Abstract
Organizational changes, increased funding and the demands of HIV antiretroviral (ARV) treatment create particular challenges for governance in the health sector. We assess resource allocation, policy making and integration of the national responses to ARV provision and reproductive health in Burkina Faso, using national and district budgets related to disease burden, policy documents, organizational structures, and coordination and implementation processes. ARV provision represents the concept of a “crisis scenario”, in which reforms are pushed due to a perception of urgent need, whereas the national reproductive health programme, which is older and more integrated, represents a “politics-as-usual scenario”. Findings show that the early years of the national response to HIV and AIDS were characterized by new institutions with overlapping functions, and failure to integrate with and strengthen existing structures. National and district budget allocations for HIV compared to other interventions were disproportionately high when assessed against burden of disease. Strategic documents for ARV provision were relatively less developed and referred to, compared to those of the Ministry of Health Directorates for HIV and for Family Health and district health planning teams for reproductive health services. Imbalances and new structures potentially trigger important adverse effects which are difficult to remedy and likely to increase due to the dynamics they create. It therefore becomes crucial, from the outset, to integrate HIV/AIDS funding and responses into health systems.
Résumé
Les changements organisationnels, l'augmentation du financement et les besoins en traitement antirétroviral du VIH créent des défis particuliers pour la gouvernance dans le secteur de la santé. Nous étudions l'allocation des ressources, la formulation des politiques et l'intégration des activités nationales de traitement antirétroviral et de santé génésique au Burkina Faso, sur la base des budgets nationaux et de district par rapport à la charge de morbidité, les documents politiques, les structures organisationnelles et les processus de coordination et d'application. Le traitement antirétroviral représente un « scénario de crise », où les réformes sont passées au nom d'un besoin urgent, alors que le programme national de santé génésique, plus ancien et mieux intégré, relève de la « vie politique courante ». Les conclusions montrent que pendant les premières années de la riposte nationale au VIH/sida, on a créé des institutions avec des fonctions se chevauchant, incapables de s'intégrer dans les structures existantes et de les renforcer. Les allocations budgétaires nationales et de district pour le VIH étaient disproportionnées par rapport à d'autres interventions, compte tenu de la charge de morbidité. Les documents stratégiques pour le traitement antirétroviral étaient relativement moins développés et moins mentionnés que ceux des directions générales du Ministère de la santé pour le VIH et la santé familiale, et des équipes de planification sanitaire de district pour les services de santé génésique. Les déséquilibres et les nouvelles structures déclenchent potentiellement des effets indésirables difficiles à corriger et qui risquent d'augmenter en raison de la dynamique qu'ils créent. Il devient donc essentiel d'intégrer dès le début le financement et les activités de VIH/sida dans les systèmes de santé.
Resumen
Los cambios organizacionales, el aumento de fondos y las demandas del tratamiento antirretroviral (ARV) del VIH crean retos específicos para la gobernancia en el sector salud. Evaluamos la asignación de recursos, formulación de políticas e integración de las respuestas nacionales al suministro de ARV y la salud reproductiva en Burkina Faso, empleando presupuestos nacionales y distritales relacionados con la carga de enfermedad, documentos de políticas, estructuras organizacionales y procesos de coordinación e implementación. El suministro de ARV representa el concepto de una “situación de crisis”, en la cual se insta a realizar reformas debido a la percepción de necesidad urgente, mientras que el programa nacional de salud reproductiva, que es más antiguo y más integrado, representa una “situación de política como de costumbre”. Los hallazgos muestran que los primeros años de la respuesta nacional al VIH y SIDA eran caracterizados por nuevas instituciones con funciones superpuestas y por la falta de integración a estructuras ya establecidas y falta de fortalecimiento de éstas. Comparada con otras intervenciones, la asignación de presupuestos nacionales y distritales para el VIH era desproporcionadamente alta comparada con la carga de enfermedad. Los documentos estratégicos para el suministro de ARV fueron relativamente menos elaborados y mencionados, comparados con las Oficinas de VIH y Salud de la Familia del Ministerio de Salud y los equipos de planificación de salud distrital para servicios de salud reproductiva. Los desequilibrios y las nuevas estructuras posiblemente provoquen importantes efectos adversos, que son difíciles de remediar y proclives a aumentar debido a las dinámicas que crean. Por ello, es crucial integrar en los sistemas de salud, desde el principio, los fondos y las respuestas para la lucha contra el VIH/SIDA.
