant care are urgently required.Citation21
Adhering to international policy as closely as possible, given these obstacles, the MOM Project, a three-year pilot was launched in August 2005 in 12 target communities of internally displaced persons in four states (Mon, Karen, Karenni and Mon) of eastern Burma (). A three-tiered collaborative network of community-based maternal health workers was established, in which health workers from local organisations received practical training in basic emergency obstetric care, evidence-based antenatal care and family planning at a central facility. These specially-trained maternal health workers returned to their communities to train a second tier of local health workers and a third tier of traditional birth attendants (TBAs). This approach aims to increases the overall coverage of pregnancies attended by individuals with the capacity to provide at least one component of basic emergency obstetric care, antenatal care or family planning. This is achieved by implementing basic interventions through the less-trained providers, and more complex interventions through the higher-trained providers, all of whom strive to provide highly mobile services to women at the village level, either in rudimentary mobile clinics or, more often, at home. The emphasis on mobility and bringing services to women’s homes allows the services to rely less on facilities and to move with villagers in the event of population displacement. Such emphasis in the development of the MOM project is relevant and necessary for any future scale up to a broader population where forced displacement is consistently reported.Citation4 Citation13
Figure 1 Map of eastern Burma showing approximate location of 12 MOM Project pilot sites

The project consists of two main phases: Phase 1 (Design/Training – August 2005 to September 2006) including selection of sites and workers, development of curricula for each of the three levels of worker, and a six-month training phase for maternal health workers, followed by shorter training for local health workers and TBAs when maternal health workers have returned to the field. Phase 2 (Implementation (ongoing) – October 2006 to September 2008) was initiated in late 2006, with the network of workers actively identifying pregnant women, providing a range of antenatal services, attending births, providing postpartum care to both mother and newborn, and delivering family planning services. A parallel monitoring and evaluation component to the project collects information through a range of qualitative and quantitative approaches.
Organisational structure and target populations
In August 2005, members of the Mae Tao Clinic, Burma Medical Association and local ethnic health departments from Shan, Mon, Karenni and Karen states met at MOM Project headquarters in the border town of Mae Sot, just inside Thailand, to discuss the programme components and finalise implementation plans. Local partners were joined by representatives from long-term technical assistance partners in the USA, including the Johns Hopkins Center for Public Health and Human Rights and Global Health Access Program. A Steering Committee was established with representatives from each of the participating organisations to provide overall strategic direction and oversee implementation. The actual implementation of the project is directed by a team of local project coordinators and staff drawn from the Mae Tao Clinic, Karen Department of Health and Welfare and Burma Medical Association.
A range of target communities were selected for inclusion in the pilot phase based on a number of criteria. First, the participation of four ethnic communities was encouraged to foster collaboration and enhance the relevance of the model for eventual scale-up in an ethnically diverse region. Second, sites within the four communities were selected based on their catchment population (4,000–8,000), lack of basic emergency obstetric services and the availability of health workers for training. Additionally, sites were considered if they had: 1) support from the local health department and village leaders, 2) sufficient numbers of candidate health workers who could be trained as maternal health workers and available local health workers to be trained in a subset of these skills, and 3) an already existing mobile clinic under the management of the local health department.
