Abstract
Research on the consequences of reproductive morbidity for women's lives and their economic and social roles is relatively under-developed. There is also a lack of consensus on appropriate conceptual frameworks to understand the social determinants of reproductive morbidity as well as their social and economic implications. We report here on an exploratory study in Yemen using quantitative (n=72 women) and qualitative methods (n=35 women), in 2005 and 2007 respectively, with women suffering from uterine prolapse, infertility or pelvic inflammatory disease (PID). It explored women's views on how reproductive morbidity affected their lives, marital security and their households, and the burden of paying for treatment. We also interviewed six health professionals about women's health care-seeking for these conditions. Sixty per cent of women reported that treatment was not affordable, and 43% had to sell assets or take out a loan to pay for care. Prolapse and PID interfered particularly in subsistence and household activities while infertility created social pressure. Reproductive morbidity is not a priority in Yemen, given its multiple public health needs and low resources, but by failing to provide comprehensive and affordable services for women, the country incurs developmental losses.
Résumé
La recherche relative aux conséquences de la morbidité génésique sur la vie des femmes et leurs rôles économiques et sociaux est relativement sous-développée. On constate également un manque de consensus sur les cadres conceptuels appropriés pour comprendre les déterminants sociaux de la morbidité génésique ainsi que leurs répercussions sociales et économiques. Nous rendons compte ici d'une étude exploratoire réalisée au Yémen à l'aide d'une méthode quantitative (n=72 femmes) et qualitative (n=35 femmes), en 2005 et 2007 respectivement, avec des femmes souffrant de prolapsus utérin, d'infécondité ou de maladie inflammatoire pelvienne (MIP). Elle a analysé l'opinion des femmes sur l'influence de la morbidité génésique sur leur vie, leur sécurité conjugale et leur ménage, et la charge financière du traitement. Nous avons aussi interrogé six professionnels de la santé sur la demande de soins des femmes pour ces affections. Soixante pour cent des femmes ont indiqué que le traitement était trop cher et 43% avaient dû vendre des biens ou prendre un crédit pour le payer. Le prolapsus et la MIP contrariaient particulièrement les moyens de subsistance et les activités du ménage, alors que l'infécondité créait des pressions sociales. La morbidité génésique n'est pas une priorité au Yémen compte tenu de ses multiples besoins de santé publique et ses faibles ressources, mais en n'assurant pas des services complets et abordables aux femmes, le pays s'expose à une perte de développement.
Resumen
Las investigaciones sobre las consecuencias de la morbilidad reproductiva en la vida de las mujeres y sus funciones económicas y sociales están relativamente subdesarrolladas. Existe falta de consenso en cuanto a los marcos conceptuales adecuados para entender los determinantes sociales de la morbilidad reproductiva y sus implicaciones sociales y económicas. Aquí se informa sobre un estudio exploratorio en Yemen con métodos cuantitativos (n=72 mujeres) y cualitativos (n=35 mujeres), en 2005 y 2007 respectivamente; las mujeres sufrían de prolapso uterino, infertilidad o enfermedad pélvica inflamatoria (EPI). Se exploraron los puntos de vista de las mujeres en cuanto a cómo la morbilidad reproductiva afectó su vida, su seguridad matrimonial y su hogar, así como la carga de pagar por el tratamiento. Además, entrevistamos a seis profesionales de la salud sobre la búsqueda de atención para estas enfermedades. El 60% de las mujeres dijeron que no podían pagar por el tratamiento; el 43% tuvo que vender todos sus bienes o solicitar un préstamo para pagar por los servicios. El prolapso y la EPI interfirieron particularmente en la subsistencia y en tareas domésticas, mientras que la infertilidad creó presión social. La morbilidad reproductiva no es una prioridad en Yemen, debido a sus numerosas necesidades de salud pública y escasos recursos, pero al no ofrecer servicios integrales y a precios razonables para las mujeres, el país sufre pérdidas de desarrollo.