Providing integrated services in comprehensive reproductive and sexual health programmes was a central theme of the 1994 Cairo International Conference on Population and Development (ICPD).Citation1 Global debates on the need to integrate HIV/AIDS into sexual and reproductive health have been ongoing. The UN Millennium Development Goals (MDGs) incorporated the goal of universal access to reproductive health with maternal health while combating HIV remained a separate goal with malaria and tuberculosis.Citation2 We carried out research on how these international policies have (or have not) translated into integration of HIV antiretroviral (ARV) treatment at policy making level in Burkina Faso. The national ARV scale-up has seen considerable progress: ARV coverage rose from 7% in 2004 to 35% in 2007. In 2006, 12,842 people living with HIV received ARVs; in 2009, this number had increased to 26,448. HIV prevalence in Burkina Faso was 1.6 percent in 2008, which is relatively low compared to other sub-Saharan countries.Citation3
National indicators show important resource constraints, poor outcomes and gaps in essential health services. Burkina Faso is one of the world's poorest countries; 46.4% of the population live below the poverty line on less than US$1 per day.Citation1 In the early 1990s, the country initiated health sector reforms, focusing on decentralization, cost recovery, and increasing the supply of essential drugs, among others.Citation4 Following the Bamaco Initiative in 2001, health expenditure as a percentage of total government expenditure between 2002 and 2007 was increased from 8.9% to 13.3%. Private expenditure on health as a percentage of total expenditure on health during these years decreased from 60% to 44%. About a third of national health expenditure is externally funded. Total national expenditure on health per capita, excluding private expenditure, was US$19.38 in 2007.Citation5 National expenditure on HIV/AIDS has been almost entirely donor funded; disbursements in 2007 were US$1.58 per capita.Citation6 The country in 2008 had a population of about 16 million and an annual population growth rate of 3.1%, a high total fertility rate of 6.34, an infant mortality rate of 86 per 1,000, and a life expectancy of 53 years.Citation3
Health outcomes and coverage indicators suggest that despite reform efforts and increased funding, important shortages still persist with regard to essential health services. A survey showed that only five out of 53 districts had the number of physicians defined as the needed minimum. 57% of physicians were working in the cities of Ouagadougou and Bobo-Dioulasso, which account for 16% of the population. Physician absenteeism was reported to be 37%. Two out of 14 centres encountered shortages in the range of 30 days per year of high-use medicines. Only 17 of the 53 district hospitals had the capacity to do caesarean sections.Citation7 Access to health services is further constrained by Burkina Faso being one of the countries in the region where common generic drugs are the most expensive. A study showed that about 35% of people who did not seek health care stated that this was due to inability to pay. Two-thirds of people accessing care said they had difficulties meeting health expenses.Citation4 Altogether, these data show that important gaps remain in the delivery of essential and basic services that are relatively simple to manage compared to ARV treatment. In the context of scarce resources, such gaps increase the need to set priorities according to burden of disease and to aim for efficiency gains through integrated approaches that will improve accessibility, user-friendliness and efficiency of service delivery through sharing of resources and avoidance of duplication in planning, management and administration.
HIV treatment programmes constitute the largest, most costly and most complex therapeutic public health intervention ever undertaken in low-income countries. They are characterised by a relatively high international and national political profile, high levels of funding and relatively short-term and ambitious targets. Organizational changes and other consequences of increased levels of funding, demands and expectations create particular challenges for governance in the health sector. However, despite an increasing focus on HIV programmes and the governance they require, the demands made on policy making and implementation are rarely examined in detail at national level, and less so at district level.Citation8 Existing reviews of evidence on the effects of ARV treatment expansion on health systems, including on the governance of health systems,Citation9–14 generally conclude that disease-specific programmes have led to the creation of parallel structures with short-term targets, motivated by a sense of urgency or crisis. The creation of national AIDS Commissions has been a policy promoted by UNAIDS and the Global Fund to Fight AIDS, TB and Malaria (Global Fund) and implemented in most low-income countries. Merits and drawbacks of these have been subject to global debate, but research has not specifically examined their role in relation to integrated programmes.
Grindle and Thomas refer to the creation of a “crisis scenario” if reforms are pushed due to a perception of urgent need, as opposed to “politics-as-usual scenarios” representing incremental health systems strengthening efforts.Citation15 They find important differences in the two types of initiatives as regards how decisions are taken, how bureaucratic agencies engage, and other process characteristics, and with timing and incrementalism, among others.Citation15 We use these concepts to illustrate the difference between ARV programmes and older essential health interventions and structures, exemplified by the national programme for reproductive health and district health planning structures.
Governance in the health sector is a relatively new and undeveloped analytical area, with consequently little guidance on how to generate feasible and useful research questions. It is a multi-dimensional concept which commonly involves both actors and institutions, and is therefore at the core of any process undertaken within a health system and a main driver of performance. A WHO framework defines governance as generating intelligence; formulating strategic policy direction; ensuring tools for implementation through powers, incentives and sanctions; building coalition and partnership; ensuring a fit between policy objectives and organizational structure; and ensuring accountability.Citation16Citation17 Policy is a closely related concept, which commonly refers to rhetoric and political speeches, written documents, and institutional mechanisms, as well as the daily interaction of local administrators.Citation18 Policy analysis looks at the elements of a policy process and the political and social forces as they affect implementation, and draws on political science and public administration perspectives.Citation19
Given the encompassing nature of both governance and policy analysis, a focus on specific manifestations of governance is required, regarding ones that are both relevant and feasible to assess. One way is to consider those dimensions of governance closely linked to implementation. Organizational structures and the development and use of strategic documents for agenda setting and policy formulation qualify for this. Measurability, another criterion, requires clearly defined units and again, policy documents qualify as such. No universally applicable guidelines exist to assess policy documents, however. A 2006 evaluation of the global AIDS response by the Overseas Development Institute (ODI), for example, looked at how far national HIV strategies contained explicit objectives, budgets and operational plans and whether they were developed in a participatory manner. It concludes that few policies were explicit about priorities, only 60% contained budgets, and only about half of the policies were translated into operational plans, including for monitoring and evaluation. Plans were commonly developed by external consultants with little participation of national stakeholders.Citation20 Similar criteria are contained in the Appraisal of Guidelines, Research and Evaluation in Europe (AGREE) instrument, a generally accepted framework for assessing the quality of clinical guidelines.Citation21 Using these models, we examine the governance of Burkina Faso's national ARV treatment programme in relation to its reproductive health programmes, with a focus on integration and progress at policy level. We compare their budgetsFootnote* and the form of health policy making for both, based on a qualitative assessment of organizational structures, extent of cooperation, and development and use of strategic documents.
