Abstract
Second trimester abortion is associated with higher rates of complications compared to first trimester abortion. Dilatation and evacuation (D&E) and medical induction using misoprostol alone or a combination of mifepristone and misoprostol are the methods most commonly used for later abortion in developed countries, yet little research has directly compared them. We reviewed the literature on PubMed and identified only one small randomised controlled trial and one retrospective cohort study with comparative data for these methods, although the cohort study did not include cases using the mifepristone regimen. We expanded our search to include case series and cohort studies for a single method. In the randomised trial, women undergoing medical induction reported significantly more pain and experienced more adverse events. In the cohort study, incomplete abortion was significantly more common among women undergoing medical induction. In the single method studies, serious complications such as uterine perforation, uterine rupture and haemorrhage were rare, although the latter may be more common with medical induction. Mild infection may also be more prevalent after medical induction. Current evidence suggests that, given trained providers and where otherwise feasible, D&E is preferable to medical induction. A larger randomised controlled trial is needed that directly compares outcomes between the two methods, examines acceptability to women and explores clinicians' perspectives on providing them.
Résumé
L'avortement du deuxième trimestre est associé à des taux plus élevés de complications que l'avortement du premier trimestre. La technique de la dilatation et évacuation et l'induction médicamenteuse avec le misoprostol seul ou en associant mifépristone et misoprostol sont les méthodes les plus fréquemment utilisées pour l'avortement tardif dans les pays développés, pourtant peu de recherches les ont directement comparées. Nous avons passé en revue la documentation sur PubMed et identifié un seul petit essai contrôlé randomisé et une étude rétrospective de cohorte avec des données comparées pour ces méthodes, même si l'étude de cohorte ne comprenait pas de cas utilisant la mifépristone. Nous avons élargi notre recherche pour y inclure des séries de cas et des études de cohorte sur une seule méthode. Dans l'essai randomisé, les femmes avortant par induction médicamenteuse ont signalé sensiblement plus de douleurs et d'effets indésirables. Dans l'étude de cohorte, les avortements incomplets étaient nettement plus fréquents pour l'induction médicamenteuse. Dans les études portant sur une seule méthode, les complications graves comme la perforation ou la rupture utérine et l'hémorragie étaient rares, bien que cette dernière soit plus courante avec l'induction médicamenteuse. Les infections légères semblent aussi plus nombreuses après l'avortement médicamenteux. Les données disponibles suggèrent qu'avec du personnel formé et quand c'est faisable, la technique de la dilatation et évacuation est préférable à l'avortement médicamenteux. Un essai randomisé contrôlé plus vaste est nécessaire pour comparer directement les résultats des deux méthodes, examiner leur acceptabilité par les femmes et étudier les perspectives des cliniciens qui les pratiquent.
Resumen
El aborto en el segundo trimestre está asociado con tasas más altas de complicaciones que las del primer trimestre. Aunque en los países desarrollados se utiliza más la dilatación y evacuación (D&E) y la inducción médica con misoprostol solo o una combinación de mifepristona y misoprostol para el aborto tardío; pocas investigaciones los han comparado directamente. Al revisar el material en PubMed, encontramos sólo un pequeño ensayo aleatorizado y un estudio de cohorte retrospectivo con datos comparativo s para estos métodos, aunque en el estudio de cohorte no se incluyeron casos donde se utiliza el regimen de mifepristona. Ampliamos nuestra búsqueda para incluir series de casos y estudios de cohorte para un sólo método. En el ensayo aleatorizado, las mujeres que se sometieron a la inducción médica informaron considerablemente más dolor y experimentaron más efectos adversos. En el estudio de cohorte, el aborto incompleto era más común entre las mujeres que se sometieron a la inducción médica. En los estudios de un sólo método, rara vez hubo complicaciones graves, como perforación uterina, ruptura uterina y hemorragia, aunque esta última podría ser más común en la inducción médica. Una infección ligera también podría ser más prevalente después de la inducción médica. La evidencia actual indica que, donde se cuenta con prestadores de servicios capacitados y es factible, la D&E es preferible a la inducción médica. Es necesario realizar un ensayo controlado aleatorizado más amplio que compare directamente los resultados entre los dos métodos, examine su aceptabilidad por parte de las mujeres y explore los puntos de vista del personal de salud en cuanto a su práctica.