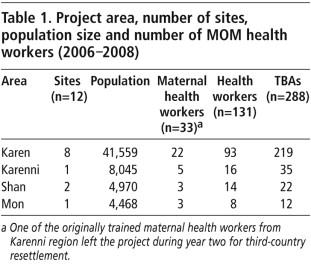
Twelve sites (eight Karen, two Shan, one Mon, one Karenni) were selected, with an estimated total population of 60,000 (Table 1). While indicators specific to the selected pilot areas have not been published, retrospective household surveys in a broader area of eastern Burma, including Karen, Karenni, and Mon regions, indicate high infant (89 per 1,000 live births), child (218 per 1,000 live births) and maternal mortality (1,200 per 100,000 live births), and crude birth rates of 35–45 per 1,000 population.Citation3,4,13
Selection of health workers
The Steering Committee developed selection criteria for the three provider levels, with one maternal health worker per 2,000 persons, one health worker per 500 and one TBA per 200. For each site, ethnic health leaders chose 1–4 maternal health workers directly from the community; each of whom had completed some prior training (usually 6–12 months), had some working experience and wrote and spoke Burmese (in addition to their own ethnic language). The selected maternal health workers received specialist training in Thailand. From among these, a team leader was selected to manage inventory of supplies, supervise field activities of other maternal health workers, health workers and TBAs, and data collection, maintain contact with the ethnic health departments and MOM project staff in Mae Sot, and return to Thailand every six months to retrain. Ethnic health leaders also selected 4–20 local health workers per site who were required to have some basic health training and experience providing services in their community. Maternal health workers and local health workers were asked to commit to three years of fieldwork. TBAs were identified from among those actively attending births and recognised by their community as someone to call upon for antenatal care, delivery, post-natal or other reproductive health services. Experience and background training were not considered in the selection of TBAs.
Maternal health worker training
Training the identified maternal health workers was the primary capacity-building activity during Phase I. A total of 33 maternal health workers were trained: 30 women and three men. Prior to the MOM training, all trainees had completed at least four months of basic health training, with the majority having had a six-month course. Almost all workers (30) had completed two years of fieldwork, with 11 trainees having over five years’ experience and one having worked for 20 years as a medic. All had completed the sixth standard of education, with 23 having reached tenth standard or, equivalently, completed secondary school education.
Their training included both classroom and practical components. The Steering Committee and project coordinators designed the curriculum, drawing upon guides and manuals by the World Health Organization (WHO), UN Population Fund (UNFPA), US Agency for International Development, JHPIEGO, International Federation of Gynecologists and Obstetricians, Reproductive Health Response in Conflict Consortium and Averting Maternal Death and Disability Project,Citation22Citation23 and advice from members of an external advisory committee. Guidelines were also adapted to take account of context-specific logistical constraints (e.g. lack of refrigeration) and cultural and political sensitivities (e.g. ethnic health leaders decided that counselling for and promotion of family planning should initially be directed to married women only). The final component of the capacity-building was in participatory educational methods, including: 1) training-of-trainers to enable maternal health workers to transfer their knowledge and skills to the other tiers of providers when back in Burma, and 2) small group discussions and role-play to increase effective communication with community members through counselling and to dispel community misconceptions (e.g. about contraceptive methods).
The classroom training focused on familiarising the trainees with basic maternal health knowledge, including evidence-based antenatal care, normal and complicated deliveries, post-natal and post-abortion care, neonatal care and resuscitation, and family planning. The two-month training consisted of six hours per day for a total of 198 classroom hours, and included lectures, case studies, role-play and clinical simulations. Classroom training was then followed by four months of hands-on experience gained through intensive participation in provision of maternal health and family planning services at Mae Tao Clinic, with over 2,000 deliveries per year, under the supervision of local senior reproductive health workers and expatriate physicians.
The practical portion emphasised skills development for blood transfusion and the six basic emergency obstetric procedures: antibiotics, parenteral magnesium, manual removal of placenta, manual vacuum aspiration, misoprostol for prevention and treatment of post-partum haemorrhage and vacuum extraction. Full implementation of vacuum extraction was delayed because of the relative difficulty of the procedure, lack of experience among senior Mae Tao Clinic medics in the use of portable devices such as the Kiwi OmniCup® vacuum extractor, and considerable effort and time being needed for the other five components. Trainees rotated through labour and delivery and outpatient and inpatient reproductive health departments, with exposure to specific interventions tracked for each trainee. Outpatient maternal and newborn health exposure included training in clean and safe delivery, antenatal and post-natal care, and post-abortion care, and emphasised the effective delivery of essential interventions such as iron folate supplementation, malaria screening and treatment during pregnancy, insecticide-treated nets, de-worming of mothers, and birth preparedness counselling, including nutrition and essential newborn care. Family planning training included counselling and education on provision of modern contraceptive methods, including male condoms, contraceptive injection, oral contraceptive pills and emergency contraception.
