Abstract
Abstract
Violence by an intimate partner, including violence during pregnancy, is an important human rights and public health issue. This paper presents the findings from large household surveys conducted in Mbeya and Dar es Salaam, Tanzania, in 2001–2002, as part of the WHO Multi-Country Study on Women's Health and Domestic Violence against Women. Seven (n=88) and twelve per cent (n=147) of ever-partnered, ever-pregnant women in Dar es Salaam (n=1,298) and Mbeya (n=1,205), respectively, reported being physically assaulted during pregnancy by their partner. Of those experiencing partner violence during pregnancy, 38% (n=33) and 23% (n=34) reported blows to the abdomen. More than a third of women experiencing the violence in each setting reported that it started during pregnancy. In both settings, the violence was significantly associated with adverse maternal health behaviours and outcomes, including drinking during pregnancy, having had a child that died and the partner preventing or discouraging attendance for antenatal care. Factors significantly associated with higher likelihood of partner violence during pregnancy included being currently unmarried, having had children from different fathers, partner's unfaithfulness and his refusal to use contraception. While interventions on partner violence during pregnancy have been tested in antenatal services in some developed countries, effective solutions for how to intervene in low-resource settings like Tanzania are still needed.
Résumé
La violence infligée par un partenaire intime, notamment pendant la grossesse, est un grave problème des droits de l'homme et de la santé publique. Cet article présente les conclusions de vastes enquêtes auprès des ménages réalisées à Mbeya et Dar es Salaam, Tanzanie, en 2001–2002, dans le cadre de l'étude multipays de l'OMS sur la santé des femmes et la violence domestique à l'égard des femmes. Parmi les femmes ayant déjà eu un partenaire et ayant déjà été enceinte, 7% (n=88) et 12% (n=147) respectivement à Dar es Salaam (n=1298) et Mbeya (n=1205) ont indiqué avoir été agressées pendant leur grossesse par leur partenaire, dont 38% (n=33) et 23% (n=34) avec des coups à l'abdomen. Plus d'un tiers des femmes brutalisées dans chaque ville ont indiqué que les mauvais traitements avaient commencé pendant la grossesse. Dans les deux villes, les violences étaient nettement associées avec des comportements et des issues préjudiciables pour la santé maternelle, notamment la consommation d'alcool pendant la grossesse, le décès d'un enfant et des mesures de la part du partenaire pour empêcher ou décourager la future mère de subir des examens prénatals. Les facteurs associés avec une plus forte probabilité de violence du partenaire pendant la grossesse comprennent le fait de ne pas être actuellement mariée, d'avoir eu des enfants de différents pères, l'infidélité du partenaire et son refus d'utiliser la contraception. Les interventions sur la violence du partenaire pendant la grossesse ont été testées dans les services prénatals de pays développés, mais des solutions efficaces font encore défaut pour intervenir dans des environnements à faibles ressources comme la Tanzanie.
Resumen
La violencia por pareja íntima, incluida la violencia durante el embarazo, es un asunto importante de derechos humanos y salud pública. En este artículo se presentan los resultados de amplias encuestas domiciliarias realizadas en Mbeya y Dar es Salaam, en Tanzania, en 2001 y 2002, como parte del estudio de la OMS realizado en múltiples países sobre la salud de las mujeres y la violencia doméstica contra las mujeres. El 7% (n=88) y el 12% (n=147) de las mujeres que alguna vez tuvieron una pareja o alguna vez estuvieron embarazadas en Dar es Salaam (n=1,298) y Mbeya (n=1,205), respectivamente, declararon haber sido agredidas físicamente por su pareja durante el embarazo. De las que sufrieron violencia por su pareja durante el embarazo, el 38% (n=33) y el 23% (n=34) declararon haber recibido golpes al abdomen. Más de una tercera parte de las mujeres que sufrieron violencia en cada entorno relataron que comenzó durante el embarazo. En ambos entornos, la violencia estaba asociada significativamente con comportamientos y resultados adversos a la salud materna, como beber alcohol durante el embarazo, tener un hijo que falleció y que la pareja impidiera o no fomentara su atención antenatal. Los factores asociados significativamente con mayor probabilidad de violencia por la pareja durante el embarazo fueron: ser soltera, haber tenido hijos de diferentes padres, la infidelidad de la pareja y su negativa a utilizar anticonceptivos. Aunque en algunos países desarrollados se han probado intervenciones para eliminar la violencia por pareja durante el embarazo en los servicios de atención antenatal, aún se necesitan soluciones eficaces sobre cómo intervenir en lugares con escasos recursos, como Tanzania.
