Abstract
To bring the United States in line with prevailing human rights standards, its National HIV/AIDS Strategy will need to explicitly commit to a human rights framework when developing programmes and policies that serve the unaddressed needs of women. This paper focuses on two aspects of the institutionalized mistreatment of people with HIV: 1) the criminalization of their consensual sexual conduct; and 2) the elimination of informed and documented consensual participation in their diagnosis through reliance on mandatory and opt-out testing policies. More than half of US states have HIV-specific laws criminalizing the consensual sexual activity of people with HIV, regardless of whether transmission occurs. Many of these laws hinge prosecution on the failure of HIV-positive people to disclose their HIV status to a sexual partner. The Obama Administration should explore administrative and legislative incentives to eliminate these laws and prosecutions, and target a portion of prevention funding for anti-stigma training. Testing policies should be reconsidered to remove opt-out and/or mandatory HIV testing as a condition for receipt of federal funding; incentives should encourage states to adopt local policies mandating counseling; and voluntary HIV testing should be offered regardless of the provider's undocumented perception of an individual's risk.
Résumé
Pour se mettre en conformité avec les normes des droits de l'homme, les États-Unis devront faire adhérer explicitement leur stratégie nationale de lutte contre le sida à un cadre des droits de l'homme lors de la préparation de programmes et politiques répondant aux besoins des femmes. Cet article porte sur deux aspects de la maltraitance institutionnalisée des personnes avec le VIH: 1) la criminalisation de leur conduite sexuelle consensuelle; et 2) l'élimination de leur participation volontaire éclairée et informée au diagnostic par des politiques de dépistage obligatoire ou à consentement explicite. Aux USA, plus de la moitié des états possèdent des lois spécifiques au VIH qui criminalisent l'activité sexuelle consensuelle des personnes avec le VIH, qu'il y ait ou non transmission du virus. Beaucoup de ces lois fondent les poursuites sur la non-révélation de la séropositivité au partenaire sexuel. Le gouvernement Obama devrait envisager des incitations administratives et législatives pour éliminer ces lois et poursuites, et réserver une partie des fonds de prévention à la formation contre la stigmatisation. Il faut revoir les politiques de dépistage pour ne plus subordonner le financement fédéral au dépistage obligatoire et/ou à consentement présumé; les états doivent être encouragés à adopter des politiques locales obligeant le conseil; et le prestataire proposera le dépistage volontaire du VIH quelle que soit l'idée intuitive qu'il se fait du risque couru par un individu.
Resumen
Para lograr que Estados Unidos siga la línea de las normas imperantes respecto a los derechos humanos, su Estrategia Nacional del SIDA deberá comprometerse explícitamente a un marco conceptual de derechos humanos al crear programas y políticas que atiendan las necesidades insatisfechas de las mujeres. Este artículo se centra en dos aspectos del maltrato institucionalizado de las personas con VIH: 1) la penalización de su conducta sexual consensual; y 2) la eliminación de participación consensual informada y documentada en su diagnóstico mediante la dependencia de políticas referentes a pruebas obligatorias u optativas. Más de la mitad de los estados de EE.UU. tienen leyes específicas al VIH, que penalizan la actividad sexual consensual de las personas con VIH, independientemente de que ocurra transmisión. De acuerdo con muchas de estas leyes, la acusación se basa en el hecho de que las personas VIH-positivas no divulguen su estado de VIH a su pareja sexual. El Gobierno de Obama debería explorar los incentivos administrativos y legislativos para eliminar estas leyes y acusaciones, y designar una porción de los fondos de prevención para la capacitación contra el estigma. Se debe reconsiderar las políticas y eliminar las pruebas optativas y/u obligatorias de VIH como condición para recibir fondos federales; los incentivos deberían motivar a los estados a adoptar políticas locales que exijan consejería; y se deben ofrecer pruebas voluntarias de VIH independientemente de la percepción indocumentada del prestador de servicios en cuanto al riesgo de una persona.
