Abstract
Abstract
There are important and compelling reasons why women have second trimester abortions, which constitute a significant percentage of all abortions performed. Laws vary widely around the world on the legality of these abortions. In many cases, they are quite restrictive. Indeed, the later in pregnancy an abortion is sought, the more restrictive the law tends to be. However, many laws say little about second trimester or later abortions. This article reviews the laws of the 191 countries around the world for which information is available and categorizes them by legal indications, which include preservation of the woman's life, health reasons, pregnancy due to sex offences, fetal impairment, socio-economic reasons and on request. Given that there are serious reasons why women have second trimester abortions, and that the laws in many countries do not make these abortions legally available, this paper makes recommendations on how laws and regulations can be changed in order better to respond to women's needs. While most countries may not decriminalise all abortions in the near future, especially second trimester abortions, less comprehensive legislative and regulatory reforms are possible. These include recommendations aimed at ensuring that abortions are carried out safely and as early as possible in pregnancy, and improving access to safe abortions by removing unnecessary legal and regulatory restrictions.
Résumé
Des raisons importantes et pressantes incitent les femmes à avorter au deuxième trimestre. Ces avortements représentent un pourcentage non négligeable de l'ensemble des avortements pratiqués. Les lois sur la légalité de ces avortements varient largement dans le monde et sont souvent assez restrictives. En fait, plus un avortement est demandé à un stade avancé et plus les lois tendent à être restrictives. Néanmoins, beaucoup de lois parlent peu des avortements du deuxième trimestre ou plus tard. Cet article examine les lois des 191 pays du monde pour lesquels on dispose d'informations et les classe par indications juridiques : protection de la vie de la femme, raisons sanitaires, grossesse consécutive à un délit sexuel, anomalie fłtale, motifs socio-économiques et avortement à la demande. Étant donné que les femmes ont des motifs graves pour avorter au deuxième trimestre et que les lois dans beaucoup de pays n'autorisent pas ces avortements, l'article recommande des modifications pouvant être apportées aux lois et aux réglementations afin de mieux répondre aux besoins des femmes. Si la plupart des pays ne dépénaliseront probablement pas tous les avortements à brève échéance, particulièrement les avortements du deuxième trimestre, des réformes législatives et régulatrices moins vastes sont possibles. Elles incluent des recommandations pour garantir des avortements pratiqués en toute sécurité et le plus tôt possible dans la grossesse, et pour améliorer l'accès à l'avortement sans risque en levant les restrictions légales inutiles.
Resumen
Existen importantes y convincentes razones por las cuales las mujeres tienen abortos en el segundo trimestre, los cuales constituyen un porcentaje significativo de todos los abortos realizados. Las leyes de aborto varían extensamente en todo el mundo. En muchos casos, son muy restrictivas. Mientras más avanzado el embarazo en el momento en que se buscan los servicios de aborto, más restrictiva tiende a ser la ley. Sin embargo, muchas leyes dictan poco en cuanto a abortos en el segundo trimestre o después. En este artículo se analizan las leyes de 191 países sobre las cuales se dispone de información y se categorizan por indicaciones legales, como la conservación de la vida de la mujer, razones de salud, embarazo producto de delitos sexuales, discapacidad fetal, razones socioeconómicas y a petición. Dado que existen importantes razones por las cuales las mujeres tienen abortos en el segundo trimestre y que, en muchos países, las leyes no permiten estos abortos, en este artículo se hacen recomendaciones sobre cómo cambiar las leyes y los reglamentos para poder responder mejor a las necesidades de las mujeres. Aunque quizás no se logre la despenalización del aborto en todos los países en un futuro cercano, especialmente del aborto en el segundo trimestre, es posible lograr reformas legislativas y reguladoras menos integrales, por ejemplo: recomendaciones dirigidas a garantizar que todos los abortos se efectúen de manera segura y lo más temprano posible en el embarazo, y a mejorar el acceso a los servicios de aborto seguro al eliminar innecesarias restricciones jurídicas y regulatorias.
Although the great majority of abortions are performed in the first trimester, a significant number are not carried out until the second trimester.Footnote* Data on the global incidence of second trimester abortions are difficult to obtain due to the lack of any statistics in countries where abortion is legally restricted.Citation1 However, estimates have placed the percentage at 10–15% of all abortions.Citation2Citation3 For example, studies have indicated a rate of 13% in the United States and Nigeria, 10% in Canada and Singapore, and 25% in India and South Africa.Citation2Citation3 This is a significant number in light of the fact that an estimated 42 million abortions (figure for 2003) are performed every year, of which 21.6 million (figure for 2008) are unsafe.Citation4 Unsafe second trimester abortions constitute a serious public health problem; they account for two-thirds of the five million estimated admissions to hospital annually for complications of unsafe abortion.Citation4Citation5 They are also responsible for a disproportionate number of abortion-related maternal deaths, even though in some cases they may be misclassified as due to other causes.Citation6Citation7
Historically, there has been little discussion in the literature of second trimester abortions and limited research on the reasons women have them. However, in recent years this has begun to change. In 2008 Reproductive Health Matters published a journal supplement on second trimester abortion,Citation8 with papers from the 2007 International Conference on Second Trimester Abortion.Citation1 Studies from England and Wales, Mozambique, Netherlands, Spain, South Africa, United States and Viet Nam, demonstrate that the factors influencing the need for second trimester abortions are present in almost all societies.Citation9–16 For example, some women do not realize that they are pregnant or are in denial about their pregnancy until the second trimester. Other women face pressure from family members or partners which delays their making a decision, or they are themselves undecided about what course to take. Some decide not to continue a wanted pregnancy after facing difficult altered personal circumstances or a diagnosis of serious fetal anomaly. After the decision to have an abortion is made, other factors can cause delays. These include lack of money to pay for the abortion, lack of information on where it can be obtained, the need to travel long distances, including to another country, to find an abortion provider, concerns about what is involved in undergoing an abortion, and delays in getting a pregnancy test or obtaining a clinic appointment. In addition, the stigma associated with second trimester abortion can cause further delay. These factors are particularly serious for young women, women with little education, poor women, and rural women. Finally, threats to health and life often do not arise until the second or third trimester of pregnancy, and many tests to detect fetal abnormalities cannot be carried out until well into the second trimester.Citation10,17–19
Legal status of second trimester abortions
In light of the need for second trimester abortions, one of the most important factors determining whether they can be safely obtained in a timely fashion is the law governing them and restrictions placed on them. Although there is a substantial body of academic literature on the legality of abortion in various countries, most of it focuses on the lawfulness of abortion in the first trimester.Citation20–26 Analyses of the legality of abortion often do not specify indications or requirements for abortions performed later in pregnancy. This paper focuses on the legality of the procedure in the second trimester and is based, in all but a few cases, on the exact wording of the specific laws and, when available, in regulations for some 191 countries for which information is available.Footnote* It is structured around an analysis of the legality of second trimester abortion according to the most common indications for such abortions which appear in the laws themselves: to preserve the woman's life, physical and mental health reasons, pregnancy due to a sex offence, fetal impairment, socio-economic reasons, and at the woman's request.