Violence by an intimate partner is one of the most common forms of violence against women, and is increasingly being recognised as an issue of significant social, public health and human rights concern.Citation1 Global research is starting to illustrate that violence may occur during pregnancy – with multi-country research suggesting that 1–28% of ever-pregnant women have experienced physical violence by a partner during pregnancy.Citation2 There is also evidence that this violence may have substantial impacts on maternal and infant health, including being associated with substance abuse during pregnancy, delays in seeking antenatal care, miscarriage and preterm delivery, and low birthweight.Citation3Citation4
Few population-based studies have been conducted on partner violence in Tanzania. A 2005 cross-sectional study in Moshi reported a lifetime rate of physical and sexual partner violence of 26%, with a prevalence of 21% within the last year.Citation5 Unfortunately, it did not investigate violence during pregnancy. The WHO multi-country study in Tanzania, on which this paper is based, showed lifetime prevalence rates of physical and/or sexual partner violence of 41% in Dar es Salaam and 56% in Mbeya, and prevalence rates of 22% and 29% within the last year, respectively.Citation6 The aim of this paper is to further analyse the WHO multi-country study data to investigate the magnitude and patterns of violence during pregnancy in two settings in Tanzania, and to explore the association between violence during pregnancy and maternal health outcomes and potential risk and protective factors for the onset of violence during pregnancy.
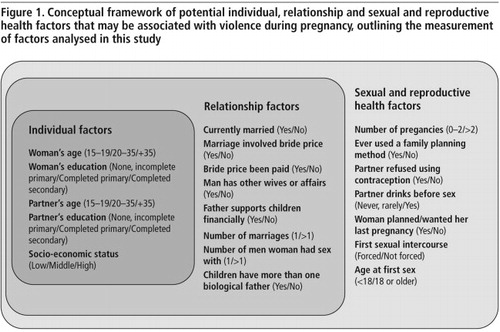
Conceptual framework for risk and protective factor analysis
Prior to the analysis, a conceptual framework, that could be used to map out the potential risk and protective factors associated with violence during pregnancy was developed, drawing upon an ecological framework.Citation2Citation7 We adapted the conceptual framework () to incorporate both the potential factors that may be associated with partner violence regardless of women's pregnancy status, as well as factors that are more pregnancy-specific. All these factors have been found in previous studies to be associated with partner violence in sub-Saharan Africa.Citation5,8–11 Importantly, as we are analysing a cross-sectional data set, we use the term “risk and protective factors” to indicate the direction of association with violence during pregnancy rather than to imply causality.
Methods
Data and study population
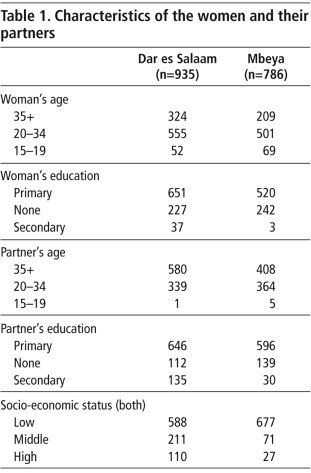
Our analyses are of cross-sectional data from the Tanzania section of the WHO Multi-Country Study on Women's Health and Domestic Violence against Women, collected from 2001 to 2002. This population-based household survey had a two-stage cluster-sampling scheme. In Dar es Salaam, all districts were included, from which 22 wards were randomly selected, but for Mbeya, only two districts, urban and rural Mbeya, were included and 22 wards were randomly selected. Using probability proportional to size (PPS) of the wards (in each site) ten cell units were then selected randomly. In each of them, households were enumerated, mapped and then randomly chosen. To ensure the safety and confidentiality of respondents, only one woman of reproductive age (15–49) was randomly selected per household to be interviewed. All interviews took place in complete privacy except for infants younger than two years. The survey used female interviewers and supervisors who were trained using a standardised three-week training course. All interviews were conducted in either Swahili or English. The translation to Swahili was adapted and corrected during the interviewer training and piloting. Information about available local services was provided to all respondents. In both sites the household and individual level response rates were very high (almost 100% in both sites at the household level, and 96% and 97% in Dar es Salaam and Mbeya, respectively, at the individual level).Citation2 The sample characteristics are described in Table 1.
