Abstract
The private health sector in India is generally unregulated. Maharashtra is among the few states which require registration of private hospitals. This paper reports on a study of standards of care in small, private hospitals (less than 30 beds) in Maharashtra state, India, with a focus on maternity care, based on interviews with the hospitals' owners or senior staff, and observation. In the absence of reliable information on the number of private hospitals in the state, a physical listing was carried out in 11 districts and an estimate drawn up; 10% of hospitals found in each location were included in the study sample. We found poor standards of care in many cases, and few or no qualified nurses or a duty medical officer in attendance. Of the 261 hospitals visited, 146 provided maternity services yet 137 did not have a qualified midwife, and though most claimed they provided emergency care, including caesarean section, only three had a blood bank and eight had an ambulance. Government plans to promote public–private partnerships with such hospitals, including for maternity services, create concern, given our findings. The need to enforce existing regulations and collect information on health outcomes and quality of care before the state involves these hospitals further in provision of maternity care is called for.
Résumé
Le secteur privé est en général non réglementé en Inde. Maharashtra est l'un des rares États qui exigent l'agrément des hôpitaux privés. Cet article concerne une étude des normes de soins dans des petits hôpitaux privés (moins de 30 lits) dans l'État de Maharashtra, Inde, en particulier les soins obstétricaux, sur la base d'entretiens avec les propriétaires ou la direction de l'hôpital, et d'observations. En l'absence d'informations fiables sur le nombre d'hôpitaux privés dans l'État, une liste a été dressée dans 11 districts et une estimation a été établie ; 10% des hôpitaux recensés dans chaque site ont été inclus dans l'échantillon de l'étude. Dans beaucoup de cas, nous avons constaté des normes de soins médiocres, et peu ou pas d'infirmières qualifiées ni de médecin de garde présent. Des 261 hôpitaux visités, 146 assuraient des services de maternité, pourtant 137 n'avaient pas de sage-femme qualifiée, et même si la plupart affirmaient pratiquer des soins d'urgence, y compris des césariennes, trois seulement disposaient d'une banque du sang et huit d'une ambulance. Compte tenu de nos conclusions, la volonté du Gouvernement de promouvoir les partenariats publics-privés avec ces hôpitaux, notamment pour les services de maternité, est préoccupante. Il est nécessaire de faire appliquer la réglementation en vigueur et de recueillir des informations relatives aux effets sur la santé et à la qualité des soins avant que l'État n'implique davantage ces hôpitaux dans les soins obstétricaux.
Resumen
En India, el sector salud privado por lo general no es regulado. Maharashtra es uno de los pocos estados que requieren registro de hospitales privados. Este artículo informa sobre un estudio de las normas de asistencia en hospitales privados pequeños (menos de 30 camas), en el estado de Maharashtra, India, con un enfoque en la atención obstétrica, basado en entrevistas con los propietarios de los hospitales o personal de alto nivel, y en observación. En la ausencia de información fidedigna sobre el número de hospitales privados en el estado, se realizó un listado físico en 11 distritos y se calculó el número aproximado. En la muestra del estudio se incluyó el 10% de los hospitales encontrados en cada lugar. En muchos casos, se encontró calidad de atención deficiente y ninguna o pocas enfermeras calificadas o un funcionario médico de turno presente. De los 261 hospitales visitados, 146 ofrecían servicios obstétricos, pero 137 no tenían a una partera profesional calificada. Aunque la mayoría afirmaba ofrecer cuidados de emergencia, incluso cesáreas, sólo tres tenían un banco de sangre y ocho tenían ambulancia. En vista de nuestros hallazgos, los planes gubernamentales de promover alianzas entre los sectores público y privado con estos hospitales, incluso para servicios obstétricos, son preocupantes. Aún es necesario velar por el cumplimiento de los reglamentos en vigor y recopilar información sobre los resultados en salud y la calidad de la atención antes de que el estado implique aun más a estos hospitales en la prestación de servicios obstétricos.
India has witnessed a rapid expansion of the private health sector in the past two decades. Central and state governments have played a critical role in this growth, by reducing public expenditure on health, allowing the mushrooming of private medical colleges, giving concessions and subsidies to “charitable trust hospitals”Footnote* to import medical equipment and selling them land to build new facilities at nominal prices.