Blood transfusion is normally considered a component of comprehensive emergency obstetric care only performed at facilities capable of caesarean section.Citation16 However, blood transfusion was included for two reasons. First, in this population high rates of anaemia and especially malariaCitation3 increase the likelihood of severe morbidity and mortality from post-partum haemorrhage.Citation24 Second, the transfusion component of the MOM Project was adapted from an existing protocol developed to care for patients at Karen Department of Health and Welfare clinics who were severely anaemic from trauma or other causes. This protocol takes advantage of recent progress made in the development of heat-stable rapid diagnostic tests to screen blood for malaria, syphilis, hepatitis B and C, and HIV. Because of the inability to store blood in the field, maternal health workers conduct community education about the need for blood transfusions in advance, and recruit prospective donors from community volunteers, thus maintaining a “walking blood bank”. When needed, they can request donors with matching blood type, conduct confidential screening, and give appropriate counselling and treatment as needed.
Periodic follow-up information-sharing and training workshops are scheduled throughout the MOM project. For all maternal health workers these require a return to Thailand annually and for team leaders, every six months. Follow-up training allows time for review of clinical work in the field, discussed below, supplemented with practical training and supervision in the reproductive health department at Mae Tao Clinic. This is also an opportunity to coordinate logistical arrangements for re-supplying areas and for the MOM office staff to review data collection tools and make updates. Finally, periodic reviews of progress and capabilities of maternal health workers allow for the addition of new training modules and new interventions in the existing platform.
Health worker training in the field
Returning to the field sites in June 2006 was a lengthy process, with some maternal health workers requiring up to six weeks to reach their target communities, as security constraints postponed movement or forced circuitous routes. Upon arrival, the maternal health workers conducted a series of meetings with local authorities, village heads, religious leaders, traditional healers, women’s and other civil society groups, and local health workers and TBAs, to explain the programme. The meetings followed an informal, participatory approach, allowing stakeholders to offer opinions and make recommendations. This process of informing and sensitising the community was envisioned as a necessary and appropriate step to secure support for the project.
Community leaders then recruited health workers at each site. Maternal health workers conducted two-month trainings for a total of 131 health workers, aged 18–30 years old, mostly unmarried women, all of whom had some prior health training and experience. The training was based on the maternal health workers’ curriculum, but included only provision of antibiotics for sepsis and administration of misoprostol for prevention of post-partum haemorrhage from the components of emergency obstetric care. Eventually, however, health workers will learn all aspects of basic emergency obstetric care and blood transfusion through continued regular training and experience working with maternal health workers in the field.
During field activities, maternal health workers rely on health workers to assist in achieving the goal of having, at every birth, no matter the location, an attendant with the capacity to provide basic emergency obstetric care. Employing communication strategies such as regular meetings between the maternal health workers and health workers and monitoring of expected delivery dates increases the likelihood of a maternal health worker in attendance. Attendance at birth by a maternal health worker is the primary objective, but when movement is restricted, primarily due to security concerns, the health workers trained in the more limited set of basic emergency obstetric care components are an option. The greater number of health workers compared to maternal health workers (average 4:1 ratio), facilitates greater dispersion of emergency obstetric services throughout the target area.
TBA training in the field
The communities of eastern Burma have an informal network of TBAs who provide some care to the vast majority of pregnant women. Following recommendations from UNFPA, WHO and others,Citation14 TBAs are supported in the MOM Project as playing a crucial role in strengthening the link between pregnant women and the maternal health and other health workers. However, recognising 1) the importance of TBAs who have early contact with pregnant women, 2) the scarcity of human resources and 3) lack of facilities, TBAs in the MOM Project are also called upon to provide the most basic components of antenatal, delivery and post-natal care.
Maternal health workers conducted 22 TBA trainings for 288 TBAs recruited by community leaders. Previous training was not a requirement for TBAs to participate, and their prior experience and training varied substantially. The TBA training followed a seven-day curriculum centred on evidence-based antenatal care, essential newborn care, clean delivery and the importance of their role in strengthening communication and working effectively with maternal health workers and health workers.
