Abstract
Abstract
The fall of state socialism in Poland in 1989 constituted a critical moment which redefined policies on reproductive health care and access to family planning, influenced by the renewed power of the Catholic church. Poland also embarked on neoliberal economic reforms that resulted in major cutbacks in social services and state health care coverage. The confluence of the elimination of contraceptive subsidies, privatisation of health care, and the intensification of bribes to underpaid health care providers created new challenges for women in accessing services. Furthermore, the 1993 ban on abortion resulted in a nearly total privatisation of this service, which is currently available clandestinely at a high price. Drawing on anthropological research in the Gdańsk metropolitan region in 2007, this paper examines the restrictions on access to family planning, abortion, maternity care, assisted reproduction and other gynaecological services. It draws attention to the urgent need for state-subsidised family planning and other reproductive health services, the reform of abortion law, and regulation of privatised services. Higher wages for public sector health professionals and better public health provision would curb informal payments. The state should support the legitimacy of women's health needs and reproductive and sexual autonomy.
Résumé
La fin du socialisme d'État en Pologne en 1989 a déclenché une redéfinition des politiques sur les soins de santé génésique et de l'accès à la planification familiale, influencée par le pouvoir accru de l'Église catholique. La Pologne a aussi entrepris des réformes économiques néolibérales qui ont abouti à des coupes sombres dans les services sociaux et la couverture sanitaire étatique. La confluence de l'élimination des subventions aux contraceptifs, la privatisation des soins de santé et l'intensification des pots-de-vin versés aux prestataires de soins de santé sous-rémunérés a créé de nouveaux obstacles empêchant les femmes d'accéder aux services. De plus, l'interdiction de l'avortement en 1993 a provoqué une privatisation presque totale de ce service, qui est actuellement disponible clandestinement à un prix élevé. Se fondant sur une recherche anthropologique dans la région métropolitaine de Gdańsk en 2007, cet article examine les restrictions de l'accès à la planification familiale, à l'avortement, aux soins maternels, à la procréation assistée et à d'autres services gynécologiques. Il montre qu'il est urgent de disposer de services de planification familiale et autres soins de santé génésique subventionnés par l'État, de réformer la loi sur l'avortement et de réguler les services privatisés. Des salaires plus élevés des professionnels du secteur public et de meilleures prestations de santé publique diminueraient les paiements informels. L'État devrait soutenir la légitimité des besoins de santé des femmes et leur autonomie génésique.
Resumen
La caída del socialismo en Polonia en 1989 constituyó un momento crítico, que redefinió las políticas referentes a los servicios de salud reproductiva y el acceso a la planificación familiar, en las cuales influyó el poder renovado de la Iglesia católica. Polonia también emprendió reformas económicas neoliberales, que produjeron considerables recortes en los servicios sociales y en la cobertura estatal de los servicios de salud. La confluencia de la eliminación de subsidios para anticonceptivos, la privatización de los servicios de salud y la intensificación de los sobornos a profesionales de la salud mal remunerados, creó nuevos retos para las mujeres en cuanto al acceso a los servicios. La prohibición del aborto en 1993 resultó en la privatización casi total de este servicio, el cual actualmente se ofrece clandestinamente a un precio muy caro. Basado en una investigación antropológica realizada en 2007 en la región metropolitana de Gdańsk, este artículo examina las restricciones al acceso a los servicios de planificación familiar, aborto, atención materna, reproducción asistida y otros servicios ginecológicos. Destaca la necesidad urgente de servicios de planificación familiar y otros servicios de salud reproductiva subsidiados por el Estado, la reforma de la ley de aborto y la regulación de los servicios privatizados. Los pagos extraoficiales se pueden reducir mediante sueldos más altos para profesionales de la salud del sector público y una mejor prestación de servicios de salud pública. El Estado debería apoyar la legitimidad de las necesidades de salud de las mujeres y su autonomía reproductiva y sexual.
