Abstract
In the Netherlands, most abortions of early pregnancies have been with electric vacuum aspiration (VA). A study was conducted on women’s motivations for choosing surgical (VA) or medical abortion and extent of satisfaction with the method chosen. Information was also collected about the proportion of medical abortions to total abortions in the Netherlands and, for comparison, in some other European countries. Of 501 women with early abortions surveyed in 2008/09, 71% opted for VA. Except for “previous experience”, women had different motivations for preferring one or other method. At the post-abortion check-up, satisfaction with the medical method was lower compared to VA. Nevertheless, 80% of those who chose medical abortion would do so again. Nineteen out of 20 doctors questioned at a meeting on abortion offered surgical and medical abortion. Seven of the 11 who gave an opinion found medical abortion an excellent alternative and four thought having the choice was important. The proportion of medical abortions per clinic ranged from <1% to 33%. The proportion of medical vs. surgical abortions in all the countries looked at is influenced by provider attitudes and service-related factors. The use of medical abortion in the Netherlands might increase over time but is unlikely to rise as high as in some other European countries.
Résumé
Aux Pays-Bas, la plupart des avortements en début de grossesse sont pratiqués par aspiration électrique par le vide. Une enquête a étudié les motivations des femmes ayant opté pour cette technique ou pour l’avortement médicamenteux, et leur degré de satisfaction avec la méthode choisie. Elle a aussi estimé la proportion d’avortements médicamenteux sur l’ensemble des avortements aux Pays-Bas et, par comparaison, dans certains pays européens. Sur les 501 femmes ayant avorté en début de grossesse qui ont répondu à l’enquête en 2008/09, 71% avaient opté pour l’aspiration électrique. À l’exception d’une « expérience précédente », les femmes avaient différentes motivations pour préférer l’une ou l’autre méthode. Au cours du contrôle post-avortement, la satisfaction était plus faible avec la méthode médicamenteuse qu’avec l’aspiration. Néanmoins, 80% des femmes ayant choisi l’avortement médicamenteux le referaient. Sur 20 médecins interrogés pendant une réunion sur l’avortement, 19 proposaient l’aspiration électrique et l’avortement médicamenteux. Sept des 11 qui ont donné leur avis trouvaient que l’avortement médicamenteux était une excellente alternative et quatre pensaient qu’il était important d’avoir le choix. Le pourcentage d’avortements médicamenteux par centre allait de <1% à 33%. La proportion d’avortements médicamenteux par rapport aux avortements chirurgicaux dans tous les pays examinés est influencée par les attitudes des soignants et des facteurs liés aux services. Le recours à l’avortement médicamenteux aux Pays-Bas pourrait s’accroître au fil du temps, mais il est peu probable qu’il atteigne le niveau de certains autres pays européens.
Resumen
En los Países Bajos, la mayoría de los abortos de embarazos tempranos se han efectuado con aspiración eléctrica endouterina (AEEU). Se realizó un estudio sobre las motivaciones de las mujeres para escoger AEEU o aborto con medicamentos y la satisfacción con el método elegido. Además, se recopiló información sobre la proporción de abortos con medicamentos al número total de abortos en los Países Bajos y, para comparación, en algunos países europeos. De 501 mujeres que tuvieron abortos tempranos y fueron encuestadas en 2008/09, el 71% optó por AEEU. Excepto por “experiencias anteriores”, las mujeres relataron diferentes motivaciones para haber preferido un método u otro. En el chequeo postaborto, la satisfacción con el método médico fue más baja comparada con la AEEU. Sin embargo, el 80% de las mujeres que escogieron aborto con medicamentos lo harían de nuevo. De los 20 médicos cuestionados en una reunión sobre aborto, 19 ofrecían aspiración por vacío y aborto con medicamentos. Siete de los 11 que dieron una opinión consideran que el aborto con medicamentos es una alternativa excelente y cuatro piensan que es importante tener la opción de escoger. La proporción de abortos con medicamentos por clínica varió de <1% al 33%. La proporción de abortos médicos con respecto a quirúrgicos en todos los países estudiados es influida por las actitudes de los prestadores de servicios y por factores relacionados con los servicios. Es posible que el uso de medicamentos para inducir el aborto en los Países Bajos aumente con el tiempo, pero es improbable que aumente tanto en algunos otros países europeos.