At this writing the United States has no National HIV/AIDS Policy. President Barack Obama has stated that he is committed to developing a National HIV/AIDS Strategy during his presidential term and has tasked the Office of National AIDS Policy with creating a National HIV/AIDS Strategy that reduces stigma, reduces HIV incidence, increases access to care and optimizes health outcomes, and reduces HIV-related health disparities.Footnote*
In April 2009, the Ford Foundation held a Women and HIV Strategic Advocacy Convening for funded organizations working on issues related to human rights, women, and HIV/AIDS. Representatives of these organizations agreed on a series of policy recommendation priorities to guide the new Office of National AIDS Policy (ONAP) and related agencies in their efforts to achieve better outcomes for women affected by HIV.
The recommendations in the resulting publication focus on reducing stigma and discrimination, and improving the recognition of HIV-affected women's human rights. They were developed to inform both the broader health care reform agenda in the United States (US), and the development of a US National HIV/AIDS Strategy.
Through our work in the HIV/AIDS community, as HIV-positive women and their allies, we believe that respecting the human rights of HIV-positive people is key to alleviating stigma and improving HIV/AIDS prevention and care. At direct odds with this principle are the significant number of states that have adopted laws that criminalize HIV exposure, and the recent explosion of cases in which HIV-positive people are being prosecuted and imprisoned for consensual sex, in most cases without having transmitted HIV to their partners. Not only do these policies and practices perpetuate HIV stigma and place the onus of HIV prevention exclusively on one partner, they also dangerously shift attention away from the key to HIV prevention – comprehensive sex education, access to information, frank discussion about ways to sexual health and prevention, and recognition of the responsibility of all adult consensual sexual partners for their own sexual health, demonstrated by safer sex practices, regardless of what is known or believed about any individual partner's status.
The women we work with face numerous structural and societal challenges in their lives that affect the health care and services available to them. We hope that these recommendations open the way to a broader dialogue about improving the lives of women living with and affected by HIV by eliminating all forms of discrimination, and by prioritizing human rights in all policy and legal decisions.
Introduction
International conventions recognize eight basic human rights: civil, political, economic, social, cultural, environmental, developmental, and sexual. All of these rights play a role in the just and humane treatment of people who, as a consequence of their vulnerability to HIV, typically are both marginalized and in need of unique services and accommodation. Laws and policies developed to deal with those affected by HIV/AIDS must incorporate this human rights framework if they intend to address the larger issues that drive and perpetuate the HIV/AIDS epidemic in the United States. Incorporating a human rights framework into national AIDS policy, and specifically the National HIV/AIDS Strategy currently under development, is a critical part of ending the HIV/AIDS epidemic. Addressing government-sanctioned stigma and discrimination that implicitly endorses the isolation and mistreatment of people living with HIV effectively closes doors to their employment, housing, health care and access to other needed services. Fulfilling the government's human rights obligations to its citizens is, therefore, not only a legal obligation but also a public health necessity and long overdue.
To bring the United States in line with prevailing human rights standards, a National HIV/AIDS Strategy will need to make an explicit commitment to a human rights framework for programs, policies, and projects intended to serve the needs of women and others living with HIV and AIDS, starting with their right to access the highest standard of care and to autonomy in decisions related to their diagnosis and treatment. Structural and individual racism and sexism that occurs in the way health care is provided must be addressed, starting with mandated health care provider education and training, in order to bridge the persistent disparities in diagnosis, treatment, and outcomes for minorities of all economic levels and for low-income people. Health care must be provided in an ethical and culturally-appropriate manner that treats patients as partners in their care and recognizes their fundamental right to choose or refuse recommended health care.
In this context, we focus here on two important aspects of the institutionalized mistreatment of people with HIV: the criminalization of their consensual sexual conduct, and the elimination of informed and documented consensual participation in their diagnosis through reliance on mandatory and opt-out testing policies. While there is much work to do before people affected by HIV in this country are treated as equal citizens worthy of the highest standard of ethical medical care, we choose these issues and offer recommendations to address them below because they have been relegated to the margins of most US HIV/AIDS policy advocacy.