In developed country settings, although abortion is very safe, mortality following second trimester procedures is higher than after first trimester abortion. In the United States, where abortion-related fatalities are rare, the risk of death has been found to increase significantly with advancing gestation.Citation1 Mortality data from 1988 to 1997 indicate that the mortality rate with abortions performed at eight weeks or earlier was 0.1 deaths per 100,000 legal terminations, and this rate increased to 1.7 deaths per 100,000 abortions performed at 13–15 weeks. The mortality ratio for abortions performed at 16–20 weeks was 3.4 deaths per 100,000 procedures, and 8.9 deaths per 100,000 abortions for those at 21 weeks or later. Although the absolute risk of death was low, the relative risk of death with an abortion performed at 21 weeks or later was more than 75 times higher than the risk associated with an abortion at eight weeks.Citation1 In this series, 85% of abortion-related deaths were due to direct causes – primarily haemorrhage and infection – and approximately 15% were due to indirect causes such as embolism and anaesthetic complications.Citation1
Both surgical and medical abortion techniques can be used in the second trimester of pregnancy. In developed countries, dilatation and evacuation (D&E) and/or medical induction with mifepristone and misoprostol (or misoprostol alone) have become the most common second trimester abortion procedures. In the United States (US), D&E is the norm, while in much of Europe it is medical induction.
D&E is usually a staged procedure. In the first phase of the procedure, the cervix is slowly dilated, usually using hygroscopic dilators such as laminaria or other artificial dilators, or using a prostaglandin such as misoprostol, or a combination of the two. These techniques for cervical dilatation are preferable to direct mechanical dilatation, which has been shown to increase the risk of cervical trauma and uterine perforation.Citation2 In some cases cervical preparation is repeated over a period of 24–48 hours, usually as an outpatient procedure. Following adequate cervical preparation, the amniotic fluid is drained using vacuum aspiration and the fetal and placental tissue are removed in pieces using grasping forceps. In many settings where sonography is readily available, physicians perform the procedure under ultrasound guidance.
Several regimens for second trimester medical induction have been studied, and these were recently compared in a review on the topic.Citation3 The regimen that has been most widely studiedCitation4 involves administering mifepristone 200 mg orally on an outpatient basis, followed 36–48 hours later by admission to the clinic or hospital and administration of misoprostol 800 mcg vaginally. The woman is then given further doses of misoprostol 400 mcg orally as necessary, every three hours, until abortion occurs, to a maximum of four doses. If this is unsuccessful, another oral dose of mifepristone 200 mg is given, followed every three hours by misoprostol 400 mcg administered vaginally to a maximum of five doses. Or, surgical evacuation of the uterus can be carried out instead.
There has been little research directly comparing D&E and modern medical methods using mifepristone alone or mifepristone–misoprostol. One randomised controlled trial compared D&E to intra-amniotic instillation of prostaglandin F2-alpha, a medical method that is no longer widely used. This study found that women undergoing medical induction with this method were significantly more likely than those undergoing D&E to have a complication (RR 5.7, 95% CI 2.1–15.3) and had significantly higher rates of vomiting and diarrhoea compared to D&E patients.Citation5 This paper reviews the limited comparative data on D&E and medical induction with misoprostol alone or mifepristone–misoprostol combined, as well as separate data on both types of procedure, focusing on complications reported. It also suggests areas for further research.