Medical abortion with mifepristone combined with a prostaglandin has been available in France since 1988 and is an alternative to surgical abortion. International research on the differences between medical and surgical procedures has demonstrated advantages and disadvantages of both methods. In the Netherlands, the proportion of women choosing medical abortion is much lower than in other countries where this method is available. Moreover, little is known about the motives and satisfaction of the women opting for one or other method in the Netherlands. What could be the reasons for this difference?
Only Dutch outpatient clinics and hospitals with special permission can provide abortions, either medical or surgical, with local or general anaesthesia. Ninety-four per cent of all abortions are performed in outpatient clinics.Citation1 Women who choose surgical abortion in the clinics have this procedure often under local anaesthesia (in 2008, 44.4% of all procedures were done with local anaesthesia, 32.9% under general anaesthesia, 9.7% with conscious sedation, 10.4% without any form of anaesthesia).Citation2 Women are advised to go to their general practitioner (GP) or the doctor who referred them to the clinic for a check-up three weeks after the abortion, or they can have their check-up at the clinic where the abortion was performed. Most often, women find it more convenient to go to their GP. When leaving the clinic, each patient is supplied with an evaluation form with questions about their physical and psychological condition after the abortion. They are asked to return this form by mail or in person at the check-up.
In the outpatient clinics, experience with surgical aspiration of very early pregnancies is widespread. In 2000, 48% of all abortions were performed before seven weeks LMP, almost exclusively by electrical vacuum aspiration.Citation3 In 2006, around 56% of all abortions were at less than seven weeks and 21.8% of these early abortions were medical abortions with mifepristone and misoprostol.Citation4 The high percentage of early abortions in these clinics indicates few patient and doctor delays in seeking or providing abortion services. In the Netherlands, most clinics limit early medical abortion to seven weeks LMP, although medical abortion has been approved by the European Medicines Agency (EMA) till nine weeks LMP. This limit in duration of pregnancy for medical abortion is discussed below. Medical abortion up to nine weeks was being provided in two clinics. These two clinics changed their policy after medical abortion through nine weeks LMP was allowed in Germany in 2008.
Since medical abortion became available in the Netherlands in 2000,Citation5 its use has increased. There are, however, large differences between the 17 clinics in terms of which procedures are used. Both surgical and medical methods are available because some studies emphasise that women prefer to have a choice,Citation6 and that women may prefer one method over the other based on clinical grounds or on their beliefs or experience with previous abortions.Citation7Citation8 The literature shows a high percentage of satisfaction with both methods, especially if circumstances make a personal, unrestricted choice possible. However, satisfaction with the surgical method in some studies has been somewhat higher, especially in those studies where the choice of method was left to the provider.Citation9
After general counselling, in most of the clinics, all women with an early pregnancy are offered the choice between a medical or a surgical abortion. The characteristics of each method are explained and written information about the methods and the differences between them are distributed, so that women can make an informed choice about which they prefer.
The surgical abortion is done in a friendly setting: often the patients are accompanied by their partner, friend or mother during the procedure. The nurse and the doctor will reassure the woman and talk her through what will happen. In early pregnancies dilation of the cervix is usually not necessary, vacuum curettes of 4 or 5 mm are used. The whole procedure including ultrasound, disinfection and aspiration will take 10–15 minutes, of which five minutes can be painful. Pain medication is often given before the procedure and in the majority of clinics conscious sedation is available if necessary.
The medical abortion method used in Dutch clinics consists of 200 mg mifepristone orally,Citation10Citation11 followed by 800μg misoprostol 24–72 hours after the administration of mifepristone. Misoprostol is used vaginally, but if women have difficulties with this route of administration they can use it sublingually. Pain medication, such as NSAIDs, is discussed during the intake and is prescribed according to the preferences of the woman. Home use of misoprostol differs per clinic; with most clinics, the woman usually takes the misoprostol at home. Three weeks after the pills are taken, a routine check-up in the clinic is strongly encouraged to exclude possible failures.
There has been only one publication about medical abortion from the Netherlands, comparing this method with the surgical method at the time of the introduction of early medical abortion for social reasons.Citation5 It is therefore interesting to know what patients’ experience with this method has been, now that it has been established for a couple of years. Moreover, medical abortion is used far more in France, Sweden, Switzerland and the UK and it would be useful to know the reasons for this, which are unclear.