The hallmark of the state socialist regime in Poland, in power from 1947 to 1989, was the separation of church and state, which particularly benefited women. Despite the historical strength of the Polish Catholic church, the socialist state's universal health care system openly endorsed family planning. In 1956, after Stalin's death and during the so-called post-Stalin thaw when Soviet control was partially eased, the Polish state legalised abortion for socio-economic reasons and subsidised it fully in public hospitals. It failed to legalise sterilisation, however, which was criminalise in 1932 and remains illegal.Citation1Citation2 In 1959, a law was passed requiring doctors to inform women who had just delivered a child or had an abortion about their contraceptive options. The state's health care system began to cover 70% of the cost of prescription contraceptives, acknowledging and legitimising women's need for family planning services. The coverage included mainly the pill and IUDs, while condoms were sold over the counter in pharmacies and paid for by users.Citation3 There was a six-fold rise in sales of oral contraceptives as many more women began using them, but production could not keep pace with rising demand, thereby creating a shortage.Citation4
In 1989, state socialism collapsed in Poland as a result of a failing economy, the collapse of the Soviet Union, and a decade of mounting opposition by Solidarity, the Catholic-influenced nationalist labour union. The regime's collapse led to a series of political and economic transformations. The most detrimental for reproductive health care access was the intensification of the political role of the Catholic church, which swiftly led to a ban on abortion and the institution of a Conscience Clause law, which restricted access to prescription drugs such as hormonal contraception and antenatal testing for fetal anomalies, as some doctors began to cite religious objection to providing these previously lawful medical services. The Church was also instrumental in eliminating health insurance coverage for contraception in 2002, and began to encourage physicians to invoke conscientious objection to limit contraceptive prescriptions.Citation5 Because sterilisation remains illegal, physicians who perform it clandestinely can be punished with imprisonment of up to ten years. The law on voluntary sterilisation is often interpreted so restrictively that even women with serious contraindications to pregnancy are denied access to sterilisation.Citation2 The Catholic church considers sterilisation a sin and any effort to decriminalise it would undoubtedly be opposed.
The early post-socialist period also ushered in economic transformations that proved to be further detrimental to women's health. As the upper echelons of Solidarity took power, headed by Lech Wałęsa, the new government embraced neoliberal economic principles that gave market forces primacy over economic and social policy and led to social welfare cuts, privatisation, decentralisation and deregulation.Citation6 Maternity leave was cut from almost two years to less than four months, most childcare facilities were privatised and family cash benefits were reduced. Comparative studies of social services in Eastern Europe show that Poland suffered among the harshest reductions in family and maternity benefits.Citation7 Cuts in health care were also substantial: subsidies of medicines dwindled from 100% before 1989 to 35% in 2004, the lowest in the European Union (EU), and many basic services were removed from universal coverage.Citation8 According to the 2006 World Health Report, Polish government expenditure on health care was 9.8% of total government expenditure, the second lowest in the EU after Latvia. Private health insurance plans are only beginning to be established; thus, most people rely on public health care and private care is paid for by users. A 2009 report shows that Poland's health continues to rank near the bottom of EU nations in health care expenditure.Citation9
Concurrent with cuts in health spending, Poland has been moving toward a privatisation of the health system. During state socialism, Poland adopted the Semashko model, named after Nikolai Semashko, a Soviet physician and the Commissar of Public Health who devised the communist state-funded and centralised health care system. The Semashko model aimed to guarantee access to public health care for the entire population, and was adopted in several Soviet bloc nations. While Poland's health care facilities were managed by state employees, a limited private sector emerged in the 1970s when economic difficulties prevented further state allocations for health; the state became receptive to allowing limited private providers to deal with the growing queues for public health services.
Since 1989 the state has gradually been decentralising the system, and privatisation has intensified. Health care is divided into public and private, with a grey sphere of informal payments. Formally, there is a free public health care system via the National Health Fund (Narodowy Fundusz Zdrowia), but due to cuts in government expenditure and shortage of providers, who have emigrated in pursuit of better wages,Citation10 public facilities are overcrowded, with long waiting lists, scarce medical supplies and out-of-date technology. Care is often perceived to be of lesser quality than if one pays in a private clinic.Citation11 Poles cite excessively long queues as the main reason for unmet medical needs, three times more than the average EU citizen.Citation12 Yet, a national opinion survey indicated that 59% of Poles rely heavily on the public system and never pursue health care privately, citing lack of need and high expense of private care.Citation13
Although the majority of the population still attend public facilities, hospitals are becoming privatised to varying degrees, including privatisation of management through contracts with outside companies, specific services sub-contracted to private providers, increased out-of-pocket payments for patients, and full privatization whereby the entire facility becomes private.Citation9,14 In 1999, 44% of individuals who pursued public health services in facilities under the new health care privatisation schemes paid fees out of pocket.Citation15 Private physicians have been vigorously promoting their practices, due primarily to meagre incomes within the public system; as of 2004, a state physician's salary was lower than the average monthly income of 2323 zł (516 €).Citation16Citation17 Nurses are also underpaid, and periodically launch major strikes protesting low pay and cuts in health care expenditures, including hunger strikes, road blocks and camping in tent cities in front of government buildings, but the government has refused to make any concessions. These conditions have encouraged Polish health professionals to emigrate, especially to the UK and Ireland. In the year after Poland's entry into the EU, approximately 4,000 Polish physicians applied for registration to work in the UK's National Health Service.Citation10 This exodus has depleted Poland's health system, leaving only 203 doctors per 100,000 population, a significantly lower number than in neighbouring nations, e.g. 356 doctors to 100,000 in Czech Republic, 313 in Slovakia, and 348 in Germany.Citation9
The impoverishment of the health system facilitates corruption, which fuels unequal access to care. Polish physicians operate a vigorous system of informal cash payments (kopertówki) that allow patients to skip waiting lists and get better quality care. Although informal payments were not uncommon during state socialism either, bribery has intensified so greatly since 1989 that the practice is now virtually mandatory, making many services more readily available to the wealthy than the poor.Citation11,18,19 The common perception is that the quality of services depends on offering bribes, of which 70% are monetary; the rest are gifts such as alcohol or chocolates. These have been especially common for surgical procedures in obstetric care, such as caesarean sections, and during labour and delivery.Citation20 Thus, while these procedures are theoretically fully state subsidised in hospitals, in reality a bribe is expected for decent quality of care. Physicians holding public hospital management posts have also been benefiting financially by treating their private patients on site and charging them higher fees for services, which many state hospitals allow. Thus, public health facilities are sources of capital for doctors' private enterprises.Citation11Citation21
The consequence of this corruption has been the privileging of wealthier patients in accessing medical care. With higher unemployment and lower incomes among women, the question arises whether this situation disproportionately affects women's access to reproductive health care.