Federal, state and local laws and policies that exclude, marginalize and even criminalize people living with HIV/AIDS must be rejected at all levels. In order for our country to meet its basic obligations to its people, it is necessary that people living with HIV/AIDS be treated with dignity, and with the same rights and privileges as all citizens to live and participate in society without irrational restrictions on their ability to maintain their health, livelihoods, and intimate and family relationships.
1. The Obama Administration must take affirmative steps to end the criminalization of people living with HIV/AIDSCitation1Citation2
Background
People with HIV in the United States are subject to discrimination and exclusion to a degree that shocks most Americans. This discrimination includes travel bans on HIV-positive individuals,Citation3 Footnote* rejection from employment due to HIV status,Citation4 denial of child custody or adoption,Citation5 and refusal to license HIV-positive individuals from occupations such as barbering and home health care.Citation4Citation6 Footnote† At the extreme end of this disparate treatment is the criminalization of people with HIV.
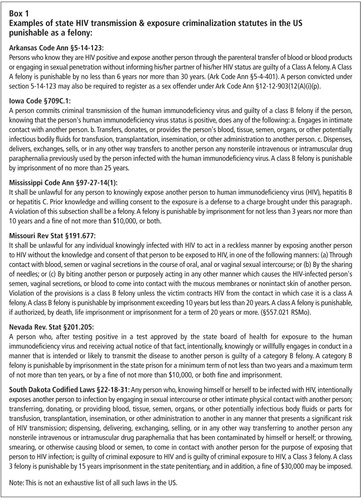
More than half of the states have HIV-specific laws criminalizing sexual contact by people with HIV (see Box 1 for examples of HIV transmission & exposure criminalization statutes punishable as felony offenses with stringent sentences and fines).Citation7 Many of these laws hinge prosecution on the failure of an HIV-positive person to disclose their HIV status to their sexual partners, or be able to prove that they did, punishing only those who have taken the step of getting tested for HIV. Consequently, it is not the risk of transmission, but the fact of an HIV test, that is the central predicate to prosecution.
Recent research has increasingly raised concerns about the negative societal and health consequences related to the rise in criminal prosecutions of people living with HIV. Criminalization laws can lead to further stigmatization of people living with HIV/AIDS and a greater likelihood that people will not be tested for fear of prosecution.Citation1
Criminalization laws ignore the numerous and studied societal reasons that prevent individuals from disclosing their HIV status to sexual partners or others, including fear of domestic violence, fear of familial or partner abandonment, and community rejection. These fears are especially pertinent for women living with HIV/AIDS.
Criminalization of HIV has a particular impact on women. Criminalization heightens stigma and discrimination faced by women when disclosing their HIV status to their partners. Women often find out their status before their partners during routine gynecological or prenatal testing. Because women often know their status first, they can be prosecuted for knowingly transmitting the virus to their partners – even in instances where women may have contracted the virus from their partners but cannot disclose their status due to fear of abuse, violence, or abandonment. Positive women are also vulnerable to prosecution for child neglect when their children contract HIV during pregnancy, childbirth, or while breastfeeding.
Criminalization of HIV transmission further marginalizes groups made vulnerable by the law, including injecting drug users and sex workers, and fails to take into consideration the only proven method of HIV/AIDS prevention: the acceptance of responsibility by both partners to take precautions to prevent HIV/AIDS and STD transmission. HIV transmission does not occur through a failure to disclose but through a failure of sexual partners to take precautions against transmission of HIV and STDs. Prosecutors' sledgehammer approach to the issue of HIV exposure demonstrates not only lingering stigma but also a failure to take into consideration the complexity of human relationships.