Methods and materials
In the Mildredhuis, an outpatient abortion clinic in the Netherlands, almost 2,000 abortions take place each year. For this study, consecutive files of 501 women who had an abortion between July 2008 and the end of January 2009 with a duration of pregnancy less than 50 days LMP were selected for analysis. The following information was collected from these records: age of the patient, duration of the pregnancy, number of previous abortions, number of children, motivation for the choice of the method, and at check-up, personal experience with the method chosen and preferred method if the woman needed an abortion in future. Any remarks pertaining to satisfaction with the method used and problems experienced during the abortion were also noted. Feedback on satisfaction was based on the available data. More than half the women with a surgical abortion did not return for a check-up, either to the clinic or their GP. Characteristics of this group were studied separately. Data were analysed using SPSS. The Medical Ethical Committee of the University of Utrecht approved the protocol.
For the comparison of the use of medical abortion in other countries, national data from France, Sweden, England and Wales, Switzerland, Scotland (and the Netherlands) were taken into consideration. In some of these countries medical abortion is provided up to 63 days LMP (nine weeks). In the other countries, at the time of data collection (2008–2009) the provision of medical abortion was limited to 49 days LMP. The data were available for medical abortion as a percentage of all abortions. In Switzerland, France and the Netherlands no national data were available on the percentage of medical abortions of early pregnancies, and in these cases an estimate was asked of experts in the countries concerned. Off-label use of medical abortion beyond nine weeks of pregnancy is carried out in most of these countries and also in the Netherlands, but in this article I have restricted the collection of data to early medical abortion.
In the Netherlands, there are about 50 abortion doctors. They have a meeting twice a year, attended by the most involved providers. Twenty participants in one of these meetings answered a small questionnaire and discussed their attitudes towards medical abortion. Questions included whether they prescribed medical abortion, until what date LMP of pregnancy, which method they would choose if they themselves or their partner needed an abortion, and what they generally thought of the medical method.
Results
Between July 2008 and the end of January 2009, 1,095 women requested an abortion at the Mildredhuis clinic. Of this number, 501 (46%) women had pregnancies of less than seven weeks LMP, of whom 145 (29%) opted for medical abortion and 356 (71%) opted for surgical abortion. Four of the 145 women choosing medical abortion wanted to have the second part of the treatment, the misoprostol, in the clinic, while 141 women chose to take the misoprostol at home.
Table 1 lists the characteristics of the women by abortion method. Women having surgical abortion were only slightly older on average and had slightly more children. The women using both methods were pregnant for less than six weeks on average and those having surgical abortion were pregnant for just over three days more than those using medical abortion pills.
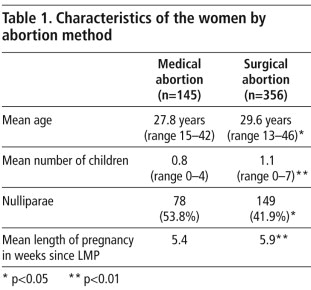
Table 2 shows the reasons why women chose one or other method and the proportion who did so for each of the reasons listed. For the medical abortion users, the main reasons given were fear of aspiration, and the perception that medical abortion was more natural and more like a miscarriage. Some said specifically that they would terminate the pregnancy only if the medical method was available. Women choosing a surgical abortion expected the procedure to be faster and easier, they liked the idea that it would be over before they went home, and some wanted an IUD inserted at that stage as well. In both groups, women with previous abortions let their experience influence their present choice.
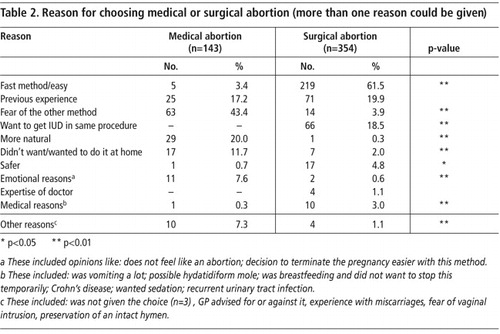
Most clinical reasons were mentioned by the woman as important for their decision, not by the provider. In five instances, the abortion could take place sooner medically and medical abortion was chosen for that reason; for instance, in two cases the clinic would be closed due to the holiday season or the women themselves were unavailable for an early surgical appointment. Except for previous experience of the method, motivations for choosing medical abortion were different from those for choosing surgical abortion.