Methods and participants
This paper draws on primary data collected from May to August 2007 in Gdańsk and the contiguous towns of Gdynia and Sopot, the second largest urban area in Poland after Warsaw, with a population of over one million, located on the Baltic coast. Gdańsk and its vicinity were selected because the median income falls closest to the average income of the 13 main urban centres in Poland and its economic base is diverse.
The study examined three aspects of reproductive health: contraceptive use and knowledge, knowledge and perception of clandestine abortion services, and childbearing decisions underlying the low birthrate. Although not pursued directly, the issue of access to family planning in light of post-socialist reforms also crystalised in the course of data collection. I conducted a comprehensive literature review in scholarly journals and books, and reports generated by the WHO, the Polish state, and the UN. I carried out a quantitative survey among 418 women aged 18–40 attending four major health care facilities and qualitative interviews with a sub-sample of 55 women who were recruited randomly at scheduled visits at each of the four clinics, during which all survey participants were approached to invite them to be interviewed.
Data were collected face-to-face. The quantitative interview had 168 questions and the qualitative interview 24 items. Interviews took 30–60 minutes. No identifying data were collected and all interviewees were assured of confidentiality. The women were recruited in four multi-specialty medical facilities that provided general and specialised medical services and served as the portal of entry for medical care for the population at large. These clinics accepted patients with public or private health care coverage, as well as those paying out of pocket. The research sites were selected from a list of 19 regional clinics by contacting every fourth clinic on the list. Interview procedures were the same across the four facilities. Respondents were recruited from among patients who were waiting for an appointment in the main waiting room at each facility. After having been identified visually as age-eligible, they were handed a written description of the project inviting them to participate. All interviews were conducted in a separate, private room in the facility, usually on the same day as their appointment. Interviews were in Polish, and were transcribed and translated into English. Women received a small remuneration of 20 zł (approx. 5€) for their time. The quantitative data were analysed using SPSS software and the qualitative transcripts analysed using ATLAS ti software. Each respondent's text was coded by thematic categories, from which predominant themes and sub-themes were identified.
The women were from diverse socioeconomic backgrounds, with the largest number earning 600–1200 zł per month (€ 150–300). Their mean age was 29, 45% were unmarried, mean parity was 0.92, 65% held part-time employment, and 90% identified as Catholic. This study has limitations. Overall, the respondents were more educated than the national average, which reflects the urban nature of the sample. Although the clinics selected for this study are typical of urban health centres across Poland, they are not a random national sample; therefore, the results are not generalisable.