The study followed the WHO ethical and safety recommendations for research on domestic violence against women.Citation12 It received ethical approval from WHO Secretariat Committee for Research in Human Subjects and the research and publications committee of the Muhimbili University College of Health and Allied Sciences, and community assent through regional and district directors and ward executive offices in Tanzania.
Violence during pregnancy throughout the paper refers to physical violence by the woman's partner during pregnancy.
Measures
A woman was categorised as having experienced violence during pregnancy if she answered yes to the question “Was there ever a time when you were beaten or physically assaulted by (any of) your partner(s) whilst you were pregnant?”. As women are commonly stigmatised and blamed for the abuse they experience, and since partner violence is considered to be a private issue, rates of violence during pregnancy are likely to be under-reported in this study. However, the careful pre-testing of the study questionnaire and the intensive interviewer training should have helped reduce this bias.Citation2
Women who stated they experienced violence during pregnancy were compared to women who said they had never experienced partner violence in their life. We excluded women who experienced violence outside pregnancy from the multivariate analyses since their risk factors are likely to be similar to those of women who experienced violence during pregnancy. With the further restriction of the sample to ever-partnered and ever-pregnant women, the analyses presented in this paper are based on 935 women from Dar es Salaam and 786 women from Mbeya. The restriction to ever-partnered women captures all women who were ever married to, ever lived with or were currently with a regular male sexual partner.
A range of reported maternal health outcomes were considered, namely: history of miscarriage, antenatal and post-natal care seeking in the last pregnancy, partner's encouragement to seek antenatal care in the last pregnancy, whether women drank alcohol during the last pregnancy, birthweight of the last child, and whether they had had a child who died. In the survey some of the maternal health outcomes considered relate only to women's last pregnancy if they were pregnant in the last five years, while the question on violence during pregnancy captures any pregnancy. This is not ideal, and is likely to result in our analysis finding weaker relationships than may actually exist.
Statistical analysis
All analyses were conducted using STATA version 11, taking the cluster sampling design into account. The association between violence during pregnancy and women's and their partner's individual, relationship and sexual and reproductive health-related factors were estimated using adjusted odds ratios of violence during pregnancy with 95% confidence intervals and the Pearson chi-square test. Odds ratios were adjusted for women's age, education and socio-economic status. While these three factors are likely to be potential risk and protective factors for physical violence by a partner during pregnancy itself, they are also likely to be associated with other possible risk and protective factors examined in this study, such as number of pregnancies, pregnancy planning or age at first sex. Data were missing for less than 5% of respondents for most variables, and women with missing data were excluded from analyses with that variable.
Findings
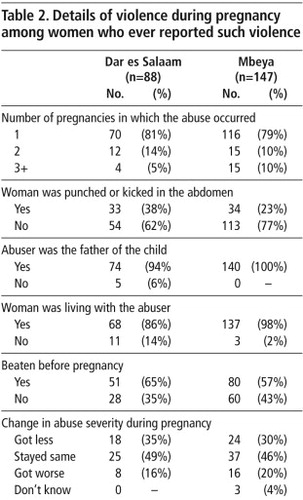
In total, 7% (n=88) of women in Dar es Salaam and 12% (n=147) of women in Mbeya reported having experienced violence during pregnancy, with the perpetrator being the father of the child in 94% of cases in Dar es Salaam and 100% in Mbeya. Pregnancy seems to have played an important role in the onset of partner violence in some cases, with 35% (n=28) of women in Dar es Salaam and 43% (n=60) in Mbeya reporting that the violence had started during pregnancy. Among women who experienced partner violence prior to the pregnancy, nearly 50% said the violence stayed the same, for around 30% it became less severe and for 20% it had got more severe. Twenty-three per cent of women in Mbeya and 38% in Dar es Salaam reported blows to the abdomen by their partner during pregnancy (Table 2).