There have been relatively few community-based studies in developing countries of reproductive morbidity, with the exception of South Asia,Citation1,2 and data on prevalence are typically lacking.Citation3 While population-based surveys in many countries, including Yemen, include questions about women's reported symptoms of some reproductive morbidities, these are unlikely to be valid measures of prevalence without clinical examination, which is costly and difficult to conduct in field settings.Citation4 Even less is known about the consequences of reproductive morbidity for women's lives and their economic and social roles.Citation1,2,5 One early qualitative study of women's experiences of utero-vaginal prolapse in India documented the negative consequences for women's lives.Citation6 More recently longitudinal follow-up of women who experienced major obstetric complications has shown an increased risk of mortality and depression among them and impoverishment of their households.Citation7,8
There is also a lack of consensus on appropriate conceptual frameworks for understanding the social determinants of reproductive morbidity as well as the social and economic implications, which could raise the visibility of these problems and their consequences, as advocacy tools to motivate health policy.Citation3 DALYs for measuring health are useful both as a tool for priority setting among competing health needs and for international comparability, but researchers have criticised their omission of the social and non-medical implications of ill-health.Citation9,10 Difficulties in accessing care and paying for treatment mean that reproductive morbidities remain untreated, with potentially serious sequelae. Compounding their physical impact (discomfort or pain) are their social implications, such as stigma and shame. Such effects may impede treatment-seeking and involvement in daily activities, with economic implications for households.
An alternative conceptual framework of potential relevance is the capabilities approach,Citation11–14 which sees poverty as capability deprivation and argues that policies should be evaluated for how well they improve the objective features of how people actually live and the aspects they value (e.g. being free from unacceptable deprivation). This may be more useful than DALYs because it can help to frame the determinants as well as the consequences of morbidity and because it takes into consideration both women's “agency” and enabling opportunities (“social arrangements”). There has been increasing application of the capabilities approach across education, disability and social development and more recently, public health, but with as yet limited application to reproductive health.Citation15–17
In the Middle East, there is evidence that women bear a high level of untreated reproductive morbidity. The Giza study in Egypt provided the first evidence that women often bear these conditions within a “culture of silence” and rarely report them to health service providers.Citation18 Reproductive morbidity thus becomes an area described by Amartya SenCitation13 as one where individuals in unfavourable or deprived circumstances adapt to the adversity and do not indicate that it affects their actual well-being. Confirming international findings,Citation1,4 clinic-based prevalence estimates of morbidity in the region may under-estimate their true prevalence. Community-based studies on reproductive morbidity have subsequently been conducted on reproductive tract infections (RTIs) and prolapse in LebanonCitation19 and Jordan.Citation20 Oman is the only Arab country to have published national data that includes both women's reports and clinical diagnosis.Citation21
As no data are available for Yemen, we decided to conduct an exploratory study in the capital Sana'a, using quantitative and qualitative methods among women suffering from uterine prolapse, infertility and pelvic inflammatory disease (PID). The objectives of the study were: 1) to explore constraints to health care-seeking and women's perceptions of the implications of the three conditions for their own lives and the economic implications of seeking care for their households; 2) to understand women's perspectives about the determinants of these conditions; 3) to investigate selected providers' views about health-seeking for these conditions; and 4) to test the empirical application of the capabilities approach to reproductive morbidity.
Reproductive morbidity includes a wide range of conditions. We chose these three conditions because they represent a range of both gynaecological and obstetric morbidity, with both physical and social implications; one (infertility) does not feature prominently in DALYsFootnote*; and they have received little policy attention in Yemen.