As is the case with first trimester abortions, the law does not indicate the extent to which safe abortion is available in practice. This can vary considerably, based on factors such as the willingness of providers, the availability of services, and the attitude of officials and the public as a whole. Thus, while the abortion laws in Great Britain and Ghana are very similar, abortion services are available to meet existing need in Britain but are lacking in Ghana.Citation27 Although it is beyond the scope of this paper to do such analyses, the language in the laws does provide useful information on their theoretical limits and the extent to which they could be applied, and serves as a starting point for further analysis of how they are applied in individual countries and how they can be changed to improve access.
It should be noted at the outset that there exist significant barriers to analysing the legal texts on second trimester abortions. In some cases, the language is convoluted or simply unclear. This can particularly be a problem in trying to determine the upper time limits (in weeks of pregnancy) set for legal abortions. Many laws do not establish time limits, no matter what the indication, while others specify (sometimes different) time limits for certain indications, but not for others. In other laws, a time limit must be inferred from the requirement that an abortion must be carried out before “viability”, a term that is about the chances of pre-term survival in relation to wanted pregnancies and has no one accepted definition,Citation28–32 and arguably no relevance in relation to induced abortion. This paper therefore includes the term as it appears in specific laws, but without seeking to assign a specific meaning to it.
Interpretation of the health indication for abortion can also pose difficulties. The wording of this indication varies greatly from country to country, particularly given the range of languages and legal traditions involved. Sometimes, as in many common law-based laws, there must be a risk to health. Great Britain's law, for example, which has served many former British colonies as a model for reform, allows abortion where “continuance of the pregnancy would involve risk, greater than if the pregnancy were terminated, of injury to the physical or mental health of the pregnant woman…”. Sometimes, as in countries that follow a civil law tradition, there must be a danger to health. Burkina Faso's Penal Code permits abortions when “continuation of the pregnancy… endangers the health of the woman…”. And in some countries there must only be medical or health reasons. In Vanuatu, there must be “good medical reasons”, in Djibouti “therapeutic reasons”, and in Pakistan a requirement of “necessary treatment”. These concepts are not necessarily the same.
Moreover, the degree of risk or danger to health varies. Some laws provide that there must simply be a risk or danger, while others provide that there must be a serious risk or danger, or that an abortion is the only way to prevent serious and/or permanent harm to health. Argentina's Penal Code allows abortion “in order to avert danger to the life or health of the mother if this danger cannot be averted by other means”. As the authors of a recent study of the health indication conclude: “inconsistencies in countries' interpretation and implementation of the health indication and, depending on where women live, the medical practitioners they consult and their ability to defend themselves before public officials, can result in discrepancies in practice and discrimination”.Citation33 In addition, while in some laws only the term “health” is used, this may or may not encompass mental health as well physical health, in line with the current World Health Organization (WHO) definition of health as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity”.Citation34 However, the analysis that follows adopts a conservative approach; that is, mental health is most likely included only when the legal text actually employs the term.
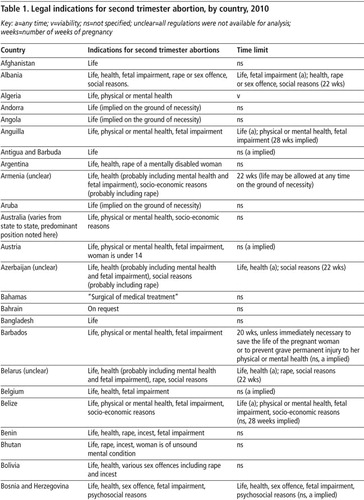
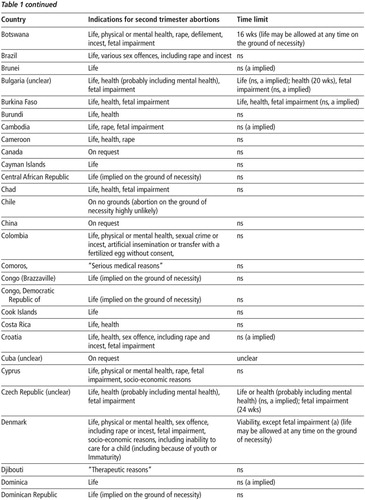
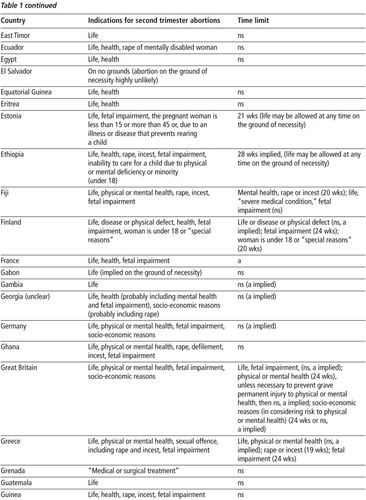
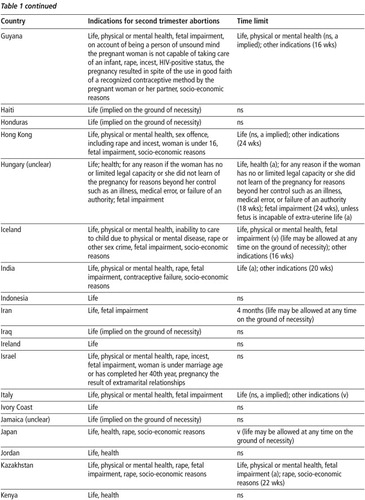
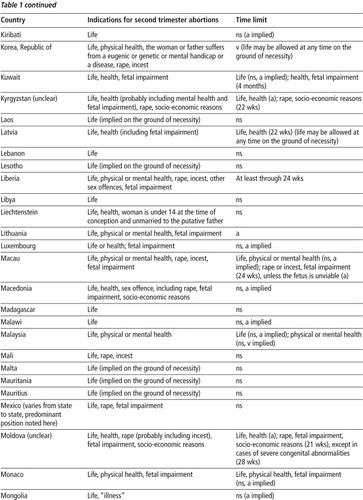
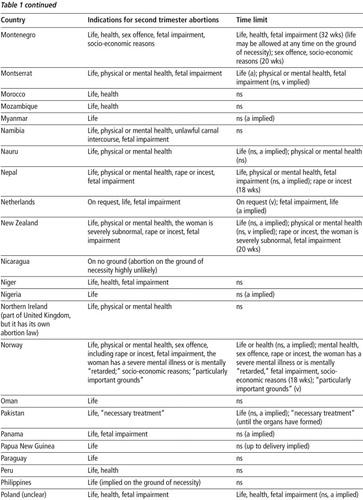
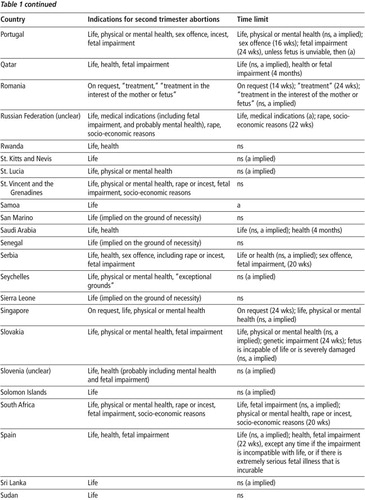
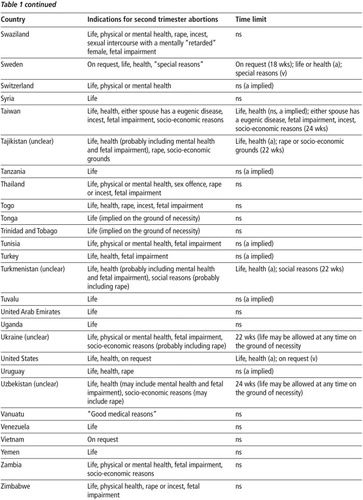
The information in this paper was compiled through the author's personal examination in almost all instances of the full texts of the laws in the original language or in reliable translations.Footnote* To the best of the author's knowledge the texts examined are up to date as of early 2010. The interpretation of laws reflects the best judgment of the author when the wording itself is unclear. Table 1 summarises the legal indications for second trimester abortion in 191 countries. When the provisions of a law are unclear or are implied, rather than clearly stated, as when a time limit is specified for some indications but not for others, or when abortion is defined as a procedure that is performed only up to a specific point during pregnancy, this is noted in the tables.Footnote*