Methods
We searched PubMed in September 2007 using the following keywords: second trimester abortion, mid-trimester abortion, dilation and evacuation, mifepristone and misoprostol. Only English language studies were included. All randomised, controlled trials and comparative cohort studies were included in the analysis. Given the small number of studies found that met our criteria, we expanded our analysis to include cohort studies and consecutive case series that included more than 400 cases for the two methods. Studies that focused on medical methods other than misoprostol or mifepristone–misoprostol were not included. The primary outcomes looked for were uterine perforation or rupture, haemorrhage requiring transfusion, incomplete abortion requiring surgical evacuation, cervical laceration, infection and any other reported complication.
Results
Only one randomised controlled trial was identified that compared outcomes between D&E and mifepristone–misoprostol medical abortion in the second trimester.Citation6 A recent Cochrane review on this topic also identified this study as the only randomised trial comparing D&E to medical induction with the mifepristone regimen.Citation7 Unfortunately, the study, which took place in the US, had difficulty recruiting women who were willing to be randomised. Hence, the study was stopped after one year with only 18 enrolled subjects. Women assigned to receive mifepristone–misoprostol reported significantly more pain than those undergoing D&E (p=0.03). Although there were no statistically significant differences in complications between the two groups, six of nine women randomised to mifepristone–misoprostol had one or more adverse events associated with the procedure, compared to one woman who underwent D&E (RR 6.0, 95% CI 0.9–40.3). In the medical induction group, the complications included the following: three women had retained placental tissue that required instrumental removal; three had a fever greater than 38°C; and one woman delivered a fetus that showed signs of life. One woman had a delayed complication; she returned six days after the procedure and was found to have retained tissue that required a suction curettage. The woman in the D&E group who had complications aborted spontaneously after laminaria were placed; she required removal of the placenta and also experienced superficial burns to her abdomen after using a heating pad for her labour pains. Women undergoing medical abortion reported more symptoms such as nausea, vomiting, dizziness and headache compared to those who had D&E, although these differences were not statistically significant.
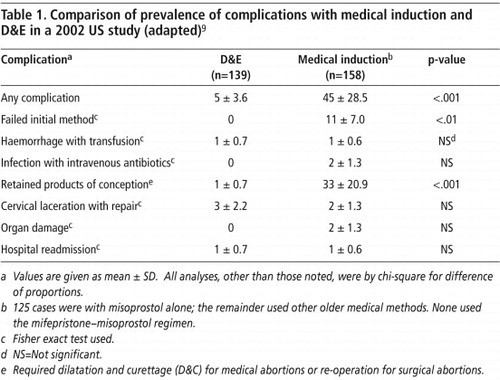
One retrospective cohort study was identified, which compared the outcomes of 139 women who underwent D&E to those of 158 women who underwent medical abortion by any method at two hospitals in the US in 1994–2001.Citation8 For 79% of the women undergoing medical induction, the misoprostol-alone regimen was used; none received mifepristone. The induction method used in the other 21% of cases was unspecified but can be assumed to be an older method. There were significant differences between the two groups: the medical induction group underwent abortion later in pregnancy than the surgical group (20.3 weeks compared with 18.4 weeks, p≤0.001); the surgical group were more likely to have had laminaria placed to dilate the cervix (92% vs. 65%, p≤0.001); and women undergoing surgical abortion were more likely to have a medical indication for the procedure (4% vs. 1%, p=0.05). Overall, the proportion of women who experienced an adverse event was higher among those undergoing medical induction compared to surgical abortion (29% vs. 4%, p<0.001). As shown in Table 1, of all the specific complications that were recorded, women undergoing medical induction were significantly more likely than those undergoing surgical abortion to experience a failure of their initial abortion method (p<0.01) and to have retained products of conception that required curettage (p<0.001). After controlling for gestational age, gravidity and length of hospital stay, the odds ratio of experiencing an adverse event was significantly lower for surgical abortion compared to medical abortion (OR 0.1; 95% CI 0.0–0.3).