Restrictions on access to modern contraceptives
The Polish Constitution of 1997 guarantees everyone the right to protection of their health, and guarantees citizens, regardless of their material situation, equal access to health care services financed through public means.Citation22 However, a loophole allows the state to selectively exclude services from the publicly-funded “health benefit basket”, and recent reforms have limited access based on ability to pay. Religious rhetoric in the 1990s not only led to the abortion ban in 1993; the promotion of natural family planning fueled the withdrawal in 1999 of five types of birth control pills from the list of subsidised medicines, deeming their use as elective rather than medicinal, and making it difficult for many women to continue using them.Citation23 Intrauterine devices (IUDs) and emergency contraception are also no longer subsidised. Only four drugs with contraceptive functions remain on the list of subsidised drugs, strictly due to their utility for treatment of certain endocrine or other conditions, such as acne or endometriosis, and prescriptions for them are limited to patients with such diagnoses.Citation24
In 2007, these changes were reflected in the narratives of the women I interviewed, who found it difficult to access many essential services that were previously state subsidised, in particular contraceptives and antenatal tests for fetal anomalies. Of the 418 women surveyed, 56% had used a modern contraceptive in the previous year (pill 13%, IUD 8%, condoms 35%), and it emerged that the type of contraceptive used by almost one in five of them was affected by lack of state subsidy. When asked in the survey why they had chosen a particular contraceptive method during the previous year, 70 of the 418 women (17%) said it was because it was less expensive; of whom 43 women used condoms, 20 used coitus interruptus, and 16 used periodic abstinence (kalendarzyk) (some women used more than one of these methods). Four were not using any method. Others surveyed cited non-economic reasons, including doctor's or friend's recommendation, ease of use, and low side effects.
Non-prescription methods are generally less effective than higher cost oral contraceptives or IUDs. Indeed, the dominant perspective among the women in the qualitative interviews was that hormonal contraceptives constituted one of the most effective and easy methods of preventing pregnancy and were therefore desirable. Among the 54 women of the 418 surveyed (13%) who had used hormonal contraceptives during the previous year, eight had discontinued their use because of the cost. During the qualitative interviews, it also emerged that some women had not considered the pill as a viable option due to cost.
“I've never used the pill, but I'd like to try. But I can't buy them because they're not covered by state health insurance.” (No.18, 32 years old, custodian)
“For a while I used the hormonal patch. They were 50 zł a month so eventually I just stopped and never brought it up with the doctor again. I think the patch is great if you can afford it.” (No.51, 39 years old, physical therapist)
“It's expensive to use pills if you have only occasional sex. Condoms are better for occasional partners…” (No.10, 34 years old, unemployed)
The costs of obtaining contraception in Poland mount further due to refusals by some doctors to prescribe contraceptives, citing conscientious objection, thereby forcing women to accrue charges from further doctors until they find a sympathetic one willing to offer the service.Citation5 This can be especially burdensome and costly for women in rural areas where there may be only one physician. Some physicians restrict prescriptions for the pill to a one-month supply, forcing women to pay for repeated visits.Citation25 Several women in this study reported having to undergo additional “cytology” tests, two to four times a year, further raising the cost:
“I used the pill some time ago but I just couldn't keep going to see the doctor for check-ups and the lab tests every three months to get the refills so I gave up. It was too much money and trouble.” (No.16, 28 years old, receptionist)
Pronatalist population policy
Advocacy efforts in recent years by reproductive health activists and politicians in favour of expanding subsidies for contraceptives have often been rebuffed by the state with demographic arguments about falling birth rates. Indeed, Poland's total fertility rate plummeted from 2.1 in 1989 to 1.27 in 2008, though it had been at or above replacement level since World War II. Fertility reached its lowest point, 1.22, in 2002 and has increased marginally since.Citation26Citation27 The demographic crisis, as it is popularly referred to, since the fall of state socialism is perceived by the state as detrimental to economic growth. In 1999 the state implemented a pronatalist Profamily Programme that has provided few material benefits for families. The objective was to stop fertility decline and create a high rate of economic development, to help to create more jobs, and therefore facilitate an increase in fertility.Citation28 Restrictions on family planning services fit into the conservative rhetoric of promoting births. In reality, the Profamily Programme has failed to increase the birth rate or counter the economic difficulties resulting from the severe reductions in welfare and health care provision. In fact, the economic cutbacks combined with discrimination by employers against pregnant women and women with small children have been decisive in women's decisions to postpone or forego childbearing, resulting in what demographers refer to as the “lowest low” fertility, i.e. below 1.5.Citation29