The Republic of Yemen was formed in 1990 following the unification of the (capitalist) North and the (socialist) South, and has had a turbulent political history. It is a low-income country which relies heavily on oil, labour migrant remittances from the Gulf States (reduced due to regional politics), and the production of qat (leaves that are chewed to achieve a euphoric sensation, widely used in Yemen). In 2003, 42% of the population were living below the poverty line and 19% in absolute poverty.Citation22 The situation is likely to have worsened since then. Yemen ranks 133 out of 169 countries on the 2010 Human Development Index. It has very low school enrolment ratios for girls and high rates of illiteracy among women. Yemeni women are almost absent from parliament and local councils and have limited legal rights.Citation23
Yemen also has extremely poor indicators of women's health, with female life expectancy at birth of only 63.Citation24 On the Mother's Index, Yemen ranks 90th out of 94 ranked countries,Citation24 has the highest fertility rate in the region (5.6 in 2006Citation24) and a life-time risk of maternal death of one in 19.Citation24 According to the Yemen Family Health Survey of 2003, the most recent nationally representative data available, 51% of Yemeni women reported complications during pregnancy, delivery (30%) and the puerperium (32%). Female genital mutilation is practised in the coastal areas with a national prevalence of 38% among ever-married women, while 22% of ever-married women of reproductive age and 10% aged 15–19 reported symptoms of genital prolapse. More than half of those reporting prolapse had been affected by it for five years or more. Overall 14% of urban and 16% of rural ever-married women reported symptoms of vaginal discharge indicative of a reproductive tract infection (RTI). Yet women reported major barriers to the utilisation of services, which was low, including cost and perceptions of poor quality of care. Poverty, limited mobility and the low status of women and the country's hilly topography have all contributed to Yemeni women's low health care utilisation. For example, in 2003, 77% of women gave birth to their last child at home and only 45% of pregnant women received any antenatal care for their last pregnancy.Citation25 Whereas elsewhere in the region the age at marriage is rising, Yemen has a low average age at marriage for girls, especially in rural areas, and recent efforts to institute a minimum age of marriage have been opposed.Citation26
The quality of health care in Yemen is poor, and avoidable risks of maternal death are high.Citation27,28 AttalCitation29 found that the quality of delivery care is substandard, and that in both the public and private hospitals studied, there was a shortage of blood, life-saving equipment and medication. A needs assessment in 2006 of health centres in eight districts found that none provided all basic emergency obstetric care functions, and none had a blood bank. Moreover, providers lacked technical competence and knowledge to handle even basic obstetric complications.Citation30 A hospital-based study in Sana'a also reported high levels of uterine rupture with inappropriate oxytocin use for labour augmentation a factor.Citation31 Bahubaishi found that the quality of family planning services in Yemen is deficient, particularly in provider–patient communication and infection control.Citation32 No published information is available on the quality of health care for reproductive morbidity.
Existing services for reproductive morbidity include public hospital out-patient departments, private obstetric-gynaecology clinics and primary health care. Only Sana'a has specialised services for infertility. In the public sector, there is a low registration cost and no doctors' fees but patients have to pay for laboratory tests and medicines.
Methods
The study had three components. The first was a quantitative survey in late 2005 of a convenience sample of 72 women recruited from three tertiary hospitals in Sana'a, diagnosed with one of the three conditions. Given low health care utilisation for reproductive morbidity, we used convenience sampling through clinics and hospitals. While we intended to interview more prolapse and fistulae cases, both proved difficult to recruit in these clinics. Of the three hospital recruitment sites, one was associated with a university but financially independent; one was private and the third governmental. Two of the hospitals specialised in maternal and child health. All three hospitals received referral cases from across the country. Recruitment also took place at an infertility clinic in Sana'a. Interviews were conducted either at the facility itself in a private location or at the women's homes. To be included, women had to be Yemeni and to have received a confirmed diagnosis of one of the three conditions. Data collection took place in Sana'a but included women from other parts of the country who had come there for treatment.
Ethical approval was granted by the University of Sana'a and the American University of Beirut.
In the survey group, 32 women were infertile (24 primary and 8 secondary), 32 had PID and 8 had uterine prolapse. The structured questionnaireFootnote* had primarily closed- and some open-ended questions. It was translated into Yemeni Arabic, piloted and amended. Given the exploratory nature of the study and the use of the capabilities conceptual approach, we did not use pre-defined tools such as the WHO quality-of-life tools.Citation33 The questions addressed reproductive history, experience of reproductive morbidity, health care-seeking and associated costs, and the implications of the condition. Data were analysed in 2006 using SPSS for descriptive statistics only, given the non-representative nature of the sample.