Public health officials and policy makers must make visible, concrete, credible investments in protections against HIV-related discrimination and must oppose policies and legislation that would marginalize, isolate and/or punish people with HIV and their communities. Federal incentives are needed to encourage states to approach HIV/AIDS prevention and care as a medical and public health issue and not as a criminal matter. Eliminating the criminalization of HIV/AIDS in the United States will bring our government in line with international consensus and action on this issue as articulated in the Joint United Nations Programme on HIV/AIDS (UNAIDS) Policy Brief on the Criminalization of HIV Transmission.Citation1
Recommended action
The Administration should direct the Centers for Disease Control and Prevention (CDC) to address criminalization laws through the following measures:
Issue a statement or publication that addresses the lack of evidence that criminal prosecutions have had a positive impact on HIV infection, transmission rates, or sexual behavior implicated in HIV transmission;
Have the Surgeon General or appropriate medical official at CDC issue a statement that collects and sets forth facts on HIV transmission, casual contact and HIV, and the impact of antiretroviral therapy on transmission risks posed by people living with HIV.Citation8
Ensure that these official statements can be easily accessed and used by people living with HIV and their advocates in both criminal and civil proceedings (where HIV also has been used to influence custody and other family law proceedings), direct that they be posted prominently on the CDC website, as well as included in the Morbidity and Mortality Weekly Report (MMWR) and/or related publications, and distributed to all state Departments of Health and Attorneys General for state-wide distribution to local health departments, prosecutors, public defenders, and civil and state court judges;
Explore incentive mechanisms, much as the CDC has done in its campaign for adoption of its 2006 HIV testing recommendations, that will encourage states to take corrective action to fix laws criminalizing HIV transmission and exposure. Incentives could include research grants that would monitor changes in testing and risk behavior following repeal of HIV criminal laws or prevention project grants in correctional facilities in states that eliminate barriers to prisoner testing, such as the threat of prosecution for having consensual sex after diagnosis.
Recommended action
The Administration should explore legislative incentives to reduce criminalization laws through supporting law enforcement initiatives that repeal laws criminalizing consensual sexual conduct of people who have tested positive for HIV. Further, the administration should provide clarity that the Ryan White HIV/AIDS Treatment Modernization Act of 2006 does not require the adoption of HIV-specific criminal laws if states can certify (as all can) that their existing criminal laws are adequate to address any need to prosecute acts of intentional transmission of HIV.
Recommended action
The Administration should further address the stigmatizing impact of criminalization by targeting a portion of prevention funding for anti-stigma training of law enforcement officials, court personnel, and prison personnel, as well as other incentive funding to reduce the irrational treatment of people with HIV in the criminal justice system.
2. Federal and state officials should reconsider current policy trends and eliminate coercive HIV testing requirementsCitation9
Background
The health of individuals and the public demand that HIV testing programs be fully informed, consensual, voluntary, confidential or anonymous, and supported, directly or by referrals, with appropriate education, counseling, health care, mental health care, and social services.
The level of understanding of HIV in the general population is still very low, and misperceptions about HIV and AIDS and the transmission of HIV continue to fuel HIV-related stigma and discrimination. For this reason we disagree with the Center for Disease Control's Revised Recommendations for HIV Testing and Counseling that support the de-linking of HIV testing from HIV counseling as a means of lifting barriers to testing.Citation10 Providing all of those offered testing with culturally and linguistically appropriate information about HIV and risk-reduction strategies will help to reduce the misperceptions and related stigma. Testing without counseling about the risk of false negatives can generate a dangerously false sense of security. Newly-infected individuals account for nearly half of all HIV transmission, so programs must counsel those who test negative about the possibility that they could in fact be positive and at their most infectious. Most people are not aware that the greatest risk of transmission is from newly infected individuals with high viral loads who may not know that they are infected and will usually test negative in standard antibody screening.
Protecting human rights through an informed consent testing protocol is consistent with, and not opposed to, the public health goal of expanded HIV testing. The importance of patient knowledge, autonomy, and active participation is central to individuals being empowered to control and demand positive health outcomes. Many current discussions about strategies to expand testing ignore human and civil rights or treat them as barriers to expanded testing and progress in public health policy.Citation5 Citation11 Patients' fundamental rights to health care and informed consent are essential to engaging them in testing, prevention, and trusting relationships with primary providers.