Contraceptive prevalence has risen substantially in Poland since 1991, when according to national survey data, modern contraceptives were used by only 19% of women nationally.Citation30 The persistently low birth rate, high abortion rate and substantial increase in contraceptive use, in spite of access problems and the high cost of obtaining contraception, indicate that family planning is and is likely to remain a high priority for Polish women, including among many who identify as Catholic, who are using modern contraceptives despite the church's prohibition, citing pragmatic reasons for needing to control fertility – both financial difficulties and wanting to care for existing children better.Citation31
“Privatisation” of abortion services
Abortion services have been completely privatized since the ban on abortion in 1993. Physicians who performed abortions before 1993 began to offer the service clandestinely afterwards for a high fee. This ban represents a legal form of “privatisation”, which led to the migration of patients and doctors to the unregulated private sector. The current law criminalises abortion under all but three circumstances: when the woman's life or health is in danger, when an antenatal test shows a serious, incurable deformity of the fetus which is threatening to its life, and when pregnancy is the result of rape or incest which has been reported to the police and the pregnancy is less than 12 weeks. Since 1956 only 3% of all abortions had been performed for these reasons. Hence, 97% of abortions were likely to be driven underground.Citation32Citation33 Even legally permissible abortions are difficult to obtain because conscientious objection is frequently declared by the directors of hospitals on behalf on the entire staff.Citation5
In addition, the abortion ban has reduced access to legal abortion in public facilities because doctors prefer to collect a high fee and avoid public visibility.Citation34 Thus, women who are eligible for publically funded procedures find it easier and faster to obtain the care clandestinely. A recent case at the European Court of Human Rights, involved Alicja Tysiac, who was denied a legal abortion, carried the pregnancy to term and became legally blind as a result. Poland was judged to have failed to create mechanisms to ensure women's right to an abortion within the current law.Citation35
During state socialism abortions were also performed privately but as doctors were not obliged to report them, data are lacking. Early restrictions on abortion began in the 1980s with the rise of Solidarity, and women who could afford to do so increasingly began to pursue abortions privately. This paved the way for the “white coat” abortion underground after 1993, mainly of experienced gynaecologists.Citation5 While the Polish Federation for Women and Family Planning estimates clandestine abortions at 80,000–200,000 per year, the government acknowledges only legal abortions, less than 200 per year in recent years. Moreover, abortion tourism for Polish women is thought to be flourishing,Citation24 though few data exist.
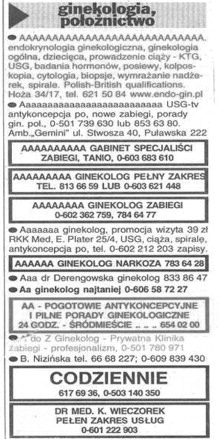
Clandestine abortion is available for about 1,000–3,000 zł and is advertised in newspapers, including the largest Polish daily Gazeta Wyborcza, but also smaller local publications such as Dziennik Bałtycki in the Gdańsk area. The advertisements are short and often contain only a mobile phone number and key phrases that were understood among the women in this study such as: “all services provided”, “vacuum”, “anaesthesia”, “menstruation induced”, “complex procedures”, and “discreet”. One can call to fix the price and location, and schedule the procedure for the same or next day. Nearly all the women I spoke to had extensive knowledge about how this abortion underground functions, including where to look for a provider, the cost and how it varies between different geographic locations, and the way clinics typically look. Almost half of them personally knew of someone who had obtained an abortion clandestinely and many thought the service was relatively accessible.
Abortion adverts, Gazeta Wyborcza, June 2002
“Abortions can be costly but you can certainly find them all over the newspapers… You just pick one and call.” (No.5, 32 years old, manager)
“A number of my friends had abortions in private offices. The offices are usually quite beautiful and it costs about 2000 zł… If I needed a doctor I would go to my gynaecologist and ask her first. She won't necessarily be the one who'll do it but she can refer me. All abortions are done locally.” (No.12, 32 years old, secretary)
“I went to [my doctor] who had prescribed my [birth control] pills hoping she'd give me a referral, but she told me to pick a doctor from the newspaper. So I got the paper and started calling. I called two adverts that said “vacuum method.” One doctor was in Katowice and wanted 1200 and the other was in Krakow and wanted 1400, both could see me that day. I came up with 1000 but had to borrow the rest from two friends… I chose the Krakow clinic since he let me bring a friend… The clinic told me I was to meet their driver at a specific location, and to hold an empty plastic shopping bag in my hand. A man pulled up in an old car and told us to get in. We got in, frightened, but we got in. The situation felt anxious and secretive. He tried to be pleasant as he drove us outside the city to the doctor's private house. The sign at the gate said: ‘Doctor of Gynaecology’, which calmed me a bit. The office was very elegant… and the older woman anaesthetist was quite friendly. She said the procedure was easy, like pulling a tooth. She came from her hospital just for this… I never learned the doctors' names. When I woke up from the anaesthesia, he wanted my phone number in case of complications and told me to return for a check up, but later I decided I didn't need to go back. My friend and I were dropped off on the same street corner, and from there I took the bus home. I was glad to have it behind me.” (No. 31, 22 years old, student)
Nurses strike, Warsaw, 21 June 2007

The medical community as a whole has been reluctant to advocate for liberalisation of the law, leaving advocacy entirely to local and international NGOs (Personal communication, Wanda Nowicka, President, Federation for Women and Family Planning, March, 2010).