Qualitative interviews were subsequently conducted in 2007 with a sample of 35 other women with a confirmed diagnosis of the same morbidity conditions, including 11 with PID, 11 with infertility and 13 with prolapse. They were recruited also in Sana'a, including from the same infertility clinic, a private obstetric-gynaecology clinic and a governmental hospital (in-patient or out-patient wards. Some of the women with prolapse were in-patients, recovering from surgery. Approaching women in in-patient and outpatient wards allowed for a higher recruitment of prolapse cases.
The qualitative interview guides were translated into Yemeni Arabic, pilot-tested and further refined. These focused on the same issues as the questionnaire, with the addition of women's perceptions of the cause of the morbidity; stigma and disclosure issues related to the condition and with more probing on its impact on social and marital relations. The open-ended interviews, conducted in Arabic, lasted 30–60 minutes. They were digitally recorded (for the 15 who consented to this), transcribed verbatim and those in Arabic translated into English. For the 20 participants who did not want to be taped, the interviewer made detailed notes immediately following the interview. Transcripts and notes were analysed thematically manually; the qualitative interviewer analysed the interviews by theme in Arabic and the first author analysed the transcripts in English. A consolidated list of themes was formed according to which the data were coded and analysed in 2008.
Interviews were later conducted with a convenience sample of six health care providers who regularly treated with reproductive morbidity. We focused on their views about the determinants and effects of reproductive morbidity conditions, and health care-seeking by women. The findings were consolidated in 2009 and disseminated in Yemen in 2010.
Findings
Participants
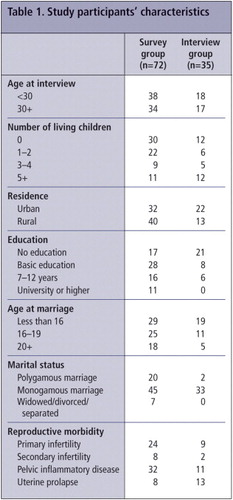
In the survey group, three-quarters of the 72 women had married at age 19 or younger and 40% below the age of 16. About a quarter of them had had no education. Of the interview group, over half were under 30 years old and had married before the age of 16, most had had no education and about half had three or more living children. Overall, 32 of the 72 women in the survey group and 22 of the 35 women in the interview group were living in an urban area (Table 1
Four of the six providers were general practitioners and two had a specialisation in obstetrics and gynaecology. Five of the six worked in government facilities but, as is typical in Yemen, had private clinics in the afternoons. One was on secondment from the government working with an NGO. They ranged in experience from 10 to 25 years and were all working in clinics that treated women with the three types of morbidity we were studying.
Health care-seeking and its economic implications
Table 2 presents key indicators related to health care-seeking for the three morbidity conditions among the 72 survey women. Fewer than half the women reported seeking care within three months of noticing symptoms and about a third waited for a year or more before seeking care.
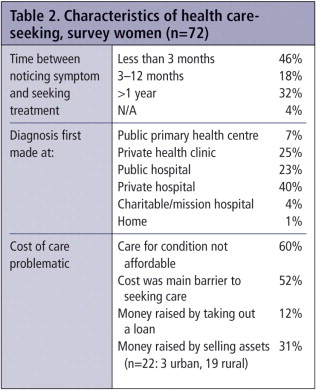
The condition was diagnosed in only 7% of cases at the primary level, 25% at a private clinic, 23% at a public hospital, 40% at a private hospital and 4% at a charitable/mission hospital. This is consistent with findings from the 2003 national survey that women's utilisation of primary health care is limited.Citation25 Yemen's Health Sector Reform strategy 2000 also reports that the lack of essential drugs and services in governmental health centres results in a high primary care bypass rate of 42–73%.Citation34
In discussing barriers to health-seeking for their condition, in addition to the pre-eminent concern about cost, the majority of women spoke of restrictions on their mobility or care-seeking choices due to either financial constraints or social norms.