For people to agree to engage in HIV testing and other activities within the health care system, they must feel secure that their rights to privacy and confidentiality will not be violated, that they will have access to health care when needed, that they will be able to disclose their HIV status with relative safety, and that they will be able to work and receive social services without regard to that status.
Promoting high-quality and ethical service provision is as important in HIV testing as it is in the medical management of HIV therapies and the conduct of clinical trials. The Centers for Disease Control and Prevention maintains in its 2006 Revised Recommendations for HIV Testing of Adults, Adolescents, and Pregnant Women in Health-Care Settings that testing must be with the knowledge of the patient, voluntary, and free from coercion,Citation11 and states that the Recommendations
“…are intended to comply fully with the ethical principles of informed consent…” Citation11
The CDC Recommendations must be revised to ensure that all of its provisions are consistent with these basic principles and mandates.
Recommended action
Remove opt-out and/or mandatory HIV testing as a condition for receipt of federal Ryan White Act/CDC funding and discourage calls and incentives for mandatory newborn testing without parental consent. HIV testing programs must be tailored to different clinical settings, populations, and patient needs, such as those in dependent or abusive relationships, recent immigrants, and young women without strong systems of social support.
Recommended action
Create incentives to encourage states to adopt local policies that mandate counseling and offering of voluntary HIV testing regardless of perceived risk. Mandatory counseling and offering of voluntary testing should be included in primary care services, including routine gynecological and sexual and reproductive health services, and other key points of entry for ongoing primary care.
These mandates will require public and private insurance plans to cover both counseling and testing as reimbursable services. Reimbursement is rarely an issue when testing is based on counseling and a conversation with the provider that confirms that the individual to be tested has engaged in behavior that can expose them to HIV.
Recommended action
Increase funding for model programs that streamline the HIV testing process while documenting informed consent, increased voluntary testing, and corresponding increased entry into care.
Recommended action
Everyone offered testing must be educated about HIV and the significance of positive and negative test results.
Conclusion
When HIV/AIDS policies, whether national or local, do not address the human rights of women affected by HIV/AIDS, they risk not only furthering the stigma and systemic discrimination faced by women but also exacerbate the epidemic itself. With many of our towns, cities and states facing an epidemic that is hitting women, and especially women of color, hard we cannot risk undermining the rights of women, nor can we implement policies that will further alienate already disenfranchised groups.
It is imperative to use a human rights framework in the development of health care reform and a National HIV/AIDS Strategy in order to bring about a successful HIV/AIDS treatment and prevention plan for our nation. Such a framework takes into account, and seeks to alleviate, the intersecting issues surrounding HIV/AIDS treatment and prevention that perpetuate health disparities.
We hope to enter a new era of respect for and compliance with national and international civil and human rights laws with the Obama Administration. The above principles and recommendations can serve as a guide in this period of great change. Taking women's rights and dignity into account throughout our legislative and executive law-making processes will prove beneficial not only for women and their families but for the nation as a whole.
Acknowledgments
Terry McGovern, Ford Foundation HIV/Human Rights Program Officer, held the Women, Human Rights & HIV/AIDS convening in New York, NY, April 2009, where the resulting publication was initially conceived. This article is an edited and expanded excerpt from a larger document entitled Critical Issues for Women and HIV: Health Policy and the Development of a National AIDS Strategy, July 2009, that covers topics of meaningful involvement, discrimination and human rights violations, disparities in southern and rural United States, health care reform and access, the integration of reproductive health and HIV/AIDS care, and prevention for women living with and affected by HIV/AIDS. The organizations that contributed to the original document were the African Friends Services Committee, New York, NY; AIDS Alabama, Birmingham, AL; Alliance of AIDS Services, Raleigh, NC; Center for HIV Law & Policy, New York, NY; Community HIV/AIDS Mobilization Project, New York, NY; Center for Health and Gender Equity, Washington, DC; HIV Law Project, New York, NY; International Community of Women Living with HIV, Washington, DC; National AIDS Fund, Washington, DC; National Women and AIDS Collective, a project of the Ms. Foundation, New York, NY; Sisterlove, Inc, Atlanta, GA; US Positive Women's Network, Oakland, CA; The Women's Collective, Washington, DC; Women Organized to Respond to Life-threatening Disease, Oakland, CA.