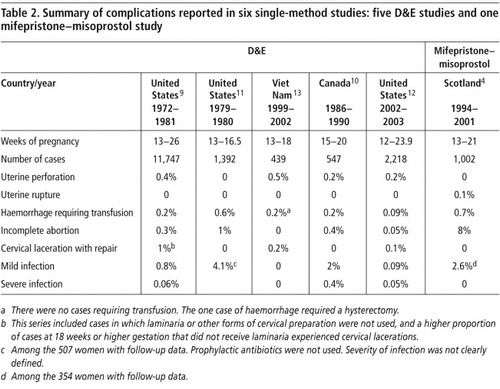
Several studies of more than 400 cases of D&E were identified. The largest included 11,747 cases between 1972 and 1981 in the US.Citation9 Another case series from Canada between 1986 and 1990 included 547 D&E cases at 15–20 weeks of pregnancy.Citation10 Footnote* Another case series from the US reported on 1,392 consecutive D&E cases at 13–16.5 weeks of pregnancy between 1979 and 1980.Citation11 We also included a retrospective cohort study of 2,218 women undergoing D&E with cervical preparation with buccal misoprostol, with or without laminaria, at 19 sites in the US in 2002–2003.Citation12 Another case series from Viet Nam of 439 women undergoing D&E between 1999 and 2002 was also reviewed.Citation13 No cohort studies or consecutive case series with at least 400 women using misoprostol alone were identified. The only case series examining the mifepristone–misoprostol regimen that met the search criteria was from Scotland. It included 1,002 consecutive women undergoing abortion at 13–21 weeks in 1994–2001.Citation4 In the remainder of the paper, we review the complications reported with both D&E and medical induction in these case series. The findings are summarised in Table 2.
Uterine perforation and uterine rupture
Among the D&E studies reviewed, the incidence of uterine perforation was rare. It varied from 0.2% in the most recent study from the USCitation12 and the Canadian study,Citation10 to 0.4% in one of the older US seriesCitation9 and 0.5% in the Viet Nam study.Citation13 The latter two studies with the higher rates of perforation both included physicians with less experience of doing D&E, suggesting that this complication decreases with increasing experience, which has also been shown elsewhere.Citation2 No cases of perforation were reported in the 1979–80 US series, despite the fact that 87% of the procedures were performed by resident physicians in training.Citation11 In other retrospective analyses, the following factors were found to be associated with uterine perforation: under-estimation of the duration of pregnancy, inadequate cervical dilatation and failure to use ultrasound during the procedure.Citation14Citation15
Uterine perforation can also occur in cases of medical induction when the medication fails and a surgical abortion becomes necessary. In the retrospective cohort study in the US, one of the 158 women (0.6%) who underwent an unspecified method of medical induction had a failed procedure, followed by D&E, which was complicated by a uterine perforation that required laparotomy for repair. Another woman in this study, who had had a previous caesarean delivery, underwent induction with vaginal misoprostol and had a uterine rupture requiring urgent laparotomy.Citation8
Uterine rupture has also been reported after medical induction with second trimester mifepristone–misoprostol. In the case series from Scotland, a primiparous woman (0.1%) had a successful induction that was complicated by prolonged haemorrhage requiring laparotomy.Citation4 At the time of laparotomy, a small tear in the uterine wall was noted that needed suturing.