Abortion to preserve the life of the pregnant woman
Almost all countries or jurisdictions in the world with specific laws on abortionFootnote† allow abortion to preserve the life of the pregnant woman. Their laws specify this indication explicitly or, under general criminal law principles of necessity, are interpreted as permitting such abortions. In most cases, no upper time limit is set by these laws, and thus the laws can be presumed to allow such abortions throughout pregnancy.Footnote** In the remaining cases, the upper time limit extends into the second trimester. Of the 191 laws reviewed, 188 allow abortion to preserve the woman's life. In Chile, El Salvador and Nicaragua, abortions are not permitted on any ground at any time during pregnancy.Footnote††
Of these 188 countries' laws, 58 permit abortion only to preserve the life of the pregnant woman at any time during pregnancy; the rest also permit abortions on other grounds. All 58 countries, except Ireland, are developing countries and include some of the most populous and poorest countries in the world, e.g. Afghanistan, Nigeria, Myanmar, Philippines, Tanzania and Uganda. In addition, most are countries where very few legal abortions are performed. These laws are generally broadly worded and do not delineate procedures under which a pregnant woman or physician can request an abortion or specify conditions on facilities or personnel for their performance. Many have not been revised since colonial days.
Abortion for health reasons
Some 113 countries allow abortion to be performed on health grounds during the second trimester. Twenty-five of the 113 countries permit abortion only to save the life of the pregnant woman or to preserve her health. These include Algeria, Argentina, Burundi, Malaysia, Morocco, Pakistan, Peru and Rwanda.
These 113 countries fall into two categories. The first consists of countries that permit abortion most likely only on physical health grounds. Their laws either use the phrase “risk to health” or “danger to health” or “for medical reasons” or specify risk or danger “to physical health”. Some 69 countries are in this category, approximately 67% of them developing countries. As noted earlier, it is often unclear whether “health” also includes mental health. Presumably, such an interpretation is more likely in a country that revised its abortion law after the WHO definition was formulated in 1946, than in a country with a law formulated prior to that.Footnote***
The second category consists of countries that specifically allow abortion for mental health reasons. Some 45 countries fall within this classification, slightly over half of them developing countries.
Only about 25% of the 113 countries' laws set time limits on abortion. These range from 16 weeks (four countries) to 32 weeks (one country), and in seven countries at “viability”. Except for those that permit abortion on health grounds at any time during pregnancy, the remainder do not specify a time limit, so it is unclear whether abortions are allowed at any time during the second trimester or not. As is the case for most of the countries that permit abortions only to preserve the life of the pregnant woman, many of these countries' laws are broadly worded and fail to specify facilities, personnel or approval requirements for the performance of abortions.
Abortion for fetal impairment
The most common additional legal indication for second trimester abortion is fetal impairment or anomaly. This may reflect the growing sophistication and use of technology that can detect a genetic or physical abnormality, which is also increasingly available in developing countries. As with the health indication, interpretation of an indication of fetal impairment can pose difficulties. The most significant is a definition of what sort of fetal impairment is sufficiently serious to justify an abortion. This question has been addressed by some government ministries and medical professional associations. For example, in a position paper, the Netherlands Ministry of Health Welfare concluded that termination of pregnancy after 24 weeks was warranted in cases in which “the unborn child cannot reasonably be expected to survive outside the mother's body” or in which there are “fetal anomalies leading to serious and incurable functional disorders but which might reasonably be expected to have a chance of survival, although mostly a very limited one”.Citation40 In a 2010 report, the UK's Royal College of Obstetricians & Gynaecologists (RCOG) advised that a number of factors be considered, including the potential for effective treatment; the probable degree of self-awareness on the part of the child and of the ability to communicate with others; the suffering that would be experienced; the probability of the child being able to live alone and to be self-supporting as an adult; and on the part of society, the extent to which actions performed by individuals without disability that are essential for health would have to be provided by others.Citation41 The RCOG decided against specifying the types of fetal impairment that justify an abortion, and in fact almost no laws do so, as is also the case with the health indication.