The vacuum created by the deterioration and even, in some places, the non-existence of public health services is being occupied by the private (mostly for-profit) health sector, resulting in an increase in the number of private hospitals from 14% of all hospitals in 1974 to 68% in 1995.Citation1 By 2004, nearly 70% of all hospitals and 40% of all hospital beds in the country were in the private sector, but importantly, over 80% of these were in urban areas.Citation2 The utilisation of public sector hospitals has concomitantly been declining in several states, including Maharashtra.Citation3Citation4
Low public health expenditure continues to characterise the Indian health system and is lower than 1% of GDP. As a consequence the out-of-pocket burden on households has been the main source of financing of health care, accounting for 80% of total health expenditure. The deterioration of public health services due to reduced investments and expenditures, is increasingly forcing people to access health care from the rapidly expanding private sector.Citation5Citation6
It is well established that the private sector is characterised by heterogeneity. At the primary level it consists of individual practitioners; at the secondary level there is enormous variation in the size of facilities, number of beds, and types and costs of services.Citation1Citation7 The secondary level consists of small and large private hospitals or nursing homes, providing both outpatient and inpatient care, the majority with less than 25–30 beds, mainly owned by doctors as sole proprietors.Citation8Citation9 Facilities range from modern, sophisticated hospitals serving the needs of the affluent classes to dilapidated rooms in slums run by semi-qualified persons. Tertiary speciality and super-speciality hospitals are mostly trust or corporate hospitals and comprise only 1–2% of the total beds in the private sector.Citation5Citation10
Despite the huge growth in investment in the private sector across all regions, there is no proper regulation or required standard of care, unlike the public health sector, which has norms for all facilities, from hospitals to dispensaries. The regulatory and institutional mechanisms for promoting accountability are weak in both public and private sectors. Several studies have commented on the variable quality of public services due to lack of adequate infrastructure, human resources and indifferent public employees.Citation5Citation11 However, the assumption that private services offer superior quality is not adequately supported by hard evidence.Citation12 Serious concerns have been raised by health researchers and activists regarding access, cost, quality and equity in some private services.Citation13Citation14 Studies over the past 20 years have demonstrated the often poor quality of care, over-hospitalisation, excess use of technology in diagnosis and treatment, over-prescription of drugs, absence of standardisation of fee structures and poor record-keeping.Citation1,13–16 Official registration of private hospitals is also low. Researchers have found through physical mapping that there are 4–10 times more private hospitals than are registered in government records.Citation13 Due to poor registration, there is no reliable information on the exact size and nature of the private sector, let alone any data on quality or cost of care. Research on private hospitals therefore poses a huge challenge as accessing data from them is difficult.
With respect to women's sexual and reproductive health, high rates of caesarean sections and hysterectomies in the private sector have been noted.Citation17Citation18 A study in Trivandrum district, Kerala, found that caesarean sections were performed three times more in private hospitals than public ones.Citation19 Moreover, since the advent of a government health insurance scheme for the poor called Aarogyasri, doctors are being reimbursed directly for certain procedures, including hysterectomy, through a network of government and private sector services. A 2009 study among 1,097 women aged 25–40 in five districts of Andhra Pradesh, conducted by the non-profit AP Mahila Samatha Society, found an increase of 20% in hysterectomy cases since July 2008. They also found that doctors had told 30% of the women that they would die if they did not have the operation.Citation20 Because irregularities had been found in claims for laparoscopies in one district; the Society is concerned that some hysterectomies may have been unnecessary.
Despite these problems, the government has been promoting public–private partnerships (PPPs) for a long time. Evidence suggests that public–private partnership initiatives in India started mainly with family planning, described in the first five-year plan (1951–56). The private partners were involved in creating awareness and demand for family planning services through community mobilisation. Few were involved in provision of contraception and abortion services. Over the years, the nature of such partnership has evolved beyond a peripheral role for non-state partners to a formal role in provision of services. The National Health Policy 2002 as well as National Rural Health Mission mandate partnerships with the private sector to increase access to services.Citation21 However, analysis in 2008 and 2009 showed that such partnerships have led to fragmentation of health programmes and that they lack institutional mechanisms for ensuring accountability and effectiveness.Citation21Citation22
In the case of the recent Chiranjeevi Scheme in Gujarat for delivery of Reproductive and Child Health services, the government provides emergency obstetric care and emergency transportation for those below the poverty line through partnership with selected private hospitals (less than 30 beds). These private hospitals have been brought in without any accreditation or review of standards for nursing homes.Citation22 A review of the scheme notes that marginalised groups in certain areas were not informed of the benefits of the scheme at all.Citation23 Moreover, a recent national hospitalisation insurance scheme for families below the poverty line, Rashtriya Swasthya Bima YojanaCitation24 (RSBY), will be implemented by reimbursements to a large number of private hospitals.