Haemorrhage
Excessive bleeding can occur with both D&E and medical induction. Blood loss with D&E is usually between 100 ml and 400 ml; 0.9% of cases were estimated to have lost more than 500 ml of blood in the largest and oldest case series from the US.Citation9 In this study and the series from Canada,Citation10 0.2% of women required a blood transfusion. In the other older series from the US, four women had immediate haemorrhage requiring transfusion and another four required transfusion at a later date (cumulative incidence 0.6%).Citation11 In the more recent series, a lower proportion of women have required transfusion. In the most recent D&E study from the US included here, six women had haemorrhage of more than 500 ml, of which two (0.09%) required transfusion.Citation12 No cases of blood transfusion were reported in the series from Viet Nam, although one woman required a hysterectomy because of haemorrhage.Citation13 Factors that have been associated with increased blood loss at the time of D&E include increasing gestational age, use of general anaesthesia, prolonged operating time, placenta praevia and placenta accreta.Citation9,16,17 Use of vasopressin in the paracervical block has been shown to reduce blood loss.Citation18
In the case series of medical induction from Scotland, 0.7% of women required blood transfusion. This incidence is higher than that of the D&E studies included here, especially compared to the most recent D&E study that found that 0.09% required transfusion.Citation13 The retrospective cohort study found no significant difference in the proportion of women requiring transfusion among those undergoing D&E compared to those undergoing medical induction.Citation8
Incomplete abortion
Another common cause of excessive bleeding is incomplete abortion. In the retrospective cohort study, as noted above, this complication was found to be significantly more common among women undergoing medical induction.Citation8 In the case series of medical induction with mifepristone–misoprostol, incomplete abortion was noted in 8% of women.Citation4 In the retrospective cohort study, where misoprostol alone or other medical induction methods were used, 19% of women had a failed medical induction.Citation8 These findings are consistent with other studies that have demonstrated that the combined mifepristone–misoprostol regimen results in significantly improved efficacy compared to misoprostol alone.Citation3 However, incomplete abortion after D&E is still far less likely than after medical induction with mifepristone-misoprostol. In the different case series of D&E reported here, the proportion of cases requiring a repeat surgical procedure for incomplete abortion varied from as low as 0.05%Citation12 in the most recent study to 0.3%,Citation9 0.4%Citation10 and 1%Citation11 in the older studies.
Cervical laceration
Cervical laceration can occur after either D&E or medical induction. The retrospective cohort study found no significant difference in the incidence of cervical laceration needing repair among women who underwent D&E compared to those who underwent medical induction.Citation8 In the case series examined, cervical laceration requiring repair was not reported among those undergoing mifepristone–misoprostol induction.Citation6 Cervical laceration was noted in 0.1% and 0.2%Citation14 of women in two of the D&E case series. In the oldest D&E study, cervical laceration (1% of cases) was more common in later gestations, and this was also before the use of laminaria for cervical preparation became routine.Citation9 In the other two D&E case series,Citation11Citation12 there were no cases of cervical laceration requiring repair.
Infection
Antibiotic prophylaxis around the time of surgical abortion performed before 16 weeks of pregnancy was shown in 1996 in a meta-analysis of studies to result in a significant reduction in the relative risk of infection (RR 0.58, 95% CI 0.47–0.71)Citation19 and is now standard practice. No such studies exist for medical induction in the second trimester, but most protocols do not involve routine use of antibiotic prophylaxis.
In the D&E case series we reviewed, antibiotic prophylaxis was used in all cases, except in the 1979–80 series.Citation11 In the older case series from the USA and Canada, mild infection was noted in 0.8%Citation9 to 2%Citation10 of cases with follow-up, and 0.05%Citation9 to 0.4%Citation10 required hospitalisation for infection. In the 1979–80 series, 4.1% of women with follow-up were diagnosed with infection.Citation11 In the more recent study of over 2,000 women from the US, two cases of fever not requiring intervention and one case of sepsis leading to coagulopathy and death were reported.Citation12 No cases of infection were reported in the study from Viet Nam.Citation13
In the case series of medical induction with mifepristone–misoprostol, no serious infections were reported, although 2.6% of the 354 women with follow-up data (35% of the total) were given antibiotics at the time of a follow-up visit for presumed pelvic infection.Citation4 The retrospective cohort study found no significant difference in the proportion of women with infection requiring intravenous antibiotics between those who underwent D&E and those who underwent medical abortion; however, the only two cases were in the medical induction group.Citation8
Discussion
Second trimester abortion is associated with higher rates of complications compared to first trimester terminations. Although the risk of complications is relatively higher in the second trimester, the absolute risk is low when the termination is performed (in the case of surgical abortion) and managed (in the case of medical induction) by skilled practitioners. Very little published data exist that directly compare D&E and second trimester medical abortion using mifepristone and misoprostol. The one small randomised controlled trial that suggests D&E is superior to medical induction with mifepristone–misoprostol, both in terms of complications and acceptability, did not have the necessary power to definitively demonstrate a difference in the main outcomes between the procedures. Yet despite the few studies, the data that do exist, reviewed here, show that complication rates with both methods – especially serious complications – are low or rare. It is also notable that D&E appears to have become safer over the years; the frequency of complications is lower in more recent studies compared to older studies.