Actual wording of the laws varies from country to country. In almost all countries the fetal impairment must be considered serious. For example, in Great Britain and many of its former colonies there must be “a substantial risk that if the child were born it would suffer from such physical or mental abnormalities as to be seriously handicapped”. In many countries the impairment must also be incurable. In France and a number of its former colonies, and countries influenced by French law, there must be “a strong possibility that the unborn child will suffer from a particularly serious condition recognized as incurable at the time of diagnosis”. A few countries, such as Israel, Nepal and Slovakia, however, specify neither requirement. Whether these differences in wording make a practical difference or not is unclear.
Some 69 countries specifically authorise abortions for this reason in the second trimester, almost evenly divided between developing and developed countries. Almost all of the countries that permit such abortions in the second trimester also authorise abortion in the second trimester for health reasons – only a few such as Cambodia, Iran, Mexico and Panama do not. Unlike the laws already discussed, the laws of most of these countries are usually detailed in nature and set forth requirements as to facilities, personnel, and approval procedures. Moreover, 42% of these countries set time limits on abortions for fetal impairment, ranging from 16 weeks (five countries) to 24 weeks (ten countries), “viability” (two countries) to 32 weeks (one country). This is a far greater percentage of countries setting such time limits than those setting limits for abortions on health grounds. However, even if an abortion cannot be performed on grounds of fetal impairment beyond a fixed upper time limit, it might well be justified on health grounds.
Abortion for pregnancy resulting from a sex offence
The next most common indication for second trimester abortions, after life, health, and fetal impairment, is if the pregnancy resulted from a sex offence, most commonly rape, and in some but not all cases, incest. There are some 49 countries whose laws include this indication, approximately half of them developed countries. Almost 80% are the same countries that authorise abortion for fetal impairment, and almost all also permit abortions for health reasons. 57% of these countries set time limits on such abortions. These range from 16 weeks (four countries) to “viability” (two countries), with a lower average time limit than for abortions on health or fetal impairment grounds (see Table 1). The lower time limit may reflect a belief that a woman (or girl) should be able to seek an abortion for a pregnancy resulting from a sex offence earlier than for other reasons. However, there is some evidence that women may be delayed in reporting rape and therefore in being able to seek an early abortion.Citation42 A number of these countries also require more than the woman's statement that the pregnancy resulted from a sexual offence. For example, in Bolivia a prosecution must have been initiated. In Cameroon, there must be a certificate from the prosecutor of a good case. In Hong Kong, the woman must make a report to a police officer. In Zimbabwe, a complaint must be lodged with the authorities. At least 12 countries require the approval of a committee or of two or more physicians.
Abortion on socio-economic grounds and/or on request
Thirty-two countries allow second trimester abortions on broad socio-economic grounds. All of these countries also permit abortions for other reasons; 81% are developed countries or former Soviet republics or Soviet bloc countries that have long had liberal abortion laws. They include Great Britain, India, Japan, Russian Federation, South Africa and Ukraine. 69% set specific time limits for such abortions, ranging from 16 weeks (two countries) to 22 weeks (ten countries) to “viability” (two countries).
Some of the countries with this indication, including Denmark, Guyana, Norway, Russian Federation, South Africa, and most former Soviet republics, allow abortion on request in the first trimester of pregnancy; others, including Great Britain, Iceland, India and Zambia do not. A few countries authorise second trimester abortions for specific, limited socio-economic reasons, e.g. the pregnant woman/girl is of unsound mind (Bhutan, Hungary, New Zealand, Norway); the pregnancy is due to contraceptive failure (Guyana, India); the woman is HIV-positive (Guyana); the woman is over a specified age (Estonia, Israel); the pregnancy is the result of extramarital relations (Israel); the pregnancy was not discovered earlier (Hungary); the pregnant woman/girl or the father suffers from a genetic disease (Republic of Korea, Taiwan); the pregnant woman/girl is unable to care for a child (Denmark, Estonia, Ethiopia, Guyana); and the pregnant girl/woman is under a specified age (Austria, Estonia, Ethiopia, Finland, Hong Kong, Israel, Liechtenstein). The specified age varies from under 14 to under 18, to under the age of marriage. The last of these is notable in light of arguments for and against parental consent for minors to obtain an abortion in many countries.
Ten countries permit second trimester abortion on request. This contrasts with 54 countries that allow abortion on request only in the first trimester.Citation21 Four of the ten do not set upper time limits on second trimester abortions. Sweden specifies 18 weeks, Singapore 24 weeks, and the Netherlands and the United States “viability,” but all allow some abortions on specific grounds after that. Eight of the ten countries are either developed countries or former Soviet bloc countries. With notable exceptions, such as India and South Africa, countries allowing abortion for socio-economic reasons or on request in the second trimester are places where obtaining a second trimester abortion is relatively easy and safe.Citation43Citation44
China does not have a specific abortion law at all, and in Canada abortion was decriminalized in 1988–89 when the Supreme Court ruled that the abortion provisions of Canada's Criminal Code violated the Canadian Charter of Rights and Freedoms, and the Parliament failed to enact new provisions.Citation45 Abortion may be assumed to be on request without legal restrictions in both countries. However, practice may still be restricted, including the availability of second trimester abortion services.Footnote* In 2002, the Australian Capital Territory also decriminalised abortion without reference to length of pregnancy.
Additional legal factors
An analysis of the permitted indications and upper time limits for second trimester abortions tells only part of the story on the legal availability of the procedure. Many abortion laws establish additional conditions for carrying out abortions that can greatly affect access. One of these relates to who can perform abortions. Very few countries allow persons other than a physician to carry out a second trimester abortion, and some, such as Bulgaria, Greece, Libya, Madagascar, Seychelles and Turkey, mandate that the physician be an obstetrician/gynaecologist or have special training. However, this is now slowly changing for both first and second trimester medical abortions,Footnote* with trained nurses, midwives and other mid-level providers able to manage these abortions alone.Citation46 Moreover, many laws allow conscientious objection on the part of individual providers, although sometimes not if the life of the woman is at risk (e.g. Great Britain, Seychelles, Singapore and Zimbabwe).