This paper reports on a study of standards of care in private hospitals with less than 30 beds in Maharashtra state, with a focus on maternity care, based on interviews with the hospitals' owners or senior staff, and observation. It questions whether public–private collaboration in the health sector in India should move forward under the present conditions.
Maharashtra: background information
The number of private hospitals in Maharashtra has grown from 68% of the total number of hospitals in 1981 to 88% in 2001. Additionally, rural Maharashtra ranks fifth in the country for the presence of private doctors in the villages, but 15th among the 28 states for the ratio of number of beds in the public sector to population.Citation25
In 2005, the public sector in the state dominated only in delivering contraceptive and immunisation services, while the private sector was the major provider of other health care services, as most primary health centres and sub-centres were not equipped to provide curative services.Citation26Citation27 In Maharashtra, the increase in utilisation of private health services grew from 84% in 1993–94 to 89% in 2003–04.Citation3Citation4 Though the private sector is widely used by all classes, a study in Mumbai clearly showed the non-availability of public health care services, which drove the poor to private hospitals, where the cost of treatment was several times higher.Citation28 Among live births in Maharashtra, out of the total deliveries recorded, 64.6% were institutional deliveries, of which 37.6% were at a private facility.Citation29
Maharashtra is one of the eight states in India with some law on registration of private hospitals. The Bombay Nursing Home Registration Act 1949Citation30 has been poorly implemented.Citation13Citation31 It was amended in 2005, and for the first time the state government, in collaboration with CEHAT (Centre for Enquiry into Health and Allied Themes), created a consultative process for formulation of rules under the Act, which involved multiple stakeholders, including health activists, researchers and representatives of medical associations.Footnote* Draft rules were discussed in various fora and submitted to the government in June 2006, but they have still not been implemented.Citation32 The reluctance of the state and resistance by a section of the medical fraternity seem to have worked together to prevent their implementation.
Methodology
The research was an exploratory study of the standards of care provided in small, private hospitals in Maharashtra. A small, private hospital for this study is defined as any hospital providing in-patient services with less than 30 beds. The Bombay Nursing Home Registration Act defines such institutions as nursing homes where “the premises are used or intended to be used for the reception of persons suffering from any sickness, injury or infirmity and the providing of treatment and nursing for them, and includes a maternity home…”.Citation32
Eleven districts were selected from five geographical regions of Maharashtra, based on various indicators of development.Footnote† From each of these districts three tehsils (blocks) were selected, depending on their level of development. As there was no information available on existing private hospitals, a physical listing was carried out in the selected tehsils to arrive at an estimate. Around 10% of hospitals from each district were selected, drawn from the city of Mumbai, rural and urban areas of developed and less developed districts of the state, giving a total sample of 267 hospitals. Six of these hospitals refused to participate; data were collected from 261. Semi-structured interviews were carried out with each hospital's In-charge and/or Duty Medical Officer/Nurse and observation of the hospital was conducted, in order to obtain data on the availability and condition mainly of the physical and structural aspects of care.
Structural aspects observed included the functional plan in the form of separate space for each activity in the hospital: inpatient facilities, operating theatre, intensive care unit, ambulance services, record maintenance services and diagnostic services, and basic infrastructural facilities such as toilets, water supply, lifts and ramps. In terms of process standards, we asked about availability of emergency services, information to patients, privacy, consent and grievance procedures. The study did not seek any information on outcomes or interview patients to understand their perceptions of the standards.