Service provision
The transition to the second phase began in each area when maternal health workers had completed training health workers and TBAs. Pregnant women are most commonly identified first by TBAs, who inform them about the MOM project and the additional services available through maternal health workers and health workers. These services can be broadly grouped into antenatal, labour and delivery (including basic emergency obstetric care), and post-natal and other services. Primary responsibility for delivering these interventions is distributed through the three-tiered network (Table 2).
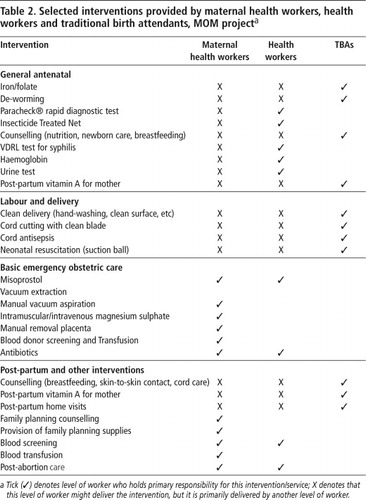
TBAs also inform health workers and maternal health workers directly about all pregnant women identified in their areas. Identification of a pregnant woman prompts a series of antenatal care services provided directly by the network of workers during home visits, including malaria screening with the Paracheck® rapid diagnostic test (Orchid Biochemical Systems, Goa, India), and provision of long-lasting, insecticide-treated nets, de-worming pills and specific counselling on nutrition, birth preparedness and preparation for care of the newborn, breastfeeding and family planning. Depending on which tier of worker is present at the time of delivery, women have access to: safe and clean delivery (with TBAs); antibiotics, if needed, and misoprostol plus safe and clean delivery (with health workers); or the full range of basic emergency obstetric care services (with maternal health workers). These services may be provided at the central site or, more usually, the woman’s home. While one of the overarching goals is to increase the proportion of women delivering with the assistance of a maternal health worker, this is not always possible. In cases where a health worker or TBA is responsible for assisting the delivery, referral to the maternal health worker might occur for any complications. Referral to maternal health workers (by word of mouth) might result in either the maternal health worker going directly to the woman’s home or the woman travelling to the local mobile clinic. There are no MOM pilot areas that can reliably refer to facilities where caesarean section is available. After delivery, regular post-natal visits take place in which attendees check both mother and neonate, providing family planning supplies, treatment for infection, post-partum vitamin A, promotion of essential newborn care, early and exclusive breastfeeding, nutrition counselling, and recognition of signs of severe illness. In addition, MOM workers are able to provide family planning during antenatal care or post-natal or post-abortion visits.
Supervision
Activities and service provision by health workers and TBAs are overseen by the maternal health workers and the maternal health workers’ team leader in each site. Direct supervision of these workers is not possible by the MOM staff in Mae Sot or by members of the Steering Committee, as security constraints substantially limit travel. Thus while periodic field visits are made as part of the qualitative monitoring and evaluation components (see Monitoring and Evaluation, below), oversight of TBAs and health workers is largely done by maternal health workers during day-to-day direct observation of their work and through periodic follow-up trainings. Maternal health workers themselves are supervised first by their team leader during ongoing implementation of field activities, and by MOM Project staff during annual follow-up trainings.
Remuneration
Compensation levels for all workers are decided in accordance with the policies of the ethnic health organisations. Maternal health workers and health workers are both paid a monthly stipend for their work in the field, in addition to a monthly food allowance, which in some cases is combined with existing funds at the clinic level to provide food for all health workers in the clinic. TBAs receive a per diem allowance during both initial and follow-up training sessions. Survey team members receive similar compensation during the time in which they are conducting surveys in the field (typically a two-month period).
Monitoring and evaluation: quantitative methods
Evaluation of the MOM project is conducted through collaboration between the technical assistance partners, Global Health Access Program and the Johns Hopkins Center for Public Health and Human Rights. Quantitative components include annual, population-based, cluster-sample surveys (conducted by a separate group of data collectors) and three periodic reviews (baseline, interim and endline) of pregnancy-tracking logs and other data forms that are routinely collected by the three cadres of MOM workers.