Notes
* See <www.whitehouse.gov/administration/eop/onap/>; <www.whitehouse.gov/the_press_office/President-Obama-Selects-Health-Policy-Expert-to-Head-Office-of-National-AIDS-Polic/> and <www.windycitymediagroup.com/gay/lesbian/news/ARTICLE.php?AID=21327>.
* Stop press: The 22-year-old travel ban was lifted by President Obama as of 2 November 2009 because it was “rooted in fear rather than fact”. From: Washington Post, 30 October 2009.
† The US Department of Justice released guidelines in July 2009, clarifying the rights of persons with HIV/AIDS to obtain occupational training and state licensing.
Related Research Data
References
- UNAIDS. Criminalization of Transmission. UNAIDS Policy Brief. At: <http://data.unaids.org/pub/BaseDocument/2008/20080731_jc1513_policy_criminalization_en.pdf. >. Accessed 11 August 2009.
- Center for HIV Law and Policy. HIV/AIDS Criminalization Resource Bank. At: <http://www.hivlawandpolicy.org/resourceCategories/view/2. >. Accessed 11 August 2009.
- UNAIDS/International Organization for Migration. Statement on HIV/AIDS-related travel restrictions. June 2004. At: <www.iom.int/jahia/webdav/site/myjahiasite/shared/shared/mainsite/activities/health/UNAIDS_IOM_statement_travel_restrictions.pdf. >. Accessed 11 August 2009.
- Center for HIV Law & Policy. State Guidelines for HIV-Positive Health Care Workers. At: <www.hivlawandpolicy.org/resourceCategories/view/5. >. Accessed 11 August 2009.
- American Civil Liberties Union AIDS Project. HIV & Civil Rights: A Report from the Frontlines of the HIV/AIDS Epidemic. At: <www.aclu.org/pdfs/hivaids/hiv_civilrights.pdf. >. Accessed 11 August 2009.
- US Department of Justice. The Americans with Disabilities Act and the Rights of Persons with HIV/AIDS to Obtain Occupational Training and State Licensing. At: <www.ada.gov/qahivaids_license.htm. >. Accessed 11 August 2009.
- ACLU Lesbian & Gay Rights Project, AIDS Project. State criminal statutes on HIV transmission, 2008. At: <www.aclu.org/images/asset_upload_file292_35655.pdf. >. Accessed 11 August 2009.
- Center for HIV Law and Policy. Sample expert statement on HIV transmission risk. At: <www.hivlawandpolicy.org/resources/view/381. >. Accessed 11 August 2009.
- ACLU AIDS Project & Lambda Legal. Increasing access to voluntary HIV testing: the importance of informed consent and counseling in HIV testing. At: <www.aclu.org/images/asset_upload_file473_30248.pdf. >. Accessed 11 August 2009.
- Centers for Disease Control and Prevention. CDC Revised Recommendations for HIV Testing of Adults, Adolescents, and Pregnant Women in Health-Care Settings 2006: 7-8, 13. At: <www.cdc.gov/mmwr/preview/mmwrhtml/rr5514a1.htm. >. Accessed 11 August 2009.
- National HIV/AIDS Clinicians' Consultation Center, San Francisco General Hospital University of California, San Francisco. Compendium of State HIV Testing Laws. 2009. At: <www.nccc.ucsf.edu/StateLaws/Index.html>. Accessed 11 August 2009.