Women's odds of drinking during their last pregnancy were significantly increased if they had experienced violence during pregnancy (Dar es Salaam: adjusted OR 5.63; CI 2.97, 10.9; p<0.001, and Mbeya: adjusted OR 3.78; CI 2.43, 5.89; p<0.001). Violence during pregnancy was also associated with having had a child or infant that died (Dar es Salaam: adjusted OR 1.89; CI 1.14, 3.12; p<0.05, and Mbeya: adjusted OR 1.73; CI 1.12, 2.68; p<0.05).
Violence during any pregnancy was not significantly associated with ever having had a miscarriage, low birthweight of the last born child, or the uptake of antenatal and post-natal care during the last pregnancy (among woman who were pregnant in the last five years). Despite this, in both sites, women were more likely to be discouraged or stopped from seeking antenatal care in their last pregnancy by their partner if they had ever experienced violence during pregnancy (among woman who were pregnant in the last five years) (Dar es Salaam: adjusted OR 2.23; CI 1.05, 5.18; p<0.05 and Mbeya: adjusted OR 3.01; CI 1.59, 5.07; p<0.001).
Women's and men's age and socio-economic status were not associated significantly with violence during pregnancy in Dar es Salaam. Women in Mbeya who had no formal education were significantly more likely to experience violence during pregnancy than women with primary education (OR 1.87; CI 1.24, 2.82, p<0.01). Similarly, such violence was more likely if their partner's education level was lower (OR 1. 76; CI 1.14, 2.72, p<0.05).
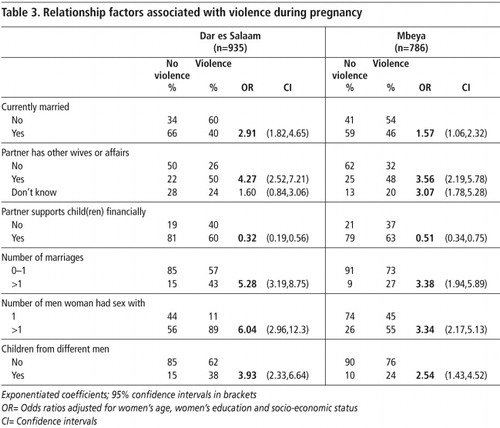
As shown in Table 3, in both sites, women who were currently unmarried, had a partner who had other wives or had extra-marital affairs or who did not support their children financially were more likely to experience violence during pregnancy. Women who had been married more than once, and those who reported having had sex with more than one man and having had children with different partners, were also significantly more likely to report violence during pregnancy in both sites. Bride price was not significantly associated with violence during pregnancy, unless it was not fully paid (Dar es Salaam: adjusted OR 3.61; CI 1.80, 7.24; p<0.001, and Mbeya: adjusted OR 1.94; CI 1.16, 3.26; p<0.05).