Problems completing the abortion with the first method used
Two early pregnancies were difficult to reach with the curette, one because of a distortion of the cervical canal and one because of a uterus duplex. Neither termination was completed by aspiration; one was terminated medically, the other woman was referred to a hospital for termination, both with success.
The surgical group had four (1.1%) cases where the uterus was not completely empty at check-up and needed a second aspiration; two of these women had a very small fetal sac of less than 8 mm at presentation. In the medical group, six (4%) patients still had a fetal sac in utero at check-up and had a subsequent aspiration.
Satisfaction with the method used at time of post-abortion check-up
In the medical abortion group, 35 women (24%) did not return for check-up (of these, 13 had had a previous medical abortion); 110 (76%) returned for check-up. In the surgical abortion group (n=356), 76 women (21%) returned for check-up. We collected information about the level of satisfaction with the methods from all available sources (evaluation forms and letters from the GP or gynaecologist); more data were available for some questions in the surgical group (Table 3 ).
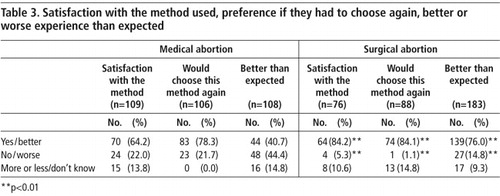
Overall, women’s satisfaction with the method used, whether they would choose the same method again and whether the experience was better than expected were in all cases significantly more positive for the surgical abortion group than the medical abortion group.
The experience with medical abortion was considered better than expected by 44 of 108 women for whom data were available, because they found it less scary than an aspiration or the whole experience was less painful than they had expected. It was worse than expected for 48 of the 108 women because of severe pain and/or blood loss. The heavy blood loss lasted in three cases for three weeks. Heavy blood loss together with severe pain was mentioned 16 times, heavy blood loss without pain was mentioned nine times, 19 women mentioned more than expected pain. Some women had other side effects of the medication, like diarrhoea or nausea; these are expected side effects of misoprostol. For four of the 48 women the experience was worse than expected because the abortion was not complete and they needed an aspiration after all. Although the experience was often worse than expected, 64.2% of the women were satisfied with medical abortion. Their reasons for choosing it tipped the balance toward a positive opinion.
“It was an overwhelming experience and I had more blood loss than I expected but it was nice to be at home.”
“First I had an awful lot of pain, but this disappeared when I sat in a hot bath.”
Of the 64 nulliparae for whom data were available, 36 said at check-up that the medical abortion was worse than they had expected for the same reasons as stated above; however, most (45 of the 64) said they would choose this method again.
Nulliparae often had a worse experience with medical abortion than multiparae. The tables used for the comparison are not shown. Looking back on the experience, 44.4% of the women (56.6% of the nulliparae versus 27.3 % of the multiparae) with a medical abortion found this experience worse than expected. The experience was worse than expected for only 14.8% (21.8% of the nulliparae versus 9.5% of the multiparae) of the women who had a surgical abortion. These differences have also been shown in other studies.Citation9,19,20
Information about the women who did not come for check-up
For insight about the experience of women for whom no information was available post-abortion, we compared them with the group for which information was available, to see if there were differences. Significantly more women who had a medical abortion returned for check-up. There was no difference in motivation for the abortion between those who returned and those who did not. However, more women having had a previous abortion or who were younger did not return for check-up in the surgical abortion group. Since the clinic as well as the GP were within easy reach for these patients, this cannot be the reason for not returning. However, most women want to leave this experience behind them as soon as possible, and many return only when there is a perceived problem. In the medical abortion group, having had an previous abortion or being younger did not reach a significant level.
Medical abortion in the other European countries
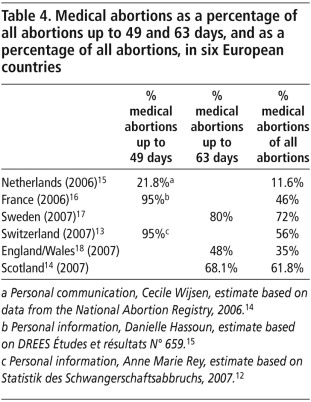
In the other European countries studied (Table 4 ), the method of preference in early pregnancy seems to be medical abortion.Citation13–18 In the Netherlands, medical abortion is used much less frequently than in Great Britain, Sweden, Switzerland and France.Citation21Citation23
Table 4 Citation12
Information from and views of 20 abortion providers in the Netherlands
Of the 20 abortion providers (40% of all providers, 66% of the most active) at the providers meeting, 19 prescribed medical abortion,15 up to 49 days LMP, two up to 63 days, and one up to 56 days. One did not prescribe medical abortion, because she thought the method inferior to surgical abortion. The limit of 49 days was adhered to, because these clinicians still follow the French protocol and also because they found (especially close to 63 days LMP) blood loss to be heavier, the effectiveness somewhat lower and the women told them that the viewing of fetal material close to 63 days was unpleasant with home use of medical abortion.