Methods
This policy analysis was part of a multi-centre research project “Effects of antiretrovirals for HIV on African health systems, maternal and child health (ARVMAC)”, between 2007 and 2010, which looked at the effects of HIV antiretroviral treatment programmes on African health systems, including maternal and child health programmes. It was carried out in three health and demographic surveillance sites: Iganga-Mayuge in Uganda, Nouna in Burkina Faso and Rufiji in Tanzania. It complemented other ARVMAC studies on health performance, human resources, access to health services and health outcomes.
To assess district budget allocation compared to burden of disease, we used annual district plans and budgets and collected information on costs not included in those budgets. All data were entered in a modified version of a district health accounts tool first introduced through the Tanzania Ministry of Health's Essential Health Interventions Programme.Citation22Citation23 It tabulates 52 health interventions which form six disease areas. It then maps budgets against burden of disease profiles addressable with interventions. Burden of disease profiles are those provided by the respective sentinel district demographic surveillance sites in each district.Citation24 For information on national donor funding for HIV and AIDS compared to other health interventions, we also drew on the creditor reporting system compiled by the Organisation for Economic Co-operation and Development (OECD). The database reports bilateral funding from the 22 OECD member states, and since 2007 16 multilateral donors have also been included, e.g. the World Bank and the Global Fund.Citation6
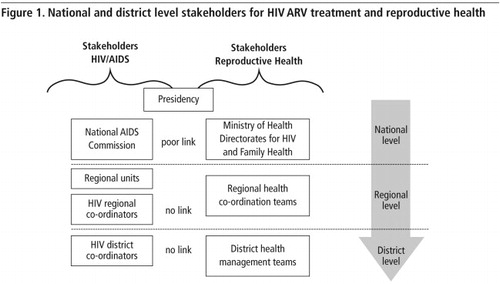
Organizational structures assessed within the “crisis-scenario” include the national AIDS Commission and the Ministry of Health (MoH) Directorate for HIV, both with their respective units at decentralized level. Organizational structures assessed within the “politics-as-usual scenario” include the MoH Directorate for Family Health and district health planning teams. Primary data sources were informant interviews and policy documents. Interviews took place in Ouagadougou, the capital of Burkina Faso, the city of Nouna, Nouna district and its regional capital Dedougou. Nouna district was chosen because it was the research site of the larger research project. Key informant interviews were conducted in French by the principal investigator and in close cooperation with a local research team, who are co-authors on this paper. Three representatives from the national AIDS Commission, one or two representatives each from the MoH Directorates (Reproductive Health, HIV, Malaria, TB, Human Resources), one representative each from WHO, the national sector development programme, the UN support programme for non-governmental organisations (NGOs), the French and Dutch bilateral agencies, and four NGOs were interviewed. Regional level interviews included the head of the regional AIDS Commission as well as the head of the regional health planning team. At district level we interviewed the district health officer as well as other members of the district planning team, the district pharmacist, physicians at the district hospital and local NGOs. Interviews took place in 2007 and again in 2008 to follow up developments. The first round of interviews included 27 interviews at national level, four interviews at district level and two interviews at regional level. The second round included 12 interviews at national level and two at district level. Topics during interviewing included concerns of participants, challenges and progress of interventions, the role of different stakeholders, institutions and events, as well as contextual issues. Specific questions included details of how policy documents were developed and who participated in the process, and how far these documents were being used for planning and implementation.
We used triangulation of methods, comparing findings from different interviews and findings from the literature. This included reinterpretation of results and search for new evidence until more coherent overall conclusions could be reached, as suggested by Rychetnik.Citation25 We used an open approach based on grounded theory implying that the process of data collection itself leads to the development of frameworks.Citation26 The objective was to allow for the unpredictability of findings and to avoid preconceptions about what to find. Interview themes were broadly defined prior to research but then continuously adapted during the process of interviewing. This permitted respondents to bring up new issues according to their points of view.Citation26–28 Findings were transcribed and assessed after interviews to filter out points still unclear and requiring further probing and discussion with the study team and in further interviews. With all interviewees, we sought informed consent and assured confidentiality of responses. Overall ethical approval was obtained by the ARVMAC project in each partner country prior to the start of work.