The complication for which there is a highly significant difference in prevalence between second trimester medical and surgical abortion is incomplete abortion. Although the efficacy of medical abortion regimens continues to improve, 8% of women in the case series from Scotland reviewed here required surgical completion of abortionCitation4 compared to 0.05% in the most recent US case series with D&E who required repeat surgical evacuation.Citation13
Although direct comparisons between the two abortion methods cannot be made for the other individual complications, the findings reviewed here can be used to generate suggestions for future research. The higher proportion of women requiring blood transfusion after medical induction compared to D&E is concerning and deserves further study. This makes intuitive sense, since incomplete abortion, which is so much more commonly associated with medical induction, is associated with haemorrhage. It may be that earlier intervention to perform a surgical evacuation in the case of bleeding with medical induction will result in fewer transfusions, but it would also increase the proportion requiring a surgical evacuation.
The findings related to infection suggest that more research is needed on this outcome after second trimester medical abortion. No conclusions about the comparative risk of infection can be drawn from the data reviewed here because of the small number of women in the medical abortion study who were seen in follow-up and because they did not receive prophylactic antibiotics. The D&E case series in which prophylactic antibiotics were provided had very few cases of infection, particularly severe infection. Future studies of medical induction with mifepristone–misoprostol should ensure adequate follow-up and measure the incidence of clearly defined infection complications in order to determine whether this is an outcome of concern and whether there is any benefit to the use of prophylactic antibiotics.
Uterine rupture can occur with medical induction, and there is much debate about whether women who have had a prior caesarean delivery are at higher risk for this complication. Uterine rupture has been reported in both women who have had prior caesareans and those who have not, and the data are not conclusive about the association between the two. Two retrospective observational studies indicate that there is no increased risk of uterine perforation among women with prior caesarean who undergo medical induction with misoprostol in the second trimester,Citation20Citation21 while another retrospective study of mifepristone–misoprostol suggests that prior caesarean is a significant risk factor.Citation22 Women with a prior caesarean are also at higher risk when they undergo D&E. In the most recent D&E study from the US reviewed here, women with a history of caesarean delivery were three times more likely to experience an adverse event than those with no prior caesarean.Citation12 Women with a history of prior caesarean who undergo second trimester abortion should be considered to be at higher risk regardless of which procedure they undergo; there are no data to suggest that one method is preferable to the other.
This paper does not examine existing data on acceptability of surgical vs medical methods among women or providers. The findings of the randomised controlled trial suggest that, at least in the US, women prefer to undergo D&E. In that study, recruitment was slow because only a minority of eligible women agreed to be randomised, and 93% of those who declined to participate stated they preferred D&E.Citation6 This preference might vary in other settings depending on cultural norms and which procedure is considered standard, but this outcome must be studied further and should inform service delivery. However, any discussion of which method to offer and which is considered to be preferable needs to take into account not only the safety and efficacy of the method but also the experience of the abortion. Proponents of surgical abortion have long argued that D&E is far more efficacious, faster and more compassionate toward women, and spares women having to endure labour and the delivery of a bruised, dead fetus. While the mifepristone–misoprostol regimen has reduced the median induction-to-abortion interval to as low as six hours,Citation23 it is still a difficult experience for women. Where mifepristone is not available and misoprostol must be used alone, the median induction-to-abortion interval is even longer and more unpredictable. In addition, for the woman who experiences an incomplete abortion after medical induction, who must then also have a surgical evacuation, incomplete abortion is surely perceived as an adverse event.