“During my husband's absence I preferred to seek care from a doctor where we live because I cannot come by myself to Sana'a for treatment.” (First year university, age 24, parity 2, PID)
“I had a ruptured uterus and the shame I felt made it unacceptable to me to be attended by a male doctor. After the rupture I had to have my tubes tied. A male specialist doctor was on duty that night. He could have handled my case better than the female midwife. That was the beginning of my suffering from pelvic inflammation.” (Primary education, age 35, parity 5, PID)
The women in our study were not representative of women in Yemen, given their better than average level of education and the fact that they were able to access health services in Sana'a. This suggests that less well-off women in Yemen face even greater barriers in seeking health care.
Effects on women's daily lives
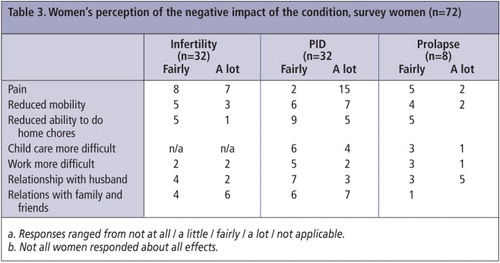
When asked whether their condition had affected their daily lives, almost all women in the survey group reported that they experienced little or no major change. These findings may reflect the limitations of a questionnaire approach, particularly in a context where women tend to expect problems associated with their reproductive health. And in fact, in response to more specific questions the impact on their daily lives was evident (Table 3). With all three conditions, a significant number of women had pain and felt the condition affected relations with husbands and family, ability to work and/or mobility a lot or a fair amount.
Similar findings emerged from the interviews: when asked about their overall health the majority reported they were in good health (all conditions) “Al Hamdu'lillah” (thank God). It is considered a virtue in Yemen not to complain about one's problems and to tolerate hardships. When probed, however, women told a different story. These conditions were largely borne in silence with little or delayed disclosure even to female friends and relatives – sometimes with negative consequences.
“At the beginning the watery discharge was in small amounts, but it increased especially whenever I sat down for washing clothes or making bread. It was really inconvenient. I spent most of the time in and out of the bathroom to clean myself and I started using cloths [tied to relieve the symptoms of prolapse]… I kept all this suffering secret. I didn't tell anybody, neither my daughter nor my daughter-in-law or even my husband. I felt shame to talk about such an issue.” (No education, age 52, parity 8, prolapse)
“I had inflammation. I suffered a lot. I had a pain in my lower abdomen. I also suffered from itching. Intercourse was very painful and a difficult experience for me, which I always tried to avoid. My husband is disappointed with my response to our relationship. He is a farmer, he cannot afford to have a second wife otherwise he could have done it. Thank God he cannot afford to bring a second wife.” (No education, age 23, parity 3, PID)
“The pain I have during intercourse is severe. The good thing is that my husband is an understanding person... I am the only wife. I don't know, maybe my condition and my sickness will make him think about getting another wife.” (Primary education, age 35, parity 5, PID)
“The urine started leaking, involuntarily, sometimes it made a noise, which was very embarrassing. It was even a big problem when I started doing my prayers, the urine started leaking. For that reason I was not able to do my prayers with other women or even in front of anybody. I prayed in a separate room by myself. This problem caused me a lot of discomfort.” (No education, age 50, parity 10, prolapse)
Women's perceptions of the determinants of their condition
When asked about what they perceived to be the cause of their condition, some of the interviewed women with PID said they believed it was iatrogenic – either through IUD insertion or unhygienic delivery practices in hospital.