Analysis of the cluster sample surveys (baseline completed in late 2006, interim and endline surveys to be completed in January 2008 and December 2008, respectively) will enable assessment of access over time to a range of interventions offered by the MOM project. The surveys include questions on background and demographic variables, pregnancy history, antenatal care coverage, including access to malaria and anaemia screening, iron/folate supplementation, de-worming, distribution of long-lasting insecticide-treated nets, number of antenatal care visits, and knowledge of family planning methods, current use and unmet need. The latter will help the MOM project direct family planning services in the target population.
These surveys also include questions on vital events and human rights violations experienced at the individual and household level. Rights violations to be monitored in this setting include forced displacement, destruction or theft of household food supplies, forced labour of household members by the Burma military, direct physical attack by troops and landmines. This methodological approach has been previously describedCitation4 and will allow estimation of important associations between access to MOM project components and human rights violations. Rape as a tool of the military junta, particularly in Shan State, has been well documented.Citation25 Questions on rape are not, however, included in the current modules of the MOM project as gender congruence between surveyor (independent from MOM project workers) and respondent is not guaranteed and the limited length and time frame allowed for each interview is not conducive to establishing the level of trust required to adequately collect such sensitive information.
These surveys will also allow estimation of neonatal and infant mortality rates,Citation3 but as they will cover only about 2,800 households per survey period, they are not a priori powered to detect any changes in mortality risk during the MOM project period. The survey workers recruited as part of the MOM survey team are from the village-based clusters to which they are assigned, but are separate from the three tiers of MOM project health providers. Given the uncertain security environment of the target populations, the inclusion of members of the internally displaced community as part of the monitoring team is essential to increased overall acceptance and participation by community members.
In addition to the cluster-sample surveys, periodic review of pregnancy-tracking logs routinely filled by maternal health workers and health workers will provide further information regarding the access to antenatal care, labour and delivery, and post-natal interventions. For each pregnancy attended by a maternal health worker and/or health worker in the programme areas, a pregnancy record is generated for tracking the progress of women from pregnancy through post-partum care. Clinical records will provide indicators, including of access to maternal health services (antenatal, peripartum, post-natal), components of basic emergency obstetric care and family planning uptake. These charts will also facilitate estimation of the proportion of total deliveries attended in catchment areas attended by MOM workers, and the proportion of births requiring each emergency obstetric intervention. The extraction of data from these pregnancy records will also allow comparison of health outcomes between areas and over time. These include post-partum haemorrhage, puerperal sepsis, abortion complications, malaria during pregnancy, and case-fatality rates for pregnancy complications managed by MOM health workers. Early neonatal mortality will also be estimated from these pregnancy records and provides an opportunity for internal validation of the neonatal mortality data estimated from the cluster-sample surveys described above.
TBAs are also involved in project monitoring and evaluation through the use of basic forms in a prospective manner to collect information on pregnancies, live births and deaths during the first week of life. These simple, picture-based forms have been developed and implemented in a range of Thai/Burma border TBA programmesCitation26 and are based on previous picture-based forms used in community programs in Cambodia and Vietnam. This third source of data on vital events provides yet another point for triangulation of data, furthering internal validation. In this internal displacement setting, opportunities for real-time supervision of data collection and other monitoring and evaluation tasks is limited, and such replication of data is essential for gaining confidence in the estimation of outcome indicators.
Monitoring and evaluation: qualitative methods
Qualitative methods of monitoring and evaluation during follow-up trainings in 2007 and 2008 for maternal health workers in Thailand will include a series of focus group discussions to collect information on barriers to provision of care, challenges arising during project implementation, and to strategise how to overcome these obstacles. The broad topics to be discussed include relationships with the community, health workers and TBAs, problems and successes in the delivery of obstetric interventions, supplies and communication, using case reports. Such reports might include particularly difficult or complicated cases, including maternal death. Experience with managing such cases will be shared, and, in the absence of a more formal approach (e.g. maternal death audit), will help highlight areas to be further addressed during follow-up training.