We reviewed key strategic and planning documents produced between 2004 and 2007 according to pre-defined criteria, including: the national HIV/AIDS strategies, national health strategy, and annual plans of the national AIDS Commission, MoH Directorates for HIV and Family Health, as well as Nouna district annual plans and budgets. We assessed corresponding units at national, regional and district level. To assess policy documents, we worked from the AGREE instrument,Citation21 and derived criteria relevant to the documents being assessed, such as how far the documents were based on evidence for priority setting, how far they presented specific and relevant information, defined targets, activities and budgets, and involved relevant stakeholders during their development.
Findings
The national response to reproductive health and HIV/AIDS
Since Cairo, the national reproductive health policy in Burkina Faso, initially including only family planning, has evolved into a broad concept, including STI/ HIV control, women's rights, sexual education and maternal and child health. Abortion remains legally restricted with exceptions. The MoH Directorate for Family Health develops plans and follows up programmes for maternal and child health. Both the National Population Council and the MoH Directorate for Family Health are responsible for coordinating reproductive health policies.
The HIV epidemic started to be portrayed as a “crisis” that needed a major effort in the early 2000s. Burkina Faso in 2001 hosted the Africa conference on AIDS and Sexually Transmitted Diseases. Two new public structures were set up that year: the national AIDS Commission, which since 2002 has also led the Country Coordinating Mechanism of the Global Fund, and the MoH Directorate for HIV. Prevention of mother-to-child transmission of HIV (PMTCT) is under the mandate of the MoH Directorate for Family Health, while HIV treatment (including for women who received PMTCT) is under the mandate of the MoH Directorate for HIV. Intervention areas of the MoH Directorate for Family Health include family planning, neonatal and obstetric care, integrated management of childhood illness (IMCI), PMTCT and reproductive health for youth.
Implementation of the national reproductive health policy has been mixed and dependent on funding. Antenatal care coverage defined in terms of at least four visits during pregnancy was 18% in 2008, the unmet need for family planning 29%.Citation3 Important weaknesses as identified by the MoH Directorate for Family Health 2007 annual plan included insufficiencies with regard to integrated management of childhood illness, poor funding and stock-outs of family planning methods, interruptions at entry level of PMTCT, poor integration of PMTCT within pre-service training, and poor funding to strengthen district capacities in the area of maternal health. Little integration of PMTCT within district plans was identified as a main reason for its relatively slow expansion.Citation29 Given these persisting challenges, it is vital to aim at needs-based resource allocation as well as potential efficiency gains through integrated approaches.
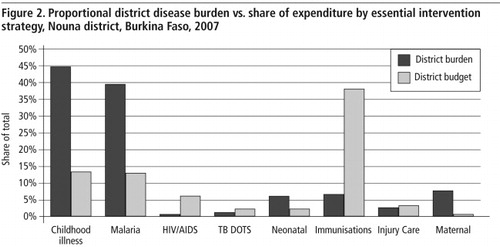
Resource allocation to HIV compared to reproductive health
Our Nouna district 2007 assessment of budgets for different interventions against burden of disease indicated a disproportionately high budget for HIV/AIDS and a disproportionately low budget for integrated management of childhood illness and maternal health, among others (
We investigated numbers of staff to assess balance of allocation of resources. In 2008 the national AIDS Commission had four times as many staff as the Directorate for Family Health and more than eight times as many staff as the Directorate for HIV (Table 1
Table 1
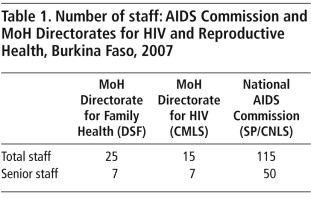
About two-thirds of the ARV treatment programme staff in 2008 were employed by donor-funded project units and received salaries that were 7–10 times higher than public health sector salaries. Interviewees confirmed these imbalances. There were no comprehensive data on salary scales, but estimates from interviewees were that physicians working for NGOs in HIV/AIDS programmes earned approximately double what physicians earned in the public sector.
According to regional and district health planners interviewed, vertical programmes increased the amount of work for reporting and monitoring. The national programmes for TB and HIV especially required resource-intensive quarterly reporting. Monitoring of TB required data from health facility level, monitoring of ARV treatment required data from hospital level. The national immunisation and reproductive health programmes were considered to be better integrated, and their supervision and reporting procedures were part of the standard health information system. A regional health planner estimated that integration of TB into standard procedures could save 24 supervision days, and integration of ARV treatment another 12 days per year.