Antenatal and delivery care, cervical cancer, and assisted reproduction
Antenatal tests and perinatal care have also been curtailed since 1989. Antenatal tests are no longer covered by the state but accrue an out-of-pocket expense unless explicitly recommended by a physician. Since severe fetal abnormalities that have been demonstrated in an antenatal test constitute grounds for a lawful abortion, the church opposes antenatal testing. In 1999, the Catholic lobby successfully supported a bill that imposed criminal penalties of two years in prison on doctors “for damaging the body of a fetus or causing damage to health, or threatening its life” as a result of an antenatal test.Citation36 Consequently, doctors are increasingly reluctant to refer women, fearing repercussions if a woman miscarries, even if she has accepted the risk. Some physicians refuse to make referrals on the basis of conscience. In terms of perinatal health care, Minister of Health Ewa Kopacz recently approved the continued exclusion from state coverage of anaesthesia during childbirth. Epidurals are thus placed alongside aromatherapy as extras during deliveries. The Federation for Women and Family Planning argued in an open letter, to no avail, that this excludes many women from otherwise available advances in health care and constitutes a patient's rights and human rights violation.Citation37
In vitro fertilisation (IVF) has been entirely unregulated in Poland and a political debate has been raging for years over whether or not IVF should be state subsidized and regulated. Thus far private clinics have been providing infertility services to both domestic and foreign patients. State regulation of IVF treatment has been paralysed by opposition from the Catholic church, which objects to assisted reproduction in principle and public funding of the service in particular. Consequently, IVF services are currently private, unregulated and unsubsidised.
Low spending on health care and the migration of providers to private practices also translate into discouragingly long waits for a gynaecological appointment in a state clinic, ranging in 2007 from 9 to 66 days, and low utilisation of care in some parts of the country.Citation26 As private hospitals are not required by the state to provide a full range of services, gynaecological care is not always included. Of concern is the fact that Poland has one of the highest rates of cervical cancer and the highest mortality rate in the EU. Less than 20% of cervical cancers in Poland are detected in the premalignant stage. Despite the epidemic levels of cervical cancer in Poland, the state failed to dedicate resources to population-based screening and instead implemented opportunistic screening in 2007, which reached only 24% of targeted women. In 2008 the state began to expanded screening but the challenges of promoting the service remain.Citation38
Discussion
Non-governmental sector initiatives to stop cuts in reproductive health services, mainly spearheaded by the Polish Federation for Women and Family Planning, have been vigorously undertaken along the way but their efforts are opposed by the decisive influence of the Catholic church in Polish politics and the neoliberal aversion to public funding of services.
In the late 1990s, women reported a greater number of chronic diseases than men, and an overall self-perceived worsening of health as compared to men in all age groups and in rural as well as urban areas.Citation39Citation40 A 2009 Eurostat report shows that far more Polish women perceive their health as “very bad” or “bad” compared to men.Citation12 The narratives of the women in this study show that while many more women use modern contraceptive methods, the high cost of prescription contraceptives due to the loss of state subsidies for family planning plays a significant role in their ability to access effective contraception. Moreover, criminalisation of abortion has resulted in privatisation of this service, which is now only accessible for a high fee and in clandestine settings.
This is troubling in light of international standards of reproductive health care. While the church in Poland opposes subsidies for contraceptives, the World Health Organization includes contraceptives on its Essential Medicines List as satisfying the “priority health care needs of the population” that should be available at “a price the individual and the community can afford”.Citation41 A decline in contraceptive access may contribute to a rise in abortions.Citation42Citation43 Even if most abortions in Poland are relatively safe (data are lacking to prove this either way), in other legally restricted settings the poor often turn to less skilled practitioners or self-induce, thereby exposing themselves to greater health risks.Citation44
The significance of these restrictions should also be understood in the context of women's economic position after 1989. State socialism facilitated women's education and by 1989 Polish women were better educated than men; more women graduated in every educational category, except vocational. Furthermore, by 1989, 80% of Polish women were employed and many held high-level jobs, especially in health care, where the majority of physicians were women.Citation45 Better education and significant employment history should have benefited Polish women in the new market economy. Yet, women across the post-socialist region find themselves in a losing position as new stratifications emerge along gender and class lines. According to the World Bank: “the transition from planned to market economy has witnessed one of the biggest and fastest increases in inequality ever recorded”.Citation46 Poland is experiencing a “feminization of poverty” as women are fast becoming the new economic “underclass”: they have twice the likelihood of falling below the poverty line as men, and constitute the majority of the unemployed, as their employment has declined from 80% to 65% since 1989.Citation47 Compounding the situation are reductions in maternity care, childcare and social services across the region.Citation48
Rural women are especially affected. Many are reverting to traditional strategies of relying on kin networks for resources, intensifying home production of clothing and food, and generally surviving on the informal economic exchanges so prevalent during state socialism which, ironically, are returning as key coping mechanisms.Citation49 Rural women are also less able to circumvent the ban on abortion due to lower incomes and fewer clandestine providers in their areas.