A second restriction relates to sometimes time-consuming approval procedures for abortions. In many countries, such as Anguilla, Barbados, Bulgaria, Burundi and Cambodia, for example, two or more physicians or a commission must approve the abortion. Often these restrictions increase with the length of pregnancy, as in Barbados, Finland, Guyana and South Africa. Some laws also require the consent of a parent if the woman is a minor (e.g. Croatia, Poland, Saudi Arabia, Turkey) or a spouse if she is married (e.g. Equatorial Guinea, Japan, Kuwait). If such consent is not obtained, a woman usually has no legal recourse. Although a number of countries allow a court or medical committee to authorise the abortion when a parent refuses (e.g. Denmark, Italy, several US states), this too can result in delay. In addition, some countries specify waiting/reflection periods before a woman can obtain an abortion (e.g. Belgium, Germany, Saint Lucia, Netherlands).
Another restriction relates to places where abortions can be carried out. A number of countries, such as Luxembourg, Montserrat, New Zealand, Singapore and Tunisia, require licensing or approval of abortion facilities. Others, such as Kuwait, Rwanda, Togo and Zambia, limit the performance of abortions to hospitals or similar institutions, while still others, such as Ethiopia, Israel, Serbia, Taiwan, Thailand and Turkey, set forth detailed requirements that an institution must meet in order to carry out abortions. A final requirement is the prohibition of abortion advertisements (e.g. Albania, Eritrea, Greece).
These restrictions may be intended to create barriers to providing and obtaining abortions, e.g. in many US states.Citation52 On the other hand, such requirements may be intended to protect women, e.g. to prevent abortions by unqualified personnel in unsafe facilities, as stated in guidelines adopted by Ethiopia and Viet Nam, for example. Moreover, it should not be inferred that if countries do not have conditions for the performance of second trimester abortions, it is easier to access them. On the contrary, these countries are more often places where very few legal abortions are carried out for any reason. Countries with such requirements have usually decided to allow abortion.
Nonetheless, the question of which requirements remain necessary, given the increasing safety and simplicity of providing second trimester abortions, particularly medical abortions in many settings, must be raised.
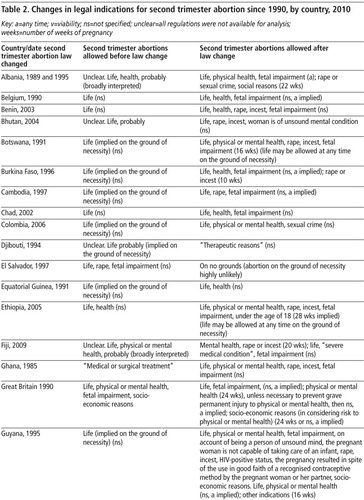
Trends
Table 2 summarises changes in second trimester abortion laws that have occurred since 1990. At least 30 countries have significantly expanded indications for abortion.Citation20Citation21 These include Albania, Bhutan, Botswana, Cambodia, Colombia, Ethiopia, Fiji, Ghana, Guyana, Indonesia, Monaco, Nepal, Portugal, Saint Lucia, South Africa, Spain, Swaziland, Switzerland and Thailand. Five West African Francophone countries liberalised their abortion laws by means of comprehensive reproductive health legislation as well, and Kenya's new Constitution, approved by referendum in August 2010, allows abortion on grounds of life and health and leaves open the possibility that a law could subsequently be enacted that permits abortion on additional grounds. Almost all of these changes affect the legal status of second trimester abortions, whether by increasing indications for abortion without setting upper time limits, by endorsing specific indications for abortion with time limits, or both.Citation20Citation21 In addition, many countries have registered the use of mifepristone and/or misoprostol for inducing abortion, often only for the first nine weeks of pregnancy,Citation53Citation54 but off-label use in the second trimester is common, (Beverly Winikoff, Expanding access through off-label use of medical abortion, conference presentation, March 2010),Citation1 e.g. in Great Britain and the US, and across Scandinavia.
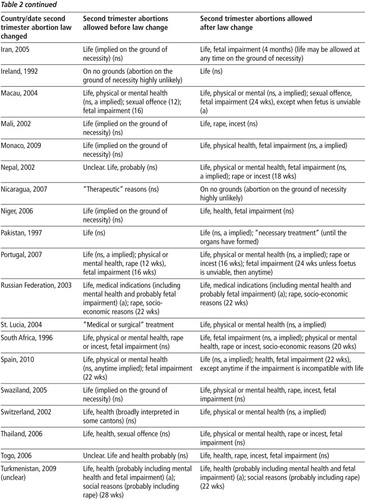
At the same time there have been moves in some countries to lower the upper time limit for second trimester abortions. In 2009, following developments in many former Soviet republics, Turkmenistan reduced the upper time limit on abortion for social reasons from 28 to 22 weeks. In Spain, although the new abortion law liberalised abortion by allowing it on request during the first 14 weeks of pregnancy, it also placed a time limit of 22 weeks on abortions performed when the health of the pregnant woman is threatened. In 2003, the Russian Federation reduced the more than ten socio-economic indications for abortions between 12 and 22 weeks to four: in cases where a court rules a woman is unfit to be a mother, in the case of rape, where the father is either very sick or dies, or where the woman is sent to prison.Citation20Citation55
Similarly some countries are placing greater procedural restrictions on the performance of abortions later in pregnancy. In 2009, for example, Germany added new procedural requirements relating to the provision of information and a reflection period for abortions sought on grounds of fetal impairment. Some proponents of these changes were said to want to create barriers to these abortions, while others were concerned that women were not getting the counselling they needed when fetal impairments were detected. In 2007, the US Supreme Court upheld a ban on a particular form of D&E used in the second trimester, following a successful campaign against it by the anti-abortion movement.Citation56
It is not entirely clear what is driving moves to restrict the performance of abortions after the first trimester. The proponents of such changes often argue that advances in medical technology have allowed prematurely born babies to survive at earlier ages and, thus the abortion time limit should be lowered to below 24 weeks of pregnancy. As the authors of a recent study on post-first trimester abortions in England and Wales point out, however, these critics seldom question the ethics of restricting access to abortion or acknowledge the compelling reasons that lead women to have abortions after the first trimester.Citation10 In any case, there is no scientific support for such changes.Citation28Citation32 One of the few bodies that examined the evidence in detail, the UK Parliament's Science and Technology Committee, concluded in 2007 that there was no justification for lowering the legal time limit on abortion.Citation29
Discussion and recommendations
Key findings of this review are summarised in Box 1. Given that there are serious reasons why women have second trimester abortions, and that the laws in many countries do not make such abortions available, an important question to ask is how laws and regulations can be changed in order better to respond to women's needs, as well as to reduce delays in accessing abortions as early as possible. In 2007, the International Conference on Second Trimester Abortion, organised by the International Consortium for Medical Abortion, adopted recommendations that take a forward-looking approach.Citation57 These include that abortion be completely decriminalised and made available at a woman's request. Short of that, they propose that the health indication for abortion should include mental as well as physical health, that judicial or administrative approval requirements for abortion following sex offences be removed, that there should be no upper time limit on abortions, and that regulatory conditions whose purpose is to impose access barriers be removed.