Their personal preference, if they themselves or their partner had to choose a method, would be as follows: 11 would (probably) choose surgical abortion, mainly because it was a fast method and very reliable. Six would choose medical abortion, since it has almost no contraindications. Three did not know which method they would choose. Of the group that would opt for surgical abortion, five would choose medical abortion in special circumstances. For instance if the pregnancy was less than six weeks, if they were very afraid of the surgical method, or if there were medical contraindications for surgical abortion. Eleven of the 20 participants stated an opinion about medical abortion: seven found it an excellent alternative and four thought it very important that women had a choice.
“It is a good alternative, although less so for women who are very much afraid of pain, because no sedation can be given.”Footnote*
“I think medical abortion is just as effective and safe as surgical abortion below 8 weeks LMP.”
“It is good there are alternative methods, it proves the success of surgical abortion.”
“I like medical abortion as a method but there is more insecurity, more questions and more complaints than with surgical abortion.”
Discussion and conclusions
In this study I did not focus specifically on effectiveness or side effects of the two abortion methods as such but more on the reported opinions of the women involved. I conclude that the motivation for choosing a surgical procedure is different from that for a medical procedure.
Two embryos following early abortion. The one on the left was aspirated from a pregnancy of 4–5 weeks LMP (6 mm). The one on the right is from a pregnancy of about 6 weeks LMP following medical abortion (18 mm).
Since the experience with former abortions is often a reason to choose a specific method again, it might well be that the proportion of medical abortions will increase as experience among women with this method increases. Although almost 30% of the women in this study had had one or more abortions previously, and this experience influenced their present preference, statistically little can be said about their former abortion, however, because the numbers were very small.
Of the women who had a medical abortion for whom the experience was worse than expected, a considerable number would, nevertheless, choose the same method again, usually because they remained afraid of the surgical method or because the positive aspects outweighed the negative ones. However, more women in the surgical than in the medical group would choose the same method of abortion again. This difference has also been shown in other studies.Citation9,19–21
Compared to four other countries in Western Europe, the use of medical abortion is low in the Netherlands. In hospitals and clinics in the other countries looked at, the more extensive use of medical abortion seems partly provider- and clinic-driven.Citation7,21 Possible provider-linked arguments are the lack of trained providers with experience with the surgical procedure with very early pregnancies or resistance to aspiration before seven weeks, and the personal preferences of the individual providers for a specific method. Possible clinic-related arguments are that surgical procedures have to be done in a hospital operating room, need general anaesthesia, a waiting period may be required, and sometimes cost can influence the choice.Citation21–23 In these countries, the arrival of medical abortion and the possibility it offers for less hospitalised care has been enthusiastically taken up. These responses have not taken place in the Netherlands. Cost, for example, is not an issue because in the Netherlands both methods are free of cost for Dutch inhabitants and the waiting period is short and identical for both methods.
Surgical abortion is the preferred choice for a large majority of women seeking abortion in clinics in the Netherlands. The proportion of women choosing medical abortion might increase in the Netherlands in the near future, but it will most likely not reach the same proportion as in some other European countries. This study shows that there is undoubtedly a place for medical abortion in the Netherlands and room for more use of the method in the clinics where it is currently hardly ever provided. At the same time, in other European countries, the proportion of medical abortions might decrease if the possibility of earlier surgical aspiration were as easily accessible as in the Netherlands.
Acknowledgements
I wish to thank Evert Ketting and Marcel Vekemans for their critical reading of this manuscript and valuable advice.
Notes
* Although sedation is inappropriate for medical abortion, pain relief can be provided. Ibuprofen is usually sufficient with early abortion.
References
- Inspectie voor de Gezondheidszorg. Jaarrapportage 2007 van de Wet afbreking zwangerschap. (Annual Report 2007 of the Law on Termination of Pregnancy) Den Haag: IGZ, 2008. p.19.