Furthermore, discriminatory practices by employers against pregnant women and women with small children have been critical in Polish women's decisions to postpone childbearing.Citation31 The low fertility rate is highly significant as it suggests that despite the legal and financial barriers, controlling fertility is of high priority for Polish women. Yet, declining fertility is used as fodder for the very anti-family planning rhetoric responsible for marginalising reproductive health services as undeserving of state subsidies.
Conclusions
This study calls attention to the need to include comprehensive family planning services in publicly funded health care, and to liberalise the restrictive abortion law in Poland. It identifies the need to regulate privatised services and increase access to maternity and gynaecological care. Higher wages for state health providers and better public health provision would curb informal payments, thereby reducing costs. Current health care policies stigmatise women's choices and deny the legitimacy of their health needs and reproductive and sexual autonomy. Poland's policies stand counter to established international standards of reproductive health care. The state should heed the recommendations of Polish reproductive health NGOs in reforming policies. Although Poland is a signatory to the European Union's Charter of Fundamental Rights and the Convention on Human Rights, the government's anti-women policies strike at the core of gender equity and reproductive and social justice.
Acknowledgements
This research was generously supported by the Charlotte Ellertson Postdoctoral Fellowship, Columbia University. I am also grateful to the many women who shared their experiences and perspectives, and clinic directors and research assistants in Gdańsk and Sopot for their interest and work in facilitating this project.
References
- M Fuszara. Legal regulation of abortion in Poland. Signs. 117: 1991
- M Rutkiewicz. Towards a human rights-based contraceptive policy; a critique of the anti-sterilization law in Poland. European Journal of Health Law. 8: 2001; 225–242.
- P Mazur. Contraception and abortion in Poland. Family Planning Perspectives. 13(4): 1981; 196.
- M Okólski. Abortion and contraception in Poland. Studies in Family Planning. 14(11): 1983; 269.
- J Mishtal. Matters of conscience: the politics of reproductive health and rights in Poland. Medical Anthropology Quarterly. 23(2): 2009; 173–176.
- D Ost. The defeat of solidarity: anger and politics in postcommunist Europe. 2005; Cornell University Press: Ithaca.
- E Fodor, C Glass, J Kawachi. Family policies and gender in Hungary, Poland, and Romania. Communist and Post-Communist Studies. 35(4): 2002; 477–483.
- Screwing the brand names. The Economist. 16 November. 2004
- World Health Organization European Region. European Health Report, 2009. Figure 3.4 and Table 6. At: <www.euro.who.int/_data/assets/pdf_file/0009/82386/E93103.pdf>. Accessed 10 August 2010
- D McLaughlin, D Smith. Doctors go west in Polish brain drain. The Observer. 15: 2005; 21.
- B Leven. Corruption and reforms: a case of Poland's medical sector. Communist and Post-Communist Studies. 38: 2005; 447–455.
- K Baert, B De Norre. Perception of health and access to health care in the EU-25 in 2007. Eurostat Statistics in Focus. 24: 2009
- M Sawińska, J Adelt. Wybieramy leczenie za darmo (We choose free health care). 2004; Ośrodek Badania Opinii Publicznej (Center for Public Opinion Research): Warsaw.
- H Maarse. The privatization of health care in Europe: an eight-country analysis. Journal of Health Politics, Policy and Law. 31(5): 2006; 981–1014.
- K Tymowska. Health care under transformation in Poland. Health Policy. 56: 2001; 85–98.
- L Czupryniak, J Loba. Route of corruption in Poland's health care system. Lancet. 364(9448): 2004; 1856.
- Central Statistical Office. Praca ludnosci: wynagrodzenia; 2006. At: <www.stat.gov.pl/english/dane_spolgosp/praca_ludnosc/zatr_wyn/2006/1q/index.htm>. Accessed 17 March 2010
- M Chawla, P Berman, A Windak. Provision of ambulatory health services in Poland: a case study from Krakow. Social Science & Medicine. 58: 2004; 227–235.
- I McMenamin, V Timonen. Poland's health reform: politics, markets and informal payments. Journal of Social Policy. 31: 2002; 103–118.
- A Kubiak. Pacjeci i lekarze o korupcji w publicznej służbie zdrowia: research report. 2001; Fundacja Batorego: Warsaw.
- P Watson. Unequalizing citizenship: the politics of Poland's health care change. Sociology. 40(6): 2006; 1079–1096.