Policy making for HIV and reproductive health
“We needed a multisectoral and visible national response to HIV” was a repeatedly heard statement, justifying the AIDS Commission's existence in the first place. One respondent, however, opined that the AIDS Commission did not really have “a reason to be” but that rather, an integrated HIV response should have been manifested by integrating the national HIV programme institutionally within the MoH Directorate for Family Health. Views of respondents were less unanimous as regards the planning capacity of the national AIDS Commission:
“It is as if the last three years investing in institutional strengthening have been for nothing; initiatives are not traceable. Usually it is the same people who participate in the training. There is a high number of employees but this does not reflect efficient work capacity.” (Donor)
“When I participated in an annual planning I had the impression that they basically took the five-year plan and divided it by five.” (Donor)
“Many countries are coming to visit the AIDS Commission for their inspiration.” (HIV officer, WHO Burkina Faso)
“The Directorate for Family Health manages well considering its high workload of different programmes; it has to respond to a large number of different demands, including requests from donor agencies...” (MoH staff)
“We are facing the same challenges as we did before HIV, overall low funding, poor infrastructure of the district hospital, and [lack of] essential drugs, especially anti-malarials, for example. It is mainly at national level that everybody talks about HIV/AIDS.” (District level respondents)
A 2007 evaluation of the national AIDS Commission undertaken by the Global Fund had similar findings. It found a disproportionate focus on HIV at the cost of other health sector responses as well as a general absence of national health system strengthening. It also highlighted the creation of new, unbalanced and uncoordinated structures, undefined roles and lack of efforts to align administrative and financial structures: “There is a national committee for every disease. Talk and focus is completely dominated by HIV… no one speaks for malaria.” It also noted inefficiencies, such as large meetings of 80–90 people with little potential for decision-making.Citation32
Analysis of policy documents
The following assessment presents how policy documents were developed and updated based on an analysis of needs relevant to planners, for example in terms of giving specific recommendations, and predicated on other national and international strategies. Documents referred to for analysis were:
| • | National HIV/AIDS strategy and operational plan of the AIDS Commission 2005–2010Citation33Citation34 | ||||
| • | National health strategy 2001–2010Citation35 | ||||
| • | National ART strategy of the MoH Directorate for HIVCitation36 | ||||
| • | Annual plan of the national AIDS CommissionCitation37 | ||||
| • | Annual plans of the MoH Directorate for Family Health 2004–2008Citation29,38–41 | ||||
| • | Annual plans of the MoH Directorate for HIV 2004–2007Citation42–45 | ||||
| • | Annual plans of Nouna Health District 2004–2008Citation46–49 | ||||
Development of documents
The AIDS Commission's strategy was developed over an intensive planning period of four months by bringing together different actors, including MoH Directorates and NGOs. The national health strategy was developed through a one-year process involving stakeholders from the different MoH Directorates, bilateral and multilateral agencies. The process included an extensive revision, which took 4–6 months. District planning teams participated in the development of the national health strategy. Annual district planning in Nouna was a one-month process that involves 15 planning team members at times for several hours per day, added to their other duties. Implementation of the annual plan was followed up through weekly meetings during the year. Similar but far less extensive processes to develop strategies and annual plans were described by the MoH Directorates.
Content of documents
The AIDS Commission's strategy was based on an evaluation of the previous (2001–2005) phase. It took a relatively descriptive rather than analytical approach. It refers to the national development strategy and the MDGs. The current phase of the national health strategy (2006–2011) was also based on an evaluation of the first phase (2001–2005). A mid-term evaluation took place and was used to revise the strategy. It took a strategic approach, highlighting key intervention areas. It is predicated on the national development strategy. The national AIDS strategy of the MoH Directorate for HIV also took a strategic approach in terms of linking up analysis with recommendations. It referred to the national health strategy. Content-wise it contained considerable overlap with the strategy of the national AIDS Commission.
The annual plans of the national AIDS Commission included extensive descriptive details with relatively little analytical interpretation. Activities were not budgeted. It did not refer to the plans of the MoH Directorate for HIV. Little progress and difference existed between plans from one year to the next. The annual plans of the MoH Directorate for HIV included few details regarding planned activities and no analysis apart from a modest situation analysis of the 2008 plan. The AIDS Commission's plans were not referred to. Compared to previous years, the situation analysis of the 2008 plan presented more analytical depth. The other plans showed little progress from one year to the next. The plans of the MoH Directorate for Family Health included a more extensive analysis based on previous years' progress. They provided clearly formulated strategic directions, including for example a summary of strengths and weaknesses or operational issues, such as the need to improve managerial capacities. The plans of Nouna health district contained a relatively detailed reflection of priorities and what was to be implemented during the year. They matched resource allocation to the respective burden of disease profiles.
Application of documents
The national health strategy is used as a key reference for priority setting by MoH Directorates and district planning teams. The strategy and operational plan 2005–2010 of the national AIDS Commission were not referred to as key reference documents by interviewees of the MoH Directorates for HIV and Family Health. Another national ART strategy had been developed by the MoH Directorate for HIV; respondents said it was not used as a reference document or for planning. Districts use their annual plans as a key resource for planning and follow-up throughout the year. They are archived and used for further analysis at national level.
Discussion
Our findings show an imbalance in resource allocation to HIV/AIDS compared to reproductive health, in terms of national and district health budgets assessed against burden of disease, and in staff, budget levels and salaries of the national AIDS Commission compared to the MoH Directorate for Family Health. In general, the HIV response appeared to have a considerably higher political profile at national as compared to district level. One explanation is that national priorities are being shaped by a sense of urgency that is promoted by international events, powerful actors and policies instead of being based on epidemiological evidence and country needs, as expressed at district level.