“I feel that the loop (IUD) caused the problem. Maybe during insertion it was not fixed in its place properly. I was worrying from that point.” (Secondary education, age 25, parity 3, PID)
“I had inflammation after the delivery of my first child. The provider examined me internally to see the measure of the uterus before delivery at least ten times. I think that was the cause of the infection, especially because it was done in an unclean situation.” (University educated, age 24, parity 3, PID)
“Whenever I felt that the uterus came down, I tried to push the organs inside and afterward I tied my abdomen and continued my daily tasks. I feel much better when I lie down with my legs up. This position gives me relief.” (No education, age 52, parity 8, prolapse)
“At the first delivery, I didn't have any problems. I was at my mother's house. She took good care of me. The second and third deliveries were at my husband's house. I didn't have anyone to help me. I had to resume work a few days later. Since then I started having feelings of heaviness down below.” (No education, age 23, parity 3, prolapse)
Physicians' perceptions
The six physicians interviewed confirmed many of the statements of the women. Four of the doctors underlined the importance of basic standards of infection control during IUD insertion, which are often not complied with in Yemen. One doctor with extensive experience treating infertility reported that most cases she saw were of primary infertility,Footnote* but for both primary and secondary infertility, tubal causes were typically due to PID or post-partum sepsis following unhygienic deliveries (at home or in hospitals). This may explain the pain reported by the infertile women in our study.
These doctors also confirmed long delays and hesitation in seeking treatment among women with these conditions, with the exception of infertility.
“For infertility, they come early because of social pressure. For prolapse they only come once the protrusion of the organs starts to make difficulties or cause ulceration. For the others, they also come early if the condition affects their sexual life or if the husband starts complaining, otherwise they live with it.” (Ob-Gyn specialist, 25 years' experience)
“If the woman is a widow or divorced she will not seek treatment because she is not sexually active, and she will live with it the rest of her life.” (GP, 14 years' experience)
The doctor working in an NGO contrasted services in government clinics, where women waiting for treatment sit in one small room. There is no privacy, and to avoid the consultation being heard by the other women, he has to sit close to the woman he is treating. He also complained that in the government clinic the husband has to wait outside, and unlike in the NGO, there is no chance to talk with the couple together: “I think the issue of giving treatment to the wife and asking her to get her husband to have an [STI] test doesn't work in our cultural setting.” (GP, 15 years' experience)
Four of the doctors also mentioned problems of self-administration of antibiotics and the resulting recurrent infections. Two spoke of the challenges of treating infections, particularly PID, in polygamous marriages, where all partners need to be treated at the same time, yet often the husband refuses.
Conclusions
This study found that reproductive morbidity can pose a heavy social and physical burden on women, as well as interfering with domestic and manual work, and provides further evidence that stigma and social norms may contribute to long delays in seeking treatment, leading to more serious sequelae.Citation36–38 Moreover, the barrier of having to raise money to pay for services deserves attention. Our findings are consistent with findings from the Health Sector Reform strategy for Yemen, that out-of-pocket contributions of households to health care costs are as high as 75%, with the government contributing only 25% (the lowest in the Arab region).Citation34
This study has several limitations. Firstly, the results are based on convenience samples in Sana'a that may be subject to selection bias. Although the women had a confirmed diagnosis, we did not have access to medical records on the severity of their conditions and we did not ask about other morbidities. We also did not explore the implications of the sale of assets for the women's households. Since this study was completed, however, we have undertaken a larger and more representative study among married women in Yemen with a focus on health-seeking behaviour.
Even so, certain tentative conclusions emerge regarding the implications of reproductive morbidity for poverty and development in Yemen. Firstly, the Yemeni government needs to ensure that women with few resources are able to access care for these conditions, given its commitment to reproductive health as articulated in the Population Policy, Poverty Reduction Strategy Paper,Citation22 Reproductive Health Strategy and ratification of the Convention on the Elimination of All Forms of Discrimination Against Women.
The capabilities approach can be useful in its focus on individual well-being while also addressing social context. Reproductive morbidity can be seen as causing capability deprivation, in that it constrains participation in both work and normal life, and therefore participation in development for women. Our findings confirm the need to go beyond DALYs to understand the social burden of disease, in that the social consequences of morbidity may in some ways have been more severe for the women than the physical ones and are of great importance for women themselves. There remains, however, the problem of priority-setting (in which DALYs have a comparative advantage) to capture policy attention in a context of scarce resources, limited data on the prevalence of morbidity and where women themselves do not readily articulate their suffering.