Conversely, D&E is exceedingly predictable with respect to the amount of time required. After the prelude of cervical preparation described above, the actual surgical procedure requires 15 to 20 minutes, even in later gestations. For the woman, such a predictable scenario is often psychologically preferable to the unknowable number of labouring hours intrinsic to induction procedures. Also, because of the additional tranquilising effect of the pain medication used, as well as the more passive involvement of the woman (who is “operated on” but is not an active participant in the actual procedure), D&E may be less emotionally traumatic than induction approaches.Citation24 However, contrary to the lesser involvement of physicians (as opposed to nurses) during induction abortions, D&E requires total physician involvement, and as gestational age increases, much of the emotional burden of the procedure is borne by the physician.
Provision of D&E requires an investment in training of health professionals who can subsequently maintain their skills by performing a minimum number of procedures each year. Research is needed to better understand what that training should include, what level of provider with surgical skills can safely carry out a D&E, and what service volume is needed to maintain skills. Research is also needed to better understand provider preferences regarding methods of second trimester abortion. Most providers today, it seems, at least in Europe, prefer women to have a medical induction than carry out a D&E, and few gynaecologists have sought out training in D&E. A recent review of mid-trimester abortion stated that, although D&E is both safe and effective, “some practitioners feel it very distressing to perform this procedure at an advanced gestation.”Citation3 However, it may also be true that some nurses attending the delivery of a fetus after medical induction in mid-trimester abortion find it equally difficult.Citation24 Studies that examine how clinicians and nurses cope with these difficulties would be useful for education and training purposes. Providing second trimester abortion is challenging for providers whatever the method, yet those willing to be providers are also highly committed to meeting women's needs.
Overall, a larger randomised trial is needed that directly compares second trimester abortion with D&E and with mifepristone–misoprostol, in order to know the extent of differences in complications between the two methods, and at the same time explores in depth acceptability issues for both women and providers. Given the difficulty with recruitment for the randomised controlled trial in the US, there has been scepticism as to whether a comparative study is possible. Ibis Reproductive Health is currently working with the University of Cape Town and other collaborators in South Africa to begin a trial comparing D&E and medical induction, and it may be that the country context there will make the study more feasible. Because medical induction is the standard method of second trimester abortion in South Africa, women may be interested in being able to access D&E services – and potentially avoid medical induction – as part of a study.
Acknowledgements
A version of this paper was presented at the International Conference on Second Trimester Abortion, 29–30 March 2007. The research was funded by the International Planned Parenthood Federation's Safe Abortion Action Fund and the William and Flora Hewlett Foundation.
Notes
* This study also likely included D&E cases performed at less than 15 weeks, but the complication data from all cases 14 weeks and earlier were combined in the report.
References
- LA Bartlett, CJ Berg, HB Shulman. Risk factors for legal induced abortion-related mortality in the United States. Obstetrics and Gynecology. 103(4): 2004; 729–737.
- DA Grimes, KF Schulz, WJ Cates Jr. Prevention of uterine perforation during curettage abortion. Jounal of the American Medical Association. 251(16): 1984; 2108–2111.
- S Lalitkumar, M Bygdeman, K Gemzell-Danielsson. Mid-trimester induced abortion: a review. Human Reproduction Update. 13(1): 2007; 37–52.
- PW Ashok, A Templeton, PT Wagaarachchi. Midtrimester medical termination of pregnancy: a review of 1002 consecutive cases. Contraception. 69(1): 2004; 51–58.
- DA Grimes, JF Hulka, ME McCutchen. Midtrimester abortion by dilatation and evacuation versus intra-amniotic instillation of prostaglandin F2 alpha: a randomized clinical trial. American Journal of Obstetrics and Gynecology. 137: 1980; 785–790.