Two questionnaires and one observation schedule were used for data collection:
| • | information on existing structure and process standards; regulation and accreditation; human resources; infrastructure; admission procedures; | ||||
| • | information on emergency services, maternity services; comfort and privacy of patient; intensive care facilities; blood bank; medical records; | ||||
| • | observation to cross-check information from interviews; physical condition of the hospital; infrastructure and essential services. | ||||
In most hospitals the owner provided the information; they were also the hospital's In-charge and there was no Duty Medical Officer or nurse who could provide this information. The interviews lasted for about one hour and observation took 15–20 minutes.
Findings
We first present an overall picture of standards of care in the 261 hospitals and then focus on the 146 with maternity services.
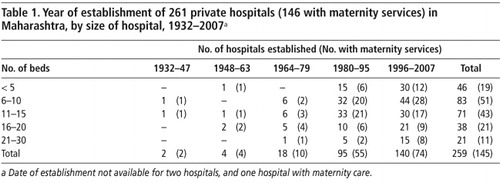
A phenomenal growth in the private health sector in Maharashtra in the past decade can be seen with the establishment of more than 140 of the 261 hospitals in this period, while another 44 were established in the past two decades. The average size was less than 15 beds (Table 1
Table 1
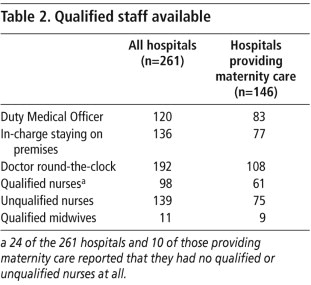
The availability of qualified staff in a hospital is an important standard of care. The Duty Medical Officer (DMO) is the resident doctor in the hospital. Only 120 of the 261 hospitals had a DMO. In one-fourth of the hospitals, there was no qualified doctor to provide round-the-clock services, i.e. neither the In-charge/owner nor the DMO was resident on the premises. Only 21 of the hospitals had allopathic DMOs; the rest were from other systems of medicine, mostly ayurvedic, even when the hospital was providing allopathic care. This is considered as cross-practice and is banned under current laws. Only 98 hospitals had qualified nurse, 139 hospitals did not have a single qualified nurse and 24 hospitals did not have a nurse at all, which is a critical indicator of standard of care (Table 2
Table 2
All the hospitals should follow a functional plan that has a separate record room, nursing station, treatment and dressing room, and casualty/emergency room. A functional plan that ensured demarcated space for essential services was found to be present only in the hospitals with more than 20 beds. However, no functional plan was followed by all the hospitals. One-third reported that they had diagnostic facilities on the premises such as x-ray, laboratory and ultrasound machines (Table 3
Table 3
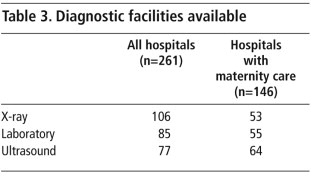
Table 4
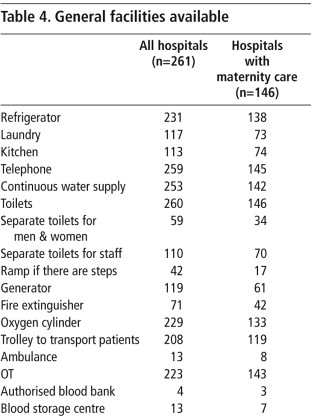
Thus, while the physical infrastructure in these hospitals, in terms of basic facilities such as electricity, ventilation and water supply appeared to be adequate, they fell short of specific services that are critical indicators of quality.
Record-keeping, grievance procedures and registration
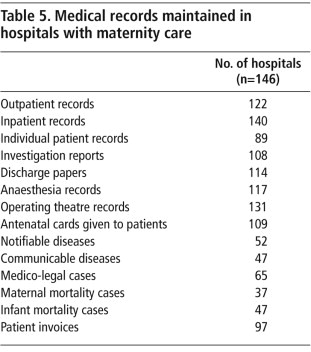
While most of the hospitals reported that they maintained medical records such as outpatient and inpatient department files, investigation reports, discharge papers, operating theatre and anaesthesia records, they fared poorly as regards maintenance of other records, such as individual patient files, notifiable and communicable diseases, medico-legal cases, and maternal and infant deaths, thus failing to measure public health outcomes.Citation33 (Table 5
Table 5
161 hospitals said they had mechanisms for handling grievances, but only 15 had a designated person to look into the grievances of patients and only 15 displayed the contact details of the concerned official. In 130 hospitals, complaints had to be registered with the hospital owner, there was no independent mechanism for handling grievances.