Newer, well-appointed national AIDS Commission building in contrast to that of the Directorate for Family Health, Burkina Faso


These findings show that highly funded and rapidly established institutions with a high level of highly paid staff at national level do not necessarily result in a high quality policy response or sufficient levels of disbursement at district level. The higher salaries of the AIDS Commission's staff likely cause a drain of qualified people from the public to donor-funded employment. The MoH Directorate for Family Health appeared to suffer less from these weaknesses and be more efficient in terms of numbers of staff in relation to workload, cooperation among staff and the quality of strategic planning. Our assessment of strategic documents substantiates these findings. In accordance with these findings, Panos found that a common weakness of policy documents is a focus on details and too little attention to guidance to set priorities.Citation50 Our findings add a different dimension to the largely positive effects Grindle and Thomas say can be caused by a perception of crisis, that is, the promotion of policy change, innovation and bolder decisions.Citation15
Duplication of roles, new institutions and actors can fragment policy making. New institutions develop their own dynamics and interests, not least staying employed. Parallel structures do not necessarily work towards an integrated health system agenda, but can compete for funds and activities in a situation of inadequate resources. Using already integrated, decentralized and existing structures may avoid inefficiencies caused by additional structures. The “politics-as-usual scenario” is based more on incrementally working within established systems. Decision-making tends to remain at lower hierarchical levels and better engages technical experience and mid-level managers.Citation15 They are therefore more likely to promote decentralisation, local ownership and needs-based priority setting. Taking a more incremental approach recognises that health services are complex adaptive systems as opposed to mechanical systems; that capacity-building is a dynamic, continuous and long-term process, including the need for major personnel, organizational, and institutional change. “Crisis scenarios” based on the need for quick solutions not only lack sustainability but may also have significant unintended and possibly irreversible adverse effects on health systems. New structures need time to become efficient and integrated. The Global Fund, for example, has shown a learning curve in its own work, adapting its approaches based on experiences at country level. There is, however, a risk that structures once set up may later be difficult to change, especially due to organizational inertia caused by the self-interest of people who want to remain in their positions.
It became apparent during interviews that stakeholders agreed on the importance of integration and were aware of current weaknesses in this regard. Some of the causes appeared to be difficult to address, such as separate funding and budgets, and the existence of parallel national institutions to deliver services. To improve integration within the current context, interviewees suggested improvements in lines of communication, joint planning, and coordination of planning cycles between the MoH Directorates and the national AIDS Commission. Integration of donor funding into a sector-wide approach as well as participation of district planning teams, in order to integrate HIV within initiatives targeting maternal and child health, were cited as further important points for a more integrated and balanced approach to HIV/AIDS. The devolution of decision-making powers to the district level has been one of the strongest elements of health sector reform in Burkina Faso and presents important prerequisites to deliver the benefits of integration, including intersectoral HIV/AIDS control.
Improving the quality of planning does not necessarily translate into good or better outcomes; the latter depend on many factors, such as staff capacity and resources at health facility level. Policy documents serve to generate interest in the process of policy formulation and to guide implementation. But their content tends to be lost in the process of implementation when a multitude of other issues come into play. Moreover, we summarised our assessment of the policy documents here, and a number of their specific strengths and weaknesses are not presented in full detail. The research focus included a few governmental directorates and could not cover the role of all stakeholders in depth, including bilateral and multilateral partners and NGOs, disregarding their potential relevance. A related limitation includes not having followed developments over time, and thus missing potential improvements as structures become established.
On the bright side, key informants' views expressed during this research were that since 2008, the situation in Burkina Faso with regard to ARV treatment policy making has changed and generally improved. It could be argued that a comparison of the national AIDS Commission to the MoH Directorates for HIV and Family Health is inappropriate, given the larger mandate of the AIDS Commission to provide a multisectoral response, including areas other than health, such as education and social services. HIV and AIDS are clearly not a health issue alone. Nevertheless – and this was reflected in the AIDS Commission's budgets – most of their response was being implemented through the health sector.
Conclusion
International debates on HIV/AIDS in recent years have hardly acknowledged the potential adverse effects of multisectoral responses, such as inefficient and imbalanced resource allocation due to the setting up of parallel structures. This study found big imbalances in resource allocation to HIV compared to maternal and child health and other reproductive health needs when assessed against the burden of disease in Burkina Faso. The national AIDS Commission's work was not well integrated with that of the MoH Directorates for HIV and Family Health. Their strategic documents were relatively less developed and poorly used compared to those of the public health sector. HIV was much less of a priority and services less visible at district level. District planning went on as “politics-as-usual” with an emphasis on burden of disease-related responses. National and district level structures as well as strategic documents of the “politics-as-usual” sectors were better established and generally of a higher level of quality, likely due to their longer establishment and more incremental and needs-based approaches. Imbalances and new structures potentially trigger important adverse effects which are difficult to remedy and likely to increase due to the dynamics they create. It therefore becomes crucial, from the outset, to integrate HIV/AIDS funding and responses into health systems.