Periodic site visits by local members of the MOM Steering Committee will also be conducted to each of the service delivery areas, primarily to supplement information provided through communications between field workers and local MOM staff. Information collected during these visits will include updates on logistical and implementation challenges, assessment of the level of activities and interventions provided, and changes in the security situation. They will not be used for evaluation purposes due to difficult and fluid security constraints, resulting in irregularity of visits, but also because verbal assessments by project workers are subjective in nature and short visits cannot capture all the activities being implemented.
Conclusions
The two key features of the MOM Project are as follows. The first is the necessity of unbundling health care from facilities, because of the constraints inherent in conflict settings. This was illustrated in eastern Burma during the devastating 2006–2007 escalation of the conflict in northern Karen State. The military junta forced the already displaced population of one of the MOM Project sites (Na Yo Hta) to scatter once more into the surrounding jungle.Citation27 The central site being used by maternal health workers for coordination of activities, supplies and training was burned by the military. MOM project workers moved with the population and provided services during four months of displacement due to active fighting. Continuity of care and delivery of services under such conditions can only be achieved within a structure that emphasises mobility of service provision to the population, rather than centralised services that must be accessed by the population.
The second key feature is that all components of pregnancy and delivery care are provided by the more intensively trained maternal health workers, while lesser-trained workers still contribute to overall coverage by providing a crucial subset of interventions. This model creates the flexibility necessary to provide community-based service delivery. Given the substantial burden of mortality and morbidity facing women in this setting, this approach may have an important public health impact despite the limitations and even without comprehensive care (such as caesarean section).
This approach reflects the realistic constraints of the setting, recognises the integral role of a variety of care providers, including TBAs, and promotes a tiered-structure that may facilitate the progressive realisation of more standard comprehensive models of reproductive health services. A more comprehensive approach, for example, would move beyond the current MOM focus on maternal health services and family planning to include efforts to reduce sexually transmitted diseases, HIV/AIDS and gender-based violence, as recommended by the Inter-Agency Working Group on Reproductive Health in Crisis.Citation28 The forthcoming evaluation of this programme will provide important insights into the feasibility and effectiveness of this approach and may help guide the development of further strategies for increasing access to care in other conflict settings
A MOM Project maternal health worker provides post-natal care during a home visit in the Mon pilot community

Acknowledgements
The MOM Project is funded by grants from the Bill and Melinda Institute for Population and Reproductive Health at the Johns Hopkins Bloomberg School of Public Health, Global Health Access Program/Planet Care, the Hussman Foundation, and the Foundation for the People of Burma.
Notes
* Burma is also known as Myanmar. We use Burma throughout this report in accordance with the preference of the 1990 General Elector winner, the National League for Democracy.
† IAWG was formerly known as the Inter-Agency Working Group on Reproductive Health in Refugee Settings.
Related Research Data
References
- Thai Burma Border Consortium. Internal Displacement in Eastern Burma: 2006 Survey. TBBC, November 2006.
- Internal Displacement Monitoring Centre. Internal Displacement: Global Overview of Trends and Developments in 2006. 2007; Norwegian Refugee Council: Geneva, Switzerland.
- TJ Lee, LC Mullany, AK Richards. Mortality rates in conflict zones in Karen, Karenni, and Mon states in eastern Burma. Tropical Medicine and International Health. 11(7): 2006; 1119–1127.
- LC Mullany, AK Richards, CI Lee. Population-based survey methods to quantify associations between human rights violations and health outcomes among internally displaced persons in eastern Burma. Journal of Epidemiology and Community Health. 61: 2007; 908–914.
- UN Development Programme. Human Development Indicators. Human Development Report. 2001; UNDP and Oxford University Press: New York.
- C Beyrer, V Suwanvanichkij, LC Mullany. Responding to AIDS, TB, malaria and emerging infectious diseases in Burma: dilemmas of policy and practice. PLoS Medicine. 3(10): 2006; e393–e400.