Only 75% of the hospitals were registered under the Bombay Nursing Home Registration Act, but the minimum requirements of registration – display of registration certificate, presence of qualified doctor and qualified nurse, and midwife in case of maternity home, registration of birth and death records – had not been attained by many of these hospitals. Thus, the terms of the Act were not being enforced and monitoring did not appear to be taking place.
Maternity services
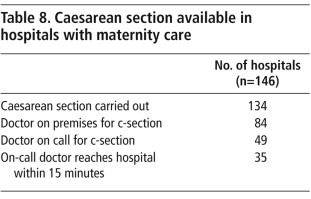
The maternity services formed a major share of the overall services provided by 146 of these hospitals. 88 of these hospitals' owners reported that they had been in private practice for more than 10 years, of whom 13 had been in private practice for more than 30 years. 126 of the these hospitals' owners were from the allopathic system of medicine, and 82 held a post-graduate degree or diploma in obstetrics & gynaecology. 96 of the 146 hospitals had 6–15 beds; the rest had 16–30. 83 of these hospitals did not have a DMO. Of those that had one, 38 had no doctor staying on the hospital premises and 61 had no qualified nurses (Table 2). Overwhelmingly, 137 of the 146 maternity hospitals did not have a qualified midwife, a basic requirement for a maternity home.
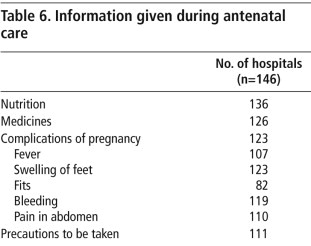
All 146 hospitals essentially provided inpatient care, and 141 reported that they provided the entire gamut of antenatal services, including iron and folic acid, calcium, blood group, measurement of weight and blood pressure, tetanus toxoid injection and routine haemoglobin, HIV and urine tests. Testing for syphilis and other STIs was not reported. Only 109 gave patients ANC cards. 143 hospitals reported that HIV testing was compulsorily for all antenatal patients. They said they sought informed consent and provided HIV counselling, but none reported any personnel designated to carry out counselling, so actual provision was uncertain. Only 55 had a laboratory where tests could be processed; most often they were sent outside. Regarding information given to pregnant women, 136 hospitals reported that information on nutrition was provided, while 123 reported that they informed women about complications of pregnancy, ranging from fever to swollen feet, fits, bleeding and abdominal pain (Table 6
Table 6
Emergency services, operating theatres and labour rooms
130 of the 146 hospitals said they provided emergency care. However, 59 of the 130 were not providing round-the-clock services. 143 of the 146 hospitals had an operating theatre, but only 121 had a labour room, of which only 89 had a delivery table with the lithotomy position. 104 of the 121 did not have a tap with a long handle, which is required in a labour room, and 67 did not have a trolley for instruments (Table 7
Table 7
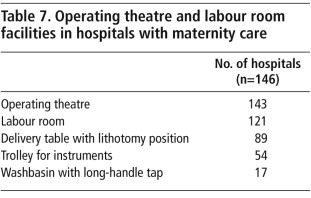
Table 8
Woman peeps through operating theatre door of Rotary Club plastic surgery clinic for impoverished people, Chalisgaon, Maharashtra, 2009

Discussion
This study assumes significance in the current scenario of health policy in India, where public-private partnerships are being promoted by the government, especially for maternity services.Citation34Citation35 There is no evidence to date on whether or how these partnerships are increasing access to services, affecting out-of-pocket payments by patients, reducing or increasing equity or improving quality of care.Citation22 Most of the proposed partnerships transfer public funds to private providers, with the aim of ensuring access for poorer patients. In the case of sexual and reproductive health services, some of the donor funds that used to be directed to public health systems are now devoted to partnerships with the private sector.Citation22
This study provides a glimpse into the standards of care in the unregulated private sector, including small hospitals providing maternity care, the same hospitals that the public health sector is supposed to form partnerships with, as seen in recent schemes like Arogyashree, Chiranjeevi and Rashtriya Swasthya Bima Yojana. This evidence is important for formulating guidelines and the contractual basis of such partnerships.