- Constitution of Poland. 4/2 1997, Article 68, point 1/2. At: <www.sejm.gov.pl/prawo/konst/polski/kon1.htm>. Accessed 19 March 2010
- J Mishtal. How the church became the state: the Catholic regime and reproductive rights and policies in Poland. J Massino, S Penn. Collected Volume on Women's Lives, Gender Relations and State Policy in Central and Eastern Europe under State Socialism. 2009; Palgrave Macmillan: New York.
- Report on Reproductive Health Supplies in ASTRA Countries. Warsaw, ASTRA - Central and Eastern European Women's Network for Sexual and Reproductive Health and Rights, 2008.
- E Zielińska, W Nowicka. Zdrowie kobiet w Polsce. Fundacja Feminoteka. Warsaw, 2009. p.10–11,19. At: <www.federa.org.pl/Informacje/Wanda%20podstona/Raport%20Zdrowie%20Kobiet%20EZ_WN%202009.pdf>. Accessed 18 March 2010
- Z Strzelecki, A Gałązka, I Kowalska. Demographic situation in Poland: 20065–20076. Report No.1. 2007; State Committee on Population: Warsaw.
- UN Population Division. Total fertility rate. At: <http://data.un.org/Data.aspx?d=PopDiv&f=variableID%3A54#PopDiv>
- Magistrate for Family Affairs. 1999; Profamily Politics of the State: Warsaw, 5–9.
- J Mishtal. Understanding low fertility in Poland: demographic consequences of postsocialist neoliberal restructuring. Demographic Research. 21(20): 2009; 599–626.
- UN Economic Commission for Europe Department of Economic and Social Affairs, Population Division. World Contraceptive Use, 2005. At: <www.un.org/esa/population/publications/contraceptive2005/2005_World_Contraceptive_files/WallChart_WCU2005.pdf>. Accessed 19 March 2010
- J Mishtal, R Dannefer. Reconciling religious identity and reproductive practices: the Church and contraception in Poland. European Journal of Contraception and Reproductive Health Care. 15(4): 2010; 232–242.
- E Johannisson, L Kovacs, BA Resch. Assessment of Research and Service Needs in Reproductive Health in Eastern Europe. 1996; Parthenon: New York.
- U Nowakowska, M Korzeniowska. Women's reproductive rights. U Nowakowska. Polish women in the 90s. 2000; Women's Rights Center: Warsaw, 219–248.
- W Nowicka, F Girard. Clear and compelling evidence: the Polish tribunal on abortion rights. Reproductive Health Matters. 10(19): 2002; 22–30.
- World Health Organization. Highlights on Health, Poland: Mortality. 2005; 1.
- W Nowicka. Struggles for and against legal abortion in Poland. B Klugman, D Budlender. Advocating for Abortion Access. 2001; Women's Health Project: Johannesburg, 232–233./242
- W Nowicka. List otwarty o bezpłatne znieczulenie farmakologiczne przy porodzie [Open letter]. Federation for Women and Family Planning. 16 February. 2010. At: <www.federa.org.pl/?page=news&newsid=951&lang=1>. Accessed 15 March 2010
- A Anttila, G Ronco. Description of the national situation of cervical cancer screening in the member states of the European Union. European Journal of Cancer. 45: 2009; 2685–2708.
- M Szaflarski. Gender, self-reported health, and health related lifestyles in Poland. Health Care for Women International. 22: 2001; 210.
- W Wróblewska. Women's health status in Poland in the transition to a market economy. Social Science and Medicine. 54: 2002; 707–726.
- World Health Organization. Essential Medicines. 2008. At: <http://apps.who.int/medicinedocs/en/d/Js4875e/5.2.html>
- A Russell, E Sobo, M Thompson. Contraception across Cultures. 2002; Berg: Oxford.
- A Titkow. Poland. HP David. From Abortion to Contraception. 1999; Greenwood Press: Westport, 165–190.
- Alan Guttmacher Institute. Clandestine Abortion: A Latin American Reality. 1994; AGI: New York.
- Statistical Yearbook of the Republic of Poland. Warsaw: Ministry of Education, 2004;196,247,371.
- Milanovic B. Explaining the increase in inequality during the transition. Policy Research Working Paper. Washington, DC: World Bank, 1998. Report #WPS1935, Vol.1.
- H Domanski. Is the East European ‘underclass’ feminized?. Communist and Post-Communist Studies. 35(4): 2002; 393.
- J Kocourkova. Leave arrangements and childcare services in Central Europe. Community, Work and Family. 5(3): 2002; 301–318.
- F Pine. Retreat to the household? Gendered domains in postsocialist Poland. CM Hann. Postsocialism: Ideals, Ideologies and Practices in Eurasia. 2002; Routledge: New York, 95–113.