WHO's 2003 Safe Abortion: Technical and Policy Guidance for Health Systems Footnote* contains a detailed analysis of access barriers and recommendations for their removal.Citation17 For example, it proposes reducing or eliminating administrative and regulatory barriers in areas such as physician or committee authorisation, restrictive time limits, waiting periods, spousal and parental approval, facility and physician-only requirements, fees, licensing, and the reporting of rape. The broader aim of this guidance and its technical and policy recommendations is to provide evidence-based recommendations for making all abortions safe.
While it may be politically unrealistic to expect most countries to decriminalise all abortions in the near future, especially in the second trimester, less comprehensive legislative and regulatoryFootnote* changes are possible. These include recommendations aimed at ensuring that abortions are carried out as early as possible in pregnancy, and improving women's access to safe abortions through the removal of clinically unnecessary legal and regulatory restrictions.
All countries should allow abortions to preserve the woman's life, for broad physical and mental health reasons, and in cases of rape, incest and fetal impairment throughout the first and second trimesters of pregnancy. Moreover, countries could amend requirements on facilities and providers so that they are evidence-based, reflect current best practice and aim only to protect the health of the woman. Best practice with regards to induced abortion has changed substantially in the past 20+ years, and laws and regulations need to have the flexibility built into them to respond to these changes, both on grounds of safety and to keep costs as low as possible for women and health systems. For example, nurses, midwives, and other mid-level providers with appropriate training could be authorized to manage both first and second trimester medical abortion in modest inpatient facilities with good referral links for emergency medical care for the very small proportion of women who may need it.Citation47 In addition, there should be no requirement that a commission or more than one physician authorize any abortion.
Spousal approval should never be necessary. Serious consideration should also be given to removing requirements for parental approval for minors to obtain an abortion, particularly where rape and incest may have been involved. Moreover, there should be no requirement that rape be reported or investigated, or that a magistrate give approval for abortions performed on this ground. In general, laws and regulations should be based on scientific evidence, be clear and uniform, and facilitate access to legal abortions. This would signal a government's commitment to allowing legal abortions to be performed, and allow women, health service managers, health and legal professionals and the public to understand the parameters of the law. It would also make it possible for improvements in abortion methods, which have developed continuously since 1980, to be incorporated into service delivery without delays, as currently occurs due to outdated laws and regulations, and support training for providers, so that out-of-date and less safe methods stop being used.
Regulations should call for the expeditious referral of patients seeking abortions by health personnel to an abortion provider, and their expeditious treatment once they have been referred. There is a growing body of sentiment that health care professionals who assert a “conscientious objection” and their institutions still have a duty to ensure that their patients have access to abortion.Citation48–51 Furthermore, governments should oversee and monitor the implementation of conscientious objection clauses so that women can actually access the services they are legally entitled to receive.
Governments should create women-supportive services that ensure privacy, confidentiality and compassionate and non-judgmental treatment, taking into account the experiences and needs of adolescents, and young and poor women especially. They should ensure that women, health personnel and the public in general are educated about the law and where to obtain safe abortion information and services. They should consider providing abortion services free of charge or ensuring that costs do not prevent any woman who needs an abortion from having one.
Training for health personnel in safe abortion procedures, including for second trimester abortions, and addressing the emotional needs of women seeking abortions through provision of accurate information, and unbiased counselling (if requested by the woman), should be a required part of pre-service training for physicians and nurses in any country where abortion is legal for at least one indication. Lastly, improving access to early pregnancy testing, strengthening sex education and access to contraception, particularly for under-served groups such as adolescents and single women and men, the poor and rural populations, would go a long way towards reducing unwanted pregnancies. UNESCO has recently published helpful guidance on this issue.Citation59 These measures would address women's need for safe, legal first and second trimester abortions in a comprehensive fashion.
Acknowledgements
The author would like to thank the International Consortium for Medical Abortion for their financial support for the research for this paper, which was commissioned by them.
Notes
* Reflecting medical practice in the latter half of the 20th century, most of the world's countries that have liberalised their abortion laws based those laws on when in pregnancy certain abortion methods were used, i.e. in the first trimester (up to 13 weeks), or the second trimester (through 28 weeks). This division is becoming outdated due to the advent of new methods, particularly medical abortion pills, and changes in medical practice. The law tends to change more slowly than medical practice, however. Abortion is currently most often widely allowed in the first trimester and less often in the second trimester, and is largely not allowed after 28 weeks of pregnancy, with exceptions.
* When the word “law” is used in this article, it is intended to encompass available regulations. The distinction between laws and regulations is not always clear. Laws are in general approved by a legislative body and set forth broad provisions on what is allowed and not allowed and certain requirements that must be met; regulations, on the other hand, are usually issued by administrative agencies such as ministries and usually deal with the implementation of laws and what might be called procedural issues. In the context of abortion, a law might simply set forth the indications for the legal performance of abortion. Regulations might deal with how to determine if an indication is present, as well as with issues of parental or spousal consent, persons allowed to perform abortions, facility requirements, informed consent, conscientious objection, record-keeping, confidentiality, provider approval procedures, etc. However, practice varies widely. Some governments have chosen to incorporate many of these aspects into the abortion law itself, leaving regulations to deal with relatively minor matters such as the designation of named facilities or the publication of forms for reporting abortions. Others have enacted relatively concise abortion laws setting forth only the circumstances under which abortions can legally be performed, and reserving all other issues for regulations. Still other countries, usually those where abortion laws are highly restrictive, have issued no regulations.
* The full text of the world's abortion laws can be consulted at the web site of the Annual Review of Population Law.Citation35 Consequently no individual laws are referenced in the article. The author is responsible for maintaining the website and keeping its information, particularly on abortion, up to date.
* This article deals with abortion as a public health issue. It does not discuss the many important human rights issues surrounding abortion, as these have been covered in numerous papers and reports in recent years.Citation36–38 Dealing with abortion as a health issue does not necessarily lead to asserting a broad human right to abortion, although it may lead indirectly to asserting a right to health. Law is not just about rights; it is most often about giving legal effect to policies that will bring about desired outcomes, and that is the perspective on abortion law that this paper takes.