The study highlights the tremendous growth in these hospitals in the last decade. The owners are doctors themselves, in contrast to larger private hospitals run by corporate companies or charitable trusts. The high proportion of ownership of these facilities is in contrast to the past, when such hospitals were housed in rented places.Citation14 This indicates the profit-making potential for doctors, who must have obtained private capital that supports entrepreneurship. These small hospitals are the dominant providers of hospital care in the private sector in Maharashtra, and have penetrated even the less developed regions of the state, often being the only medical care available.
Maternity care forms an important component of care in these hospitals. Despite the huge investment in the Reproductive and Child Health programme in India, there has been increased utilisation of private sector services. The main reasons reported by women for using private sector maternity care were proximity and quick service.Citation29 However, this study throws light on the poor standards of care that may actually pertain.
Private hospitals are governed by laws and regulations for which different departments of the state and district-level committees are responsible. Many of these function in parallel to each other, not in an integrated manner. They should be brought under one umbrella, so that minimum standards can be agreed and better accountability achieved.
Conclusion
The number of hospitals with fewer than 30 beds in the private health sector in Maharashtra has grown over the years without effective regulation or accountability. Existing regulatory bodies, from the medical councils to consumer courts, have been largely ineffective. The state needs to play a stronger role in regulation not just of quality of care but also by setting, monitoring and enforcing minimum standards and determining the scope of the private sector. Information should be collected on health outcomes and quality of care before the state involves these hospitals further in provision of maternity care. Until this is done, including this sector in partnerships with the state for providing services such as maternity care, and particularly emergency obstetric care, may be putting patients at risk and could even end up regularising the poor functioning of this sector. Lastly, the state's own managerial capacity for monitoring public–private partnerships needs to be improved.
Acknowledgements
This paper is based on a study conducted by CEHAT in 2008–09. We acknowledge the contribution of the project research team and thank the Programme Development Committee of CEHAT for their comments on the research report. The research team consisted of Amita Pitre, Amit Khandewale,Chandrima Chatterjee, Padma Deosthali, Ritu Khatri, Ravi Pillai, Sushma Gamre, Suchitra Wagle, Varsha Zende. The Programme Development Committee members include Dr Lakshmi Lingam, Dr Padma Prakash, Sangeeta Rege, Sana Contractor, Dr Padmini Swaminathan and Dr Vibhuti Patel.
Notes
* Hospitals registered as charitable trusts get concessions under various laws. They are required to reserve 20–30% of beds and outpatient services for the poor and weak.
* For more information see <www.cehat.org/go/ResearchAreas/HleprBnhra>.
† Level of urbanization, hospital beds per 100,000 population, under-five mortality rate, female literacy rate, and district domestic product at current year prices.
* Qualified nurses are those with a recognised degree from an institution, either auxillary nurse-midwife (18-month course) or BSc (three-year course). Unqualified nurses do not hold a recognised degree and may or may not have received in-house training.
References
- R Baru. Private Health Care in India: Social Characteristics and Trends. 1998; Sage Publications: Delhi.
- Duggal R. Urban health care: issues and challenges. Background paper for Urban Community Initiative – A Development Challenge of the Holy Family Hospital and Tata Institute of Social Sciences. July 2004.
- Ministry of Statistics and Programme Implementation, India. National Sample Survey Organization 52nd round. New Delhi; 1996.
- Ministry of Statistics and Programme Implementation, India. National Sample Survey Organization 60th round. New Delhi; 2004.
- New Delhi: Planning Commission. Approach paper to the 11th Five Year Plan. Government of India; 2006.
- R Duggal. Public health expenditures, investments and financing under the shadow of a growing private sector. L Gangolli, R Duggal, A Shukla. Review of Health Care in India. 2005; CEHAT: Mumbai, 225–246.
- R Baru. Privatization of health services: a South Asian perspective. Economic and Political Weekly. 38(42): 2003; 4433–4437.
- R Baru. Private health sector in india: raising inequities. L Gangolli, R Duggal, A Shukla. Review of Health Care in India. 2005; CEHAT: Mumbai, 269–277.