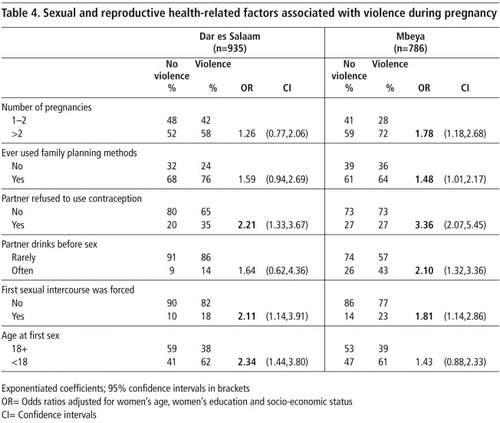
In Mbeya, violence during pregnancy was significantly associated with the woman having been pregnant more than twice, ever having used contraception and drinking by the partner before sex (Table 4). Moreover, women in Mbeya were more likely to have experienced violence during pregnancy if their last pregnancy was not planned or intended (among woman who were pregnant in the last five years) (adjusted OR 1.99; CI 1.36, 2.92; p<0.01). Partner's refusal to use contraception and forced first sexual intercourse were significantly associated in both sites, while being younger than 18 at first sex increased women's likelihood of reporting violence during pregnancy among women in Dar es Salaam.
Discussion
To the best knowledge of the authors, this is the first population-based study in a sub-Saharan African setting that has examined the prevalence, health effects and risk and protective factors of violence during pregnancy in detail.
Several limitations need to be acknowledged. First, while this study provided quantitative, factual evidence on violence during pregnancy, it lacks a qualitative component to explore the meaning of those experiences and the reasons for it from the respondents' perspectives. Second, the cross-sectional design of the study limits the extent to which we can establish causality, and distinguish risk factors from consequences of violence during pregnancy. Third, all the information is based on women's self-reports, which could have led to imprecise information and under-reporting of this and other sensitive issues. We were also not able to explore the potential role of other risk factors, such as social support or lack of it during pregnancy or having tested positive for HIV during pregnancy – issues that other research in Tanzania and elsewhere has found to be important.Citation13 Lastly, as our only measure of exposure to violence was “violence during any pregnancy”, whilst several of our health measures related to the most recent pregnancy, we would expect that the strength of the associations identified here, especially with unintended pregnancy,Citation3Citation4 may have been even stronger if we had been able to match up the exposure with the specific pregnancy.
Nevertheless, violence during pregnancy emerged in this analysis as a prevalent phenomenon with several health implications. It further showed that pregnancy influenced the occurrence of partner violence in Tanzania and was strongly associated with individual, relationship and sexual and reproductive health risk factors.
Maternity ward, Temeke General Hospital, Dar es Salaam, Tanzania, 2008

The prevalence of violence during pregnancy of 7% in Dar es Salaam and 12% in Mbeya is similar to the prevalence found in many other sub-Saharan African countries.Citation14 The maternal health outcomes and behaviours found to be associated with violence during pregnancy in this study, such as increases in having had a child or infant that died, women's drinking during pregnancy and partner's lack of encouragement to seek antenatal care, are also supported by the existing literature.Citation3,4,15 These studies also suggest that having had a child or infant that died is not only directly related to violence during pregnancy, but also indirectly since violence during pregnancy is known to be associated with preterm delivery, substance abuse and women's inability to obtain adequate nutrition and rest during pregnancy.Citation15Citation16
Importantly, our findings suggest that, for many women, pregnancy may be a trigger for partner violence, with more than a third of women who experienced violence during pregnancy in this study reporting that the violence started for the first time during pregnancy. Of these women, 38% in Dar es Salaam and 23% in Mbeya reported blows to the abdomen by their partner while pregnant.
A surprising finding is that most women only reported such violence during one of their pregnancies, despite having had more than one pregnancy. Unfortunately the original study did not ask in which of the pregnancies the violence occurred, or the reasons for this. This is an important gap. More in-depth research is needed to explore this issue further. For example, the violence may be associated with an unwanted pregnancy or suspicions over the paternity of the child.
Further research is also needed to inform the development of appropriate prevention strategies. These strategies may differ depending on the reasons for the violence and whether the violence occurred in the woman's first or a later pregnancy. Similarly, future research should investigate why, for so many women (almost a fifth in this research), violence stopped during pregnancy and whether it recommenced after the birth of the child.
Risk factors for violence during pregnancy found in this study give insights into possible interventions. The association with men's and women's education in Mbeya, for example, suggests that a primary education versus no formal education is protective against violence during pregnancy. Previous studies have found that more years of education often lead to later parenthood, while younger age at pregnancy is associated with higher risk of partner violence.Citation17 Further investigation into the particular stressors of young parents-to-be that increase their risk of partner violence is important, in order to tailor prevention efforts to them.