† For example, in Australia and Mexico, individual states and territories regulate abortion. Northern Ireland is still governed by the abortion law that was in force in the United Kingdom before the 1967 Abortion Act, which covers only Great Britain. Macau and Hong Kong have laws differing from that governing the rest of China, which were in large part carried over from colonial days. When this paper uses the term “country”, it should also be understood to include specific jurisdictions.
** Time limits (length of pregnancy or gestational age) in this article are based on the number of weeks from the first day of the last menstrual period.
†† Although abortion on the grounds of necessity is theoretically possible in these countries, it is usually presumed that no abortions are legal, because all three countries deliberately enacted legislation removing any legal grounds for abortion in recent decades.Citation20
*** It is notable that at least one international body, the Human Rights Committee, has applied the WHO definition of health in interpreting a law that was enacted before the WHO definition was adopted. In KL v. Peru it ruled that Peru was in violation of the International Covenant on Civil and Political Rights for not allowing an abortion to a woman carrying an anaencephalic fetus, partly on the ground that Peru's law has a health exception and that the records showed she was suffering psychologically as a result of the diagnosis.Citation39
* In Canada, for example, issues of access continue to make it difficult for rural women to obtain abortions without travelling great distances. Discussed in Rodgers S. Abortion denied: bearing the limits of law. (Manuscript as at March 2007), referenced in Berer.Citation8
* Medical abortion here means first and second trimester abortion with a combination of mifepristone and misoprostol or with misoprostol alone.Citation17
* This Guidance is being amended and updated by the Department of Reproductive Health and Research/Special Programme on Human Reproduction at WHO at this writing.
* Indeed, the Western Hemisphere Region of the International Planned Parenthood Federation has formulated model regulations for the provision of legal abortion services.Citation58
Related Research Data
References
- International Conference on Second Trimester Abortion. Conference Report. 29–31 March 2007, London. At: <www.medicalabortionconsortium.org/activities/conference-report-29-31-march-2007-london-uk-5.html>. Accessed 25 February 2010
- PA Lohr, JL Hayes, K Gemzell-Danielsson. Surgical versus medical methods for second trimester induced abortion. Cochrane Database of Systematic Reviews. 1: 2008; CD006714.At: <http://apps.who.int/rhl/reviews/CD006714.pdf>. Accessed 25 February 2010
- South Africa. Department of Health. Termination of pregnancy update: cumulative statistics through 2004. 2005; Department of Health: Pretoria.
- Unsafe abortion: global and regional estimates of the incidence of unsafe abortion and associated mortality in 2008. 6th update, 2010 (Forthcoming); WHO: Geneva.
- S Singh. Hospital admissions resulting from unsafe abortion: estimates from 13 developing countries. Lancet. 368: 2006; 1887–1892.
- JA Unuigbe, AU Oronsaye, AAE Orhue. Abortion-related morbidity and mortality in Benin City, Nigeria: 1973–1985. International Journal of Gynecology & Obstetrics. 26(3): 1988; 435–439.
- D Walker, L Campero, H Espinoza. Deaths from complications of unsafe abortion: misclassified second trimester deaths. Reproductive Health Matters. 12(24 Suppl): 2004; 27–38.
- M Berer. Second trimester abortion: public policy, women's health [Editorial]. Reproductive Health Matters. 16(31 Suppl): 2008; 3–13.
- TD Tuyet Hoang, Phan Thuy, NK Trang Huynh. Second trimester abortion in Viet Nam: changing to recommended methods and improving service delivery. Reproductive Health Matters. 16(31 Suppl): 2008; 145–150.
- R Ingham, E Lee, SJ Clements. Reasons for second trimester abortions in England and Wales. Reproductive Health Matters. 16(31 Suppl): 2008; 18–29.
- MB Ustá, EMH Mitchell, H Gebreselassie. Who is excluded when abortion access is restricted to twelve weeks?: evidence from Maputo, Mozambique. Reproductive Health Matters. 16(31 Suppl): 2008; 14–17.
- L Font-Ribera, G Pérez, A Espelt. Determinants of induced abortion delay. Gaceta sanitaria / S.E.S.P.A.S. 23(5): 2009; 415–419.
- O Loeber, C Wijsen. Factors influencing the percentage of second trimester abortions in the Netherlands. Reproductive Health Matters. 16(31 Suppl): 2008; 30–36.
- J Harries, P Orner, M Gabriel. Delays in seeking an abortion until the second trimester: a qualitative study in South Africa. Reproductive Health. 4: 2007; 7.At: <www.ncbi.nlm.nih.gov/pmc/articles/PMC2039724/>. Accessed 14 May 2010
- EA Drey, DG Foster, RA Jackson. Risk factors associated with presenting for abortion in the second trimester. Obstetrics & Gynecology. 107(1): 2006; 128–135.
- MF Gallo, NC Nghia. Real life is different: a qualitative study of why women delay abortion until the second trimester in Vietnam. Social Science & Medicine. 64(9): 2007; 1812–1822.
- World Health Organization. Safe Abortion: Technical and Policy Guidance for Health Systems. 2003; WHO: Geneva.
- D Singh, JR Singh, V Kumar. Prenatal diagnosis for congenital malformations and genetic disorders. Emedicine. 2008. At: <http://emedicine.medscape.com/article/1200683-overview>. Accessed 25 February 2010
- RD Wilson. Amended Canadian guideline for prenatal diagnosis (2005): change to 2005-techniques for prenatal diagnosis. JOGC Clinical Practice Guidelines. 168: 2005. At: <www.sogc.org/guidelines/public/168E-CPG-November2005.pdf>. Accessed 25 February 2010
- R Boland, L Katzive. Developments in laws on induced abortion: 1998–2007. International Family Planning Perspectives. 34(3): 2008; 110–120. At: <www.guttmacher.org/pubs/journals/3411008.html>. Accessed 25 February 2010
- A Rahman, L Katzive, SK Henshaw. A global review of laws on induced abortion, 1985–1997. International Family Planning Perspectives. 24(2): 1998; 56–64. At: <www.guttmacher.org/pubs/journals/2405698.html>. Accessed 25 February 2010
- SK Henshaw. Induced abortion: a world review. Family Planning Perspectives. 22: 1990; 76–89. At: <www.guttmacher.org/pubs/journals/2405698.html>. Accessed 26 February 2010
- RJ Cook, BM Dickens. Issues in Reproductive Health Law in the Commonwealth. 1986; Commonwealth Secretariat: London.