- E Stover, V Suwanvanichkij, A Moss. The Gathering Storm: Infectious Diseases and Human Rights in Burma. 2007; Human Rights Center, University of California: Berkeley.
- Global Fund to Fight AIDS, Tuberculosis and Malaria. Termination of grants to Myanmar. 2005; GFATBM: Geneva. At: <www.theglobalfund.org/en/media_center/press/pr_050819_factsheet.pdf. >. Accessed 30 August 2007.
- T McGinn. Reproductive health of war-affected population: what do we know?. International Family Planning Perspectives. 26(24): 2000; 174–180.
- UN High Commissioner for Refugees. Inter-Agency Working Group on Reproductive Health. Inter-Agency Global Evaluation of Reproductive Health Services for Refugees and Internally Displaced Persons. 2004; UNHCR: Geneva.
- Reproductive Health Response in Conflict Consortium. The Field-Friendly Guide to Integrate EmOC in Humanitarian Programs. 2005; Women’s Commission for Refugee Women and Children: New York.
- SK Krause, JL Meyers, E Friedlander. Improving the availability of emergency obstetric care in conflict-affected settings. Global Public Health. 1(3): 2006; 205–228.
- Backpack Health Worker Team. Chronic Emergency: Health and Human Rights in Eastern Burma. 2006. At: <www.jhsph.edu/humanrights/ChronicEmergency_BPHWT_Report2005.pdf. >. Accessed 15 August 2007.
- World Health Organization. World Health Statistics 2007. 2007; WHO: Geneva.
- World Health Organization. World Health Report 2005: Make Every Mother and Child Count. 2005; WHO: Geneva.
- UN Population Fund. Maternal Mortality Update 2002: A Focus on Emergency Obstetric Care. 2003; UNFPA: New York.
- V Filippi, C Ronsmans, OM Campbell. Maternal health in poor countries: the broader context and a call for action. Lancet. 368(9546): 2006; 1535–1541.
- World Health Organization. Making pregnancy safer: the critical role of the skilled attendant: a joint statement by WHO, ICM and FIGO. 2004; WHO: Geneva.
- World Health Organization. World Health Report 2006: Working Together for Health. 2006; WHO: Geneva.
- M Koblinsky, Z Matthews, J Hussein. Maternal Survival 3: Going to scale with professional skilled care. Lancet. 368: 2006; 1377–1386.
- A Costello, K Azad, S Barnett. An alternative strategy to reduce maternal mortality. Lancet. 368(9546): 2006; 1477–1479.
- World Health Organization. Managing Complications in Pregnancy and Childbirth: A Guide for Midwives and Doctors. WHO/RHR/00.7. 2003; WHO: Geneva.
- Averting Maternal Death and Disability. Emergency Obstetric Care for Doctors and Midwives. May 2003. At: <www.reproline.jhu.edu/english/2mnh/2obs_care/EmOC/index.htm. >. Accessed 22 August 2007.
- KS Khan, D Wojdyla, L Say. WHO analysis of causes of maternal death: a systematic review. Lancet. 367: 2006; 1066–1074.
- Shan Human Rights Foundation, Shan Women’s Action Network. License to Rape: the Burmese military regime’s use of sexual violence in the ongoing war in Shan State. Chiang Mai, 2002.
- Mullany LC. Developing methods to estimate population-level health indicators among IDP communities in eastern Burma. Presented at: Public Health and Human Rights in the Era of AIDS: An International Seminar, Johns Hopkins Bloomberg School of Public Health, Baltimore MD. 7–9 April 2004.
- Karen Human Rights Group. SPDC military begins pincer movement, adds new camps in Papun district. News Bulletin #2006-B10, 2006. At: <www.khrg.org/khrg2006/khrg06b10.pdf. >. Accessed 30 August 2007.
- UN High Commissioner for Refugees Inter-Agency Working Group on Reproductive Health. Reproductive Health in Refugee Situations: An Inter-Agency Field Manual. 1999; UNHCR: Geneva.