- DA Grimes, MS Smith, AD Witham. Mifepristone and misoprostol versus dilation and evacuation for midtrimester abortion: a pilot randomised controlled trial. BJOG. 111(2): 2004; 148–153.
- Lohr PA, Hayes JL, Gemzell-Danielsson K. Surgical versus medical methods for second trimester induced abortion. Cochrane Database of Systematic Reviews 2008, Issue 1. Art. No.: CD006714. DOI: 10.1002/14651858.CD006714.pub2.
- AM Autry, EC Hayes, GF Jacobson. A comparison of medical induction and dilation and evacuation for second-trimester abortion. American Journal of Obstetrics and Gynecology. 187(2): 2002; 393–397.
- WF Peterson, FN Berry, MR Grace. Second-trimester abortion by dilatation and evacuation: an analysis of 11,747 cases. Obstetrics and Gynecology. 62(2): 1983; 185–190.
- FR Jacot, C Poulin, AP Bilodeau. A five-year experience with second-trimester induced abortions: no increase in complication rate as compared to the first trimester. American Journal of Obstetrics and Gynecology. 168(2): 1993; 633–637.
- AM Altman, PG Stubblefield, JF Schlam. Midtrimester abortion with Laminaria and vacuum evacuation on a teaching service. Journal of Reproductive Medicine. 30(8): 1985; 601–606.
- A Patel, E Talmont, J Morfesis. Adequacy and safety of buccal misoprostol for cervical preparation prior to termination of second-trimester pregnancy. Contraception. 73(4): 2006; 420–430.
- LD Castleman, KT Oanh, AG Hyman. Introduction of the dilation and evacuation procedure for second-trimester abortion in Viet Nam using manual vacuum aspiration and buccal misoprostol. Contraception. 74(3): 2006; 272–276.
- PD Darney, E Atkinson, K Hirabayashi. Uterine perforation during second-trimester abortion by cervical dilation and instrumental extraction: a review of 15 cases. Obstetrics and Gynecology. 75(3/Part 1): 1990; 441–444.
- PD Darney, RL Sweet. Routine intraoperative ultrasonography for second trimester abortion reduces incidence of uterine perforation. Journal of Ultrasound Medicine. 8(2): 1989; 71–75.
- AG Thomas, M Alvarez, F Friedman Jr. The effect of placenta previa on blood loss in second-trimester pregnancy termination. Obstetrics and Gynecology. 84(1): 1994; 58–60.
- WK Rashbaum, EJ Gates, J Jones. Placenta accreta encountered during dilation and evacuation in the second trimester. Obstetrics and Gynecology. 85(5 Pt 1): 1995; 701–703.
- KF Schulz, DA Grimes, DD Christensen. Vasopressin reduces blood loss from second-trimester dilatation and evacuation abortion. Lancet. 2(8451): 1985; 353–356.
- GF Sawaya, D Grady, K Kerlikowske, DA Grimes. Antibiotics at the time of induced abortion: the case for universal prophylaxis based on a meta-analysis. Obstetrics and Gynecology. 87(5 Pt 2): 1996; 884–890.
- GJ Daskalakis, SA Mesogitis, NE Papantoniou. Misoprostol for second trimester pregnancy termination in women with prior caesarean section. BJOG. 112(1): 2005; 97–99.
- JE Dickinson. Misoprostol for second-trimester pregnancy termination in women with a prior cesarean delivery. Obstetrics and Gynecology. 105(2): 2005; 352–356.
- C Mazouni, M Provensal, G Porcu. Termination of pregnancy in patients with previous cesarean section. Contraception. 73(3): 2006; 244–248.
- H el-Refaey, A Templeton. Induction of abortion in the second trimester by a combination of misoprostol and mifepristone: a randomized comparison between two misoprostol regimens. Human Reproduction. 10(2): 1995; 475–478.
- NB Kaltreider, S Goldsmith, AJ Margolis. The impact of midtrimester abortion techniques on patients and staff. American Journal of Obstetrics and Gynecology. 135(2): 1979; 235–238.