Previous studies have argued that women's increased economic power and men's increased absence from home in search of work in Tanzania are likely to make women less acceptant of men's traditional privileges, such as taking multiple wives or sexual partners. In turn, men might feel threatened by that and react with escalation of power, including the use of violence.Citation5 In this study, several similar factors, such as not being formally married, not having received the full payment of the bride price, partner having had other wives or affairs, and partner's unwillingness to support their children financially, were also associated with violence during pregnancy. While these issues are known to trigger violence in all stages of life, they might be of special prominence during pregnancy, when there is more pressure on partners to take responsibility and commit to the relationship and a child.Citation18 In addition, women might have higher expectations of their partners during pregnancy, to ensure a stable future for themselves and the child, with expectations that uncommitted partners might perceive as overly demanding. While being currently unmarried can also be a consequence of partner violence, as a study in rural Mwanza showed,Citation19 in some cases it might also be the stress resulting from social stigma associated with a pregnancy outside marriage that triggers violence.
Other relationship-level factors associated with physical violence by a partner during pregnancy are the woman having been married more than once, having had sex with more than one man and having had children by different biological fathers. All these issues may be related to jealousy, a prominent trigger for partner violence, in Tanzania as elsewhere.Citation20 Although one would expect jealousy to decrease during pregnancy, studies have demonstrated the opposite if partners develop doubts about paternity and due to the increased attention women give to themselves and receive from others during pregnancy.Citation18
Differences in women's risk factors for violence during pregnancy between the more developed capital city Dar es Salaam and the rural, agricultural, provincial Mbeya, with its more traditional social norms and gender roles, became most marked at the sexual and reproductive health level. Factors implying that women lacked control over contraceptive use and number of pregnancies they had, as well as their partner's drinking before sexual intercourse, were significantly associated with violence during pregnancy in Mbeya but not in Dar es Salaam.
The high prevalence of violence during pregnancy and its strong links with poor maternal health outcomes underline the importance of developing and testing appropriate interventions. Antenatal care brings women in contact, often repeatedly, with health care services, and pregnant women may be more open to discussing sensitive issues and making changes in their lives due to their desire to bring a healthy baby into the world and secure its well-being. Antenatal services have therefore been highlighted as an entry point for interventions, and several interventions have been tested in developed countries. Most of these interventions incorporated at least one 30-minute counselling session into women's antenatal care visits. The sessions were based on an empowerment protocol and designed to enhance abused women's independence and control. In them, women were given advice on safety planning, making choices and problem solving. In Hong Kong, a component of empathic understanding was also added.Citation21Citation22
Research is needed on whether these interventions would be feasible and how they would need to be adapted for low-resource settings, given the constraints on time and resources in many antenatal care services.Citation23Citation24 Research is also needed to develop and evaluate community-based interventions, targeted at both women and men, to address violence by partners against expectant mothers.
Violence during pregnancy is a serious issue that affects the lives and health of many women and their unborn children. While efforts have been made to address this issue in the developed world, solutions on how to intervene in low resource settings are urgently needed.
Acknowledgements
This study was part of the WHO Multi-Country Study on Domestic Violence against Women. We gratefully acknowledge Claudia Garcia-Moreno and the core team, the Tanzanian study team members Gideon Kwesigabo, Sherbanu Kassimu and Joe Lugalla, the women who participated in the original study and its funders. This analysis was funded via an interdisciplinary post-doctoral fellowship from the Medical and the Economic and Social Research Councils to Heidi Stöckl.
References
- C García-Moreno, H Stöckl. Protection of sexual and reproductive health rights: addressing violence against women. International Journal of Gynecology and Obstetrics. 106: 2009; 144–147.
- C García-Moreno, HA Jansen, M Ellsberg. WHO multi-country study on women's health and domestic violence against women: initial results on prevalence, health outcomes and women's responses. 2005; World Health Organization: Geneva.