- RJ Cook, BM Dickens. Emerging Issues in Commonwealth Abortion Laws. 1982; Commonwealth Secretariat: London.
- United Nations Population Division. Department of Economic and Social Affairs. Abortion policies: a global review. 2002; UN: New YorkAt: <www.un.org/esa/population/publications/abortion/index.htm>. Accessed 26 February 2010
- Center for Reproductive Rights. The world's abortion laws 2008, poster. 2007; CRR: New YorkAt: <http://reproductiverights.org/sites/crr.civicactions.net/files/pub_fac_abortionlaws2008.pdf>. Accessed 26 February 2010
- RAS Morhee, ESK Morhee. Overview of the law and availability of abortion services in Ghana. Ghana Medical Journal. 40(3): 2006; 80–86. At: <www.ncbi.nlm.nih.gov/pmc/articles/PMC1790853/>. Accessed 26 February 2010
- I Seri, J Evans. Limits of viability: definition of the gray zone. Journal of Perinatology. 28: 2008; S4–S8. At: <www.nature.com/jp/journal/v28/n1s/full/jp200842a.html>. Accessed 26 February 2010
- United Kingdom House of Commons Science and Technology Committee. Scientific developments relating to the Abortion Act 1967, 12th report of session 2006-07, Vol. 1 (HC 1045-1). September 2007. At: <www.publications.parliament.uk/pa/cm200607/cmselect/cmsctech/1045/1045i.pdf>. Accessed 26 February 2010
- British Medical Association. Fetal viability: a briefing paper from the BMA. 2005. At: <www.bma.org.uk/ethics/reproduction_genetics/AbortionTimeLimits.jsp?page=6>. Accessed 15 August 2010
- Royal College of Obstetricians and Gynaecologists. Fetal awareness: review of research and recommendations for practice. 2010; RCOG: London.
- Pro-Choice Forum. Late abortion: a review of the evidence. A briefing. 2008; Pro-Choice Forum: CanterburyAt: <www.prochoiceforum.org.uk/pdf/PCF_late_abortion08.pdf>. Accessed 26 February 2010
- A Ortega Ortiz. Review of: Causal salud: interrupción legal de embarazo, ética y derechos humanos. Bogotá: FLASOG; 2008. Reproductive Health Matters. 17(33): 2009; 181–182.
- World Health Organization. Constitution, 22 July 1946, Preamble. At: <www.who.int/governance/eb/who_constitution_en.pdf>. Accessed 26 February 2010
- Annual Review of Population Law. Abortion Laws of the World. At: <www.hsph.harvard.edu/population/abortion/abortionlaws.htm>. Accessed 26 February 2010
- C Zampas, JM Gher. Abortion as a human right: international and regionsl standards. Human Rights Review. 8(2): 2008; 249–294.
- RJ Cook, B Dickens. Human rights and abortion laws. International Journal of Gynecology and Obstetrics. 65: 1999; 81–87.
- Ipas. Human rights, unwanted pregnancy and abortion-related care: reference information and illustrative cases. 2002. At: <www.ipas.org/Publications/asset_upload_file568_2443.pdf>. Accessed 15 August 2010
- United Nations Human Rights Committee. KL v. Peru. 2005.
- Netherlands. Ministry of Health Welfare and Sport. [Termination of life neonates] (Parliamentary document). 2006.
- Royal College of Obstetricians & Gynaecologists. Termination of Pregnancy for Fetal Abnormality in England, Scotland and Wales: report of a working party. 2010; RCOG: London.
- E Díaz Amado, MC Calderón García, K Romero Cristancho. Obstacles and challenges following the partial decriminalisation of abortion in Colombia. Reproductive Health Matters. 18(36): 2010; 118–126.
- G Sedgh, S Henshaw, S Singh. Induced abortion: rates and trends worldwide. Lancet. 370: 2007; 1338–1345.
- SK Henshaw, S Singh, T Haas. The incidence of abortion worldwide. International Family Planning Perspectives. 25(Suppl.): 1999; S30–S38.
- Canada. Supreme Court. R. v. Morgenthaler. 1988.
- M Berer. Provision of abortion by mid-level providers: international policy, practice and perspectives. Bulletin of World Health Organization. 87: 2009; 58–63.
- Information for health care providers. Information Package on Medical Abortion. International Consortium for Medical Abortion website. At: <www.medicalabortionconsortium.org/articles/for-health-care-providers/health/?bl=en>. Accessed 21 August 2010
- RJ Cook, BM Dickens. The scope and limits of conscientious objection. International Journal of Gynecology and Obstetrics. 71: 2000; 71–77.
- American College of Obstetricians and Gynecologists Committee on Ethics. The limits of conscientious refusal in reproductive medicine (Opinion No. 385). 2007. At: <www.acog.org/from_home/publications/ethics/co385.pdf>. Accessed 14 August 2010
- International Federation of Gynecology & Obstetrics. Resolution on “Conscientious Objection.” 2006. At: <www.figo.org/projects/conscientious>. Accessed 14 August 2010
- L Casas. Invoking conscientious objection in reproductive health care: evolving issues in Peru, Mexico and Chile. Reproductive Health Matters. 17(34): 2009; 78–87.
- Center for Reproductive Rights. Defending human rights: abortion providers facing threats, restrictions, and harassment. 2009; Center for Reproductive Rights: New York.
- Gynuity Health Projects. Mifepristone approval. At: <http://gynuity.org/resources/info/list-of-mifepristone-approval/>. Accessed 12 August 2010
- Gynuity Health Projects. Misoprostol approved. At: <http://gynuity.org/resources/info/map-of-misoprostol-approval/>. Accessed 12 August 2010
- T Parfitt. Russia moves to curb abortion rates. Lancet. 362(1988): 2003; 968.
- United States Supreme Court. Gonzales v. Carhart, Case No. 05-380. 2007. At: <www.supremecourtus.gov/opinions/06pdf/05-380.pdf>. Accessed 12 August 2008
- International Conference on Second Trimester Abortion. Recommendations, 29–31 March 2007. Reproductive Health Matters. 16(31 Suppl.): 2008; 205–206.
- International Planned Parenthood Federation. Western Hemisphere Region. Legal abortion: a comparative analysis of health regulations. 2009. At: <www.ippfwhr.org/sites/default/files/Legal_Abortion.pdf>. Accessed 14 August 2010
- United Nations Education, Scientific and Cultural Organization. International technical guidance on sexuality education: an evidence-informed approach for schools, teachers and health educators. 2009; UNESCO: Paris.