Midwife at Madoodha Health Clinic, visited by Oxfam's Mobile Health Unit once a month to see patients with little or no access to health care, Yemen, 2007

As in many other developing countries, reproductive morbidity is not a priority in Yemen, with its limited resources and multiple public health needs. Maternal mortality and family planning are currently priority issues, and reproductive morbidity falls in the grey area between the Reproductive Health Department, the Population Sector of the Health Ministry and the National AIDS Programme. Infertility care, on the other hand, is provided in hospitals under the curative section of the Ministry of Health. Our findings strongly support the argument made by many others (e.g. Pinotti et alCitation39) about the need to develop comprehensive services to address women's health, especially given the multiple morbidities that women experience, rather than the fragmented approaches that currently dominate.
Acknowledgements
Fieldwork for this study was funded by the Economic and Social Research Council (ESRC) support for the Global Poverty Research Group (Universities of Manchester and Oxford) and by a grant from the Middle East/North Africa regional office, Ford Foundation, to the Faculty of Health Sciences, American University of Beirut, Lebanon. The Wellcome Trust (UK) (Grant No. 061495/Z/00/Z) to the Center for Research on Population and Health supported the visit of both Bothaina Attal and Najia Bahubaishi to Beirut for data analysis. We thank Amir Hassan, Liverpool School of Tropical Medicine, and participants at an ESRC-funded workshop on Reproductive Morbidity and Poverty, London School of Economics, November 2010, for comments.
Notes
* DALYs measure disability, interpreted as individual physical suffering, and since infertility is often asymptomatic, it is only included in DALYs as a disabling outcome of sexually transmitted diseases.Citation9
* The questionnaire in English and Arabic and other research tools are available from the first author.
* A study of 1,100 patients at a national centre for infertility similarly found that 78% were cases of primary infertility, but tubal infertility accounted for 41% of infertility in women.Citation35
References
- M Koenig, S Jejeebhoy, S Singh. Investigating women's gynaecological morbidity in India: not just another KAP survey. Reproductive Health Matters. 6(11): 1998; 84–97.
- M Koblinsky, ME Chowdhury, A Moran. Maternal morbidity and disability and their consequences: neglected agenda in maternal health. Journal of Health, Population and Nutrition. 30(2): 2012; 124–130.
- M Koenig, M Shepherd. Alternative study designs for research on women's gynaecological morbidity in developing countries. Reproductive Health Matters. 9(18): 2007; 165–175.
- R Sadana. Measuring reproductive health: review of community-based approaches to assessing morbidity. Bulletin of World Health Organization. 78(5): 2000; 640–654.
- Greene ME, Merrick T. Poverty reduction: Does reproductive health matter?: World Bank, Health, Nutrition and Population Discussion Paper; 2005.
- TKS Ravindran, R Savitri, A Bhavani. Women's experiences of utero-vaginal prolapse: a qualitative study from Tamil Nadu, India. M Berer, TKS Ravindran. Safe Motherhood Initiatives: Critical Issues. 1999; Reproductive Health Matters: London, 166–172.
- KT Storeng, SF Murray, MS Akoum. Beyond body counts: a qualitative study of lives and loss in Burkina Faso after ‘near-miss’ obstetric complications. Social Science and Medicine. 71: 2010; 1749–1756.
- KT Storeng, RF Baggaley, R Ganaba. Paying the price: The cost and consequences of emergency obstetric care in Burkina Faso. Social Science and Medicine. 66(3): 2008; 545–557.
- C Abou Zahr, P Vaughan. Assessing the burden of sexual and reproductive ill-health: questions regarding the use of disability-adjusted life years. Bulletin of World Health Organization. 78(5): 2000; 655–666.
- P Allotey, D Reidpath. Objectivity in priority setting tools: context and the DALY. Reproductive Health Matters. 10(20): 2002; 38–46.
- AK Sen. Capability and Well-Being. 1993; Oxford Scholarship Online Monographs.
- AK Sen. The Standard of Living. 1988; Cambridge University Press: Cambridge.
- AK Sen. Development as Freedom. 1999; Oxford University Press: Oxford.