- H Kruijer, L van Lee, C Wijsen. Landelijke abortusregistratie 2008. 2009; Rutgers Nisso Groep: Utrecht, 17.
- C Wijsen, J Rademakers. Abortus in Nederland 2001–2002. (Abortion in the Netherlands 2001–2002). 2003; RutgersNissogroep: Utrecht, 19.
- Inspectie voor de Gezondheidszorg. Jaarrapportage 2006 van de Wet afbreking zwangerschap. (Annual Report 2006 of the Law on Termination of Pregnancy) Den Haag: IGZ, 2007. p.17.
- J Rademakers, E Koster, A Jansen-van Hees. Medical abortion as an alternative for vacuum aspiration: first experiences with the “abortion pill” in the Netherlands. European Journal of Contraception and Reproductive Health Care. 6: 2000; 185–191.
- A Hemmerling, F Siedentopf, H Kentenich. Emotional impact and acceptability of medical abortion with mifepristone: a German experience. Journal of Psychosomatic Obstetrics & Gynaecology. 26: 2005; 23–31.
- PC Ho. Women’s perceptions on medical abortion. Contraception. 74: 2006; 111–115.
- RC Henshaw, SA Naji, IT Russell. Comparison of medical abortion with surgical vacuum aspiration: women's preferences and acceptability of treatment. British Medical Journal. 307: 1993; 714–717.
- C Rørbye, M Nørgaard, L Nilas. Medical versus surgical abortion: comparing satisfaction and potential confounders in a partly randomized study. Human Reproduction. 20: 2005; 834–838.
- M Berer. Medical abortion: a fact sheet. Reproductive Health Matters. 13: 2005; 20–24.
- SR Trupin, C Moreno. Medical abortion: overview and management. Medscape General Medicine. 4(1): 2002. At: <www.medscape.com/viewarticle/429755. >. Accessed 4 March 2009.
- MD Creinin. Medical abortion for early pregnancy. Current Problems in Obstetrics, Gynaecology and Fertility. 20: 1997; 19–32.
- Bundesamt für Statistik BFS, Switzerland. Statistik des Schwangerschaftsabbruchs, 2007. Anzahl Schwangerschaftsabbrüche stabil und relativ tief. (Statistics of termination of pregnancy 2007. Number of terminations of pregnancy stable and relatively low). At: <www.svss-uspda.ch/pdf/SA-2007-bfs.pdf>. Accessed 22 April 2009.
- Shanks E, Chalmers J, Philip A. Abortion Statistics, Scotland, year ending December 2007. Edinburgh: ISD Scotland Statistical Publication Notice 2008. At: <www.isdscotland.org/isd/5644.html>. Accessed 28 March 2009.
- L van Lee, C Wijsen. Landelijke Abortus Registratie 2006 [National Abortion Registry 2006]. 2006; RutgersNissogroep: Utrecht.
- Vilain A. Les interruptions volontaires de grossesse en 2006. (Voluntary terminations of pregnancy in 2006, France) DREES Études et résultats N° 659, Paris, 2008. At: <www.sante.gouv.fr/drees/etude-resultat/er-pdf/er659.pdf>. Accessed 3 April 2009.
- B Ollars, A Lindam. Induced abortions 2007. Official Statistics of Sweden. Health and Diseases. 4: 2008
- Government Statistical Service. Abortion Statistics, England and Wales: 2007. Statistical Bulletin. 1: 2008. At: <www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsStatistics/DH_085508. >. Accessed 3 April 2009.
- A Bachelot, L Cludy, A Spira. Conditions for choosing between drug-induced and surgical abortions. Contraception. 45: 1992; 47–59.
- Winikoff B. Acceptability of medical abortion in early pregnancy. Family Planning Perspectives 1995;27:142–48 &158.
- G Pheterson. Avortement pharmacologique ou chirurgical: les critères sociaux du “choix” (Medical versus surgical abortion: social determinants of “choice”). Cahiers du Genre. 31: 2001; 221–247.
- RK Jones, MRS Zolna, SK Henshaw. Abortion in the United States: incidence and access to services, 2005. Perspectives on Sexual and Reproductive Health. 40: 2008; 13–15.
- RK Jones, SK Henshaw. Mifepristone for early medical abortion: experiences in France, Great Britain and Sweden. Perspectives on Sexual and Reproductive Health. 34: 2002; 154–161.