- J Campbell, C Garcia-Moreno, P Sharps. Abuse during pregnancy in industrialized and developing countries. Violence against Women. 10: 2004; 770–789.
- JL Jasinski. Pregnancy and domestic violence: a review of the literature. Trauma, Violence, and Abuse. 5: 2004; 47–64.
- LA McCloskey, C Williams, U Larsen. Gender inequality and intimate partner violence among women in Moshi, Tanzania. International Family Planning Perspectives. 31: 2005; 124–130.
- C Garcia-Moreno, L Heise, HA Jansen. Violence against women. Science. 25: 2005; 1282–1283.
- L Heise. Violence against women: an integrated, ecological framework. Violence against Women. 4: 1998; 262–290.
- CA Karamagi, JK Tumwine, T Tylleskar. Intimate partner violence against women in eastern Uganda: implications for HIV prevention. BMC Public Health. 6: 2006
- KL Dunkle, RK Jewkes, HC Brown. Gender-based violence, relationship power, and risk of HIV infection in women attending antenatal clinics in South Africa. Lancet. 363: 2004; 1415–1421.
- S Vyas, C Watts. How does economic empowerment affect women's risk of intimate partner violence in low and middle income countries? A systematic review of published evidence. Journal of International Development. 21: 2009; 577–602.
- DK Kaye, F Mirembe, A Johansson. Implications of bride price on domestic violence and reproductive health in Wakiso District, Uganda. African Health Sciences. 5: 2005; 300–303.
- C Watts, L Heise, M Ellsberg. Putting Women First: Ethical and safety recommendations for research on domestic violence against women. 1999; World Health Organization: Geneva.
- S Maman, JK Mbwambo, NM Hogan. HIV-Positive Women Report More Lifetime Partner Violence: Findings From a Voluntary Counseling and Testing Clinic in Dar es Salaam, Tanzania. American Journal of Public Health. 92: 2002; 1331–1337.
- KM Devries, S Kishor, H Johnson. Intimate partner violence during pregnancy: review of prevalence data from 19 countries. Reproductive Health Matters. 18(36): 2010; 158–170.
- K Åsling-Monemi, R Peña, M Ellsberg. Violence against women increases the risk of infant and child mortality: a case–referent study in Nicaragua. Bulletin of World Health Organization. 81: 2003; 10–16.
- JC Campbell. Health consequences of intimate partner violence. Lancet. 359: 2002; 1331–1336.
- TE Moffitt, A Caspi. Findings About Partner Violence From the Dunedin Multidisciplinary Health and Development Study. 1999; US Department of Justice: Washington DC.
- K Edin, U Hogberg, D Lars. The pregnancy put the screws on: discourses of professionals working with men inclined to violence. Men and Masculinities. 11: 2009; 307–324.
- JT Boerma, M Urassa, S Nnko. Sociodemographic context of the AIDS epidemic in a rural area in Tanzania with a focus on people's mobility and marriage. Sexually Transmitted Infections. 78: 2002; 97–105.
- R Kahurananga, M Kileo. Finding a way forward: gender-based violence in Tanzania. D Brandt. Violence against Women: From Silence to Empowerment. 2003; World Vision: Monrovia, 59–74.
- A Tiwari, DYT Fong, KH Yuen. Effect of an advocacy intervention on mental health in Chinese women survivors of intimate partner violence: a randomized controlled trial. Journal of American Medical Association. 304: 2010; 536–543.
- B Parker, J McFarlane, K Soeken. Testing an intervention to prevent further abuse to pregnant women. Research in Nursing and Health. 22: 1999; 59–66.
- C Watts, S Mayhew. Reproductive Health Services and Intimate Partner Violence: Shaping a Pragmatic Response in Sub-Saharan Africa. International Family Planning Perspectives. 30: 2004; 207–213.
- M Colombini, S Mayhew, C Watts. Health-sector responses to intimate partner violence in low- and middle-income settings: a review of current models, challenges and opportunities. Bulletin of the World Health Organization. 86: 2008; 635–642.