Acknowledgements
“Effects of Antiretrovirals for HIV on African Health Systems, Maternal and Child Health” (ARVMAC) is supported by the European Commission 6th Framework Programme. The ARVMAC consortium includes the following partner institutions: Centre de Recherche en Santé de Nouna, Nouna, Burkina Faso; Ifakara Health Institute, Dar es Salaam, Tanzania; Institute of Tropical Medicine, Antwerp, Belgium; Karolinska Institute, Stockholm, Sweden (Co-ordinating Institute); Makerere University Institute of Public Health, Kampala, Uganda; Swiss Tropical and Public Health Institute, University of Basel, Basel, Switzerland; and Directorate of Global Health, Heidelberg University, Heidelberg, Germany.
Notes
* A more extensive, cross-country, district budget analysis will be presented in another publication, in preparation at this writing.
References
- United Nations Development Programme. Human Development Report 2007/8: Fighting Climate Change: Human Solidarity in a Divided World. 2008; UNDP: New York.
- A Germain, R Dixon-Mueller, G Sen. Back to basics: HIV/AIDS belongs with sexual and reproductive health. Bulletin of World Health Organization. 87: 2009; 840–845.
- World Health Organization. World Health Statistics 2010. 2010; WHO: Geneva.
- S Haddad, A Nougtara, P Fournier. Learning from health system reforms: lessons from Burkina Faso. Tropical Medicine & International Health. 11: 2006; 1889–1897.
- World Health Organization. Global Health Expenditure Database. Burkina Faso – National Expenditure on Health. 2011. At: <http://apps.who.int/nha/database/StandardReport.aspx?ID=REP_WEB_MINI_TEMPLATE_WEB_VERSION&COUNTRYKEY=84523. >.
- OECD. Database on Aid Activities: CRS online. 2011. At: <www.oecd.org/dataoecd/20/29/31753872.htm. >.
- C Bodart, G Servais, YL Mohamed. The influence of health sector reform and external assistance in Burkina Faso. Health Policy & Planning. 16: 2001; 74–86.
- L Gilson, N Raphaely. The terrain of health policy analysis in low and middle income countries: a review of published literature 1994–2007. Health Policy & Planning. 23: 2008; 294–307.
- RG Biesma, R Brugha, A Harmer. The effects of global health initiatives on country health systems: a review of the evidence from HIV/AIDS control. Health Policy & Planning. 24: 2009; 239–252.
- A Case, C Paxson. The Impact of the AIDS Pandemic on Health Services in Africa: Evidence from Demographic and Health Surveys. 2009; National Bureau of Economic Research: Cambridge, MA.
- B Marchal, A Cavalli, G Kegels. Global health actors claim to support health system strengthening-is this reality or rhetoric?. PLoS Medicine. 6: 2009
- G Ooms. From the Global AIDS Response towards Global Health?. 2009; International Civil Society Support Group, Hélène de Beir Foundation.
- D Yu, Y Souteyrand, M Banda. Investment in HIV/AIDS programs: does it help strengthen health systems in developing countries?. Globalization and Health. 4: 2008; 8.
- B Samb, T Evans, M Dybul. An assessment of interactions between global health initiatives and country health systems. Lancet. 373: 2009; 2137–2169.
- MS Grindle, JW Thomas. Public Choices and Policy Change: The Political Economy of Reform in Developing Countries. 1998; John Hopkins University Press: Baltimore, MD.
- P Travis, D Egger, P Davies. Towards better stewardship: concepts and critical issues. Global Programme on Evidence for Health Policy Discussion Papers No. 48. 2002; World Health Organization: Geneva.
- S Siddiqi, TI Masud, S Nishtar. Framework for assessing governance of the health system in developing countries: gateway to good governance. Health Policy. 90: 2009; 13–25.
- C Shore, S Wright. Policy: a new field of anthropology. C Shore, S Wright. Anthropology of Policy: Critical Perspectives on Governance and Power. 1997; Routledge: New York.
- K Buse, N Mays, G Walt. Making Health Policy. 2005; Open University Press: Berkshire.
- K Buse, M Sidibe, D Whyms. Scaling-up the HIV/AIDS Response: From Alignment and Harmonization to Mutual Accountability. 2006; Overseas Development Institute: London.
- The AGREE Collaboration. Appraisal of Guidelines for Research & Evaluation (AGREE) Instrument. London; 2001.
- D de Savigny, D Munna, C Mbuya. District health expenditure mapping: a budget analysis tool for council health management teams. 2001; Ministry of Health: Dar es Salaam.
- Ministry of Health and Social Welfare. PlanRep PMORALG. At: <www.pmoralg.go.tz/mis/planrep.php. >. 2011.
- Indepth. The International Network for the Demographic Evaluation of Populations and their Health in Developing Countries. 2011. At: <www.indepth-network.org. >.
- L Rychetnik, P Hawe, E Waters. A glossary for evidence based public health. Journal of Epidemiology & Community Health. 58: 2004; 538–545.