- VR Muraleedharan. Characteristics and structure of the private hospital sector in urban India: a study of Madras city. Applied Research Paper. 1999; Partnership for Health Reform Project, ABT Associates: Bethesda MD.
- P Deosthali, R Khatri. Private health sector in Maharashtra: a study of private hospitals. 2010; CEHAT: Mumbai.
- Rao, Nundy SM, Dua A. Delivery of health care services in the private sector: financing and delivery of health care services in India. National Commission of Macroeconomics and Health background papers. Ministry of Health and Family Welfare, Government of India. New Delhi; 2005.
- R Baru, A Acharya, S Acharya. Inequities in access to health services in India: caste, class and region. Economic and Political Weekly. 45(38): 2010; 49–58.
- S Nandraj. Beyond the law and the Lord, quality of private health care. Economic and Political Weekly. 29(27): 1994; 1680–1685.
- S Nandraj, R Duggal. Physical standards in private health sector: a case study of rural Maharashtra. 1997; CEHAT: Mumbai.
- Private sector health care in developing countries needs better stewardship researchers say. Bulletin of World Health Organization. 23 April 2002. At: <www.who.int/bulletin/releases/2002/04/en/index.html. >.
- R Bhat. Characteristics of private medical practice in India: a provider perspective. Health Policy and Planning. 14(1): 1999; 26–37.
- M Pai. Medical interventions: caesarean sections as a case study. Economic and Political Weekly. 35(31): 2000; 2755–2761.
- U Sudhir. Womb removal: Andhra's big medical scandal. 27 August 2010. At: <www.ndtv.com/article/india/womb-removal-andhras-big-medical-scandal-47462. >.
- RK Homan, KR Thankappan. An examination of public and private sector sources of inpatient care in Trivandrum district, Kerala. 1999; Achuta Menon Centre for Health Services: Thiruvananthapuram.
- Moyna. Menopaused 20-somethings. Down to Earth. 15 June 2010. At: <www.downtoearth.org.in/node/668. >.
- R Baru, M Nundy. Blurring boundaries in public–private partnerships in health services in India. Economic and Political Weekly. January: 2008; 62–71.
- National Conference Report. Emerging health care models: engaging the private sector. Mumbai, 25–26 September 2009. At: <www.cehat.org/go/uploads/PPP/reportfinal.pdf. >.
- A Kastia, R Bisht. Investigating PPP health model Chiranjeevi Yojana, Sabarkantha district, Gujarat. Presented at: Emerging health care models: engaging the private sector. Mumbai, 25–26 September 2009. At: <www.cehat.org/go/uploads/PPP/anuja.ppt. >.
- Government of India. Rashtriya Swasthya Bima Yojana. At: <www.rsby.gov.in. >.
- Health information of India 2005. At: <http://cbhidghs.nic.in/hia2005/content.asp. >.
- R Duggal, T Dilip, P Raymus. Health and healthcare in Maharashtra: a status report. 2005; CEHAT: Mumbai.
- S Saha. Perception about quality of women's reproductive health services in Solapur, Maharashtra. 2005; CEHAT: Mumbai.
- TR Dilip, R Duggal. Unmet need for public health care services in Mumbai. Asia-Pacific Population Journal. 19(2): 2004
- Ministry of Health and Family Welfare. National Family Health Survey: Maharashtra. 2005–06; Government of India: New Delhi.
- Bombay Nursing Home Registration Act 1949. Government of Maharashtra. Public Health Department. Directorate of Health Services. At: <www.maharashtra.gov.in/data/gr/marathi/2003/05/10/20030819165545001.pdf. >.
- Government of Maharashtra. Human Development Report Maharashtra. 2002; UNDP: New Delhi.
- Government of Maharashtra. Public Health Department. Directorate of Health Services. At: <www.cehat.org/go/BnhraWeb/Bnhraintro. >.
- G Shenoy. Reporting notifiable diseases to authorities. Express Healthcare Management. 1–15 December 2003. At: <www.expresshealthcaremgmt.com/20031215/legalities01.shtml. >.
- National Health Policy 2002. At: <http://mohfw.nic.in/np2002.htm. >.
- National Rural Health Mission. Ministry of Health and Family Welfare. Government of India. New Delhi: 2007. At: <www.mohfw.nic.in/nrhm.htm. >.