- B Glaser, A Strauss. The Discovery of Grounded Theory: Strategies for Qualitative Research. 1967; Aldine: Chicago.
- R Weiss. Learning From Strangers; The Art and Method of Qualitative Interview Studies. 1994; The Free Press: New York.
- C Marshall, GB Rossman. Designing Qualitative Research. 1995; Sage Publications: Thousand Oaks.
- DSF. Plan d'action. 2007; Direction Generale de la Santé de la Famille Ministère de la Santé: Ouagadougou.
- Conseil National de lutte contre le SIDA et les IST. Cadre Stragegique de Lutte contre le VIH, le SIDA et les Infections Sexuallement Transmissibles (CLCS) 2011–2015. 2010; Burkina Faso.
- DSF. Plan d'action. 2007; Direction Generale de la Santé de la Famille Ministère de la Santé: Ouagadougou.
- Global Fund to Fight AIDS, TB and Malaria. L'Evaluation des Cinq Ans du Fonds Mondial – Rapport d'évaluation du Partenariat national pour le Burkina Faso. Geneva. 2007.
- SP/CNLS-IST. Cadre Stratégique de Lutte Contre le VIH/SIDA et les Infections Sexuellement Transmissibles (CSLS) 2006–2010. 2005; Secrétariat Permanent du Conseil National de Lutte contre le SIDA et les IST: Ouagadougou.
- SP/CNLS-IST. Plan d'Opérationnalisation du Cadre Stratégique de Lutte Contre le VIH/SIDA et les Infections Sexuellement Transmissibles (CSLS) 2006–2010. 2008; Secrétariat Permanent du Conseil National de Lutte contre le SIDA et les IST: Ouagadougou.
- Ministère de la Santé. Programme National du Développement Sanitaire (PNDS) 2001–2010. 2005. Ouagadougou.
- CMLS. Plan d'extension de la Prise en charge Medicale des Personnes Vivant avec le VIH/SIDA y compris par les Antiretroviraux au Burkina Faso. 2005; Comite Ministériel de Lutte contre le VIH/SIDA et les IST, Ministère de la Santé: Ouagadougou.
- SP/CNLS-IST. Plan National Multisectoriel de Lutte contre le VIH/SIDA et les IST Annee 2007. 2007; Secrétariat Permanent du Conseil National de Lutte contre le SIDA et les IST: Ouagadougou.
- DSF. Plan d'action. 2003; Direction Generale de la Santé de la Famille Ministère de la Santé: Ouagadougou.
- DSF. Plan d'action. 2004; Direction Generale de la Santé de la Famille Ministère de la Santé: Ouagadougou.
- DSF. Plan d'action. 2005; Direction Generale de la Santé de la Famille Ministère de la Santé: Ouagadougou.
- DSF. Plan d'action. 2006; Direction Generale de la Santé de la Famille Ministère de la Santé: Ouagadougou.
- CMLS. Plan d'action opérationnelle de Lutte contre le VIH/SIDA et les IST Secteur Santé 2004. 2004; Comite Ministériel de Lutte contre le VIH/SIDA et les IST, Ministère de la Santé: Ouagadougou.
- CMLS. Plan d'action opérationnelle de Lutte contre le VIH/SIDA et les IST Secteur Santé 2005. 2005; Comite Ministériel de Lutte contre le VIH/SIDA et les IST, Ministère de la Santé: Ouagadougou.
- CMLS. Plan d'action opérationnelle de Lutte contre le VIH/SIDA et les IST Secteur Santé 2006. 2006; Comite Ministériel de Lutte contre le VIH/SIDA et les IST, Ministère de la Santé: Ouagadougou.
- CMLS. Plan d'action opérationnelle de Lutte contre le VIH/SIDA et les IST Secteur Santé 2007. 2007; Comite Ministériel de Lutte contre le VIH/SIDA et les IST, Ministère de la Santé: Ouagadougou.
- ECD. Plan d'Action 2006 District Sanitaire de Nouna. 2005; Ministère de la Santé, Region Boucle du Mouhoun, Direction Regionale de la Santé, District Sanitaire de Nouna: Burkina Faso.
- ECD. Plan d'Action 2007 District Sanitaire de Nouna. 2006; Ministère de la Santé, Region Boucle du Mouhoun, Direction Regionale de la Santé, District Sanitaire de Nouna: Burkina Faso.
- ECD. Plan d'Action 2008 District Sanitaire de Nouna. 2007; Ministère de la Santé, Region Boucle du Mouhoun, Direction Regionale de la Santé, District Sanitaire de Nouna: Burkina Faso.
- ECD. Plan d'Action 2009 District Sanitaire de Nouna. 2008; Ministère de la Santé, Region Boucle du Mouhoun, Direction Regionale de la Santé, District Sanitaire de Nouna: Burkina Faso.
- Panos. Antiretroviral drugs for all? Obstacles to access to HIV/AIDS treatment. Lessons from Ethiopia, Haiti, India, Nepal and Zambia. 2006; Panos Global AIDS Programme: Southern Africa.