- MC Nussbaum. Women and Human Development: The Capabilities Approach. 2000; Cambridge University Press: Cambridge.
- J DeJong. Capabilities, reproductive health and well-being: an application of Sen's and Nussbaum's capabilities framework. Journal of Development Studies. 42(7): 2006; 1158–1179.
- P Prah-Ruger. Health capability: conceptualization and operationalization. American Journal of Public Health. 100(1): 2010; 41–49.
- DS Jayasundara. Reproductive health of women in developing countries and human development: a test of Sen's theory. [Unpublished PhD dissertation]. 2009; University of Texas: Arlington.
- H Khattab, N Younis, H Zurayk. Women, Reproduction, and Health in Rural Egypt: The Giza Study. 1999; American University of Cairo Press: Cairo.
- ME Deeb, J Awad, JS Yeretzian. Prevalence of reproductive tract infections, genital prolapse, and obesity in a rural community in Lebanon. Bulletin of World Health Organization. 81(9): 2003; 639–645.
- SM Mawajdeh, R Al-Qutob, A Schmidt. Measuring reproductive morbidity: a community-based approach, Jordan. Health Care for Women International. 24(7): 2003; 635–649.
- R Mabry, A Al-Riyami, M Morsi. The prevalence of and risk factors for reproductive morbidities among women in Oman. Studies in Family Planning. 38(2): 2007; 121–128.
- Republic of Yemen. Poverty Reduction Strategy Paper 2003–2005. (Translated from the original text in Arabic). 2002; International Monetary Fund: Washington, DC. At: www.imf.org/external/np/prsp/2002/yem/01/index.htm. Accessed 15 November 2011.
- World Bank. The Status and Progress of Women in the Middle East and North Africa. 2009; Washington, DC.
- Save the Children. State of the World's Mothers 2007. Saving the Lives of Children Under 5. Westport CT; 2007. At: www.savethechildren.org/site/c.8rKLIXMGIpI4E/b.6153061/k.A0BD/Publications.htm. Accessed 25 June 2007.
- Yemen Ministry of Public Health and Population and Central Statistical Organization. Yemen Survey of Family Health; 2003.
- Gobran J. Growing debate in Yemen in the age of marriage. Al-Akhbar. 26 April 2010.
- B Geyoushi, Z Matthews, W Stones. Pathways to evidence-based reproductive healthcare in developing countries. British Journal of Obstetrics and Gynaecology. 110(5): 2003; 500–507.
- EA Diab. Uterine ruptures in Yemen. Saudi Medical Journal. 26(2): 2005; 264–269.
- B Attal. Quality assessment of birth care in the public and private hospitals in Sana'a city, Yemen. Unpublished PhD dissertation. 2003; Liverpool University.
- AW Al Serouri, A Al Rabee, M Bin Afifi. Reducing maternal mortality in Yemen: challenges and lessons learned from baseline assessment. International Journal of Gynecology and Obstetrics. 105: 2009; 86–91.
- I Dhaifalalah, J Santavy, H Fingerova. Uterine rupture during pregnancy and delivery among women attending the Al-Thawra hospital in Sana'a City, Yemen. International Journal of Gynecology and Obstetrics. 107: 2006; S2, S155.
- N Bahubaishi. Assessment of the quality of care and utilisation of family planning services in Sana'a City. Unpublished PhD dissertation. 2007; Liverpool University.
- World Health Organization. WHO Quality of Life-Brief. At: www.who.int/substance_abuse/research_tools/whoqolbref/en/
- Ministry of Public Health. Government of Republic of Yemen. Health Sector Reform in the Republic of Yemen: Strategy for Reform. 2000; Sana'a.
- I Dhaifalah. Infertility in Yemen: The first steps [Lecture Presentation]. 2011; University Hospital Olomouc. At: http://ulgrs.upol.cz/portalen/wp-content/uploads/2011/01/lecture_Infertility-in-Yemem-Dhaifalah-.pdf
- RA Bang, AT Bang. Why women hide them: rural women's viewpoints on reproductive tract infections. Journal about Women and Society. 1992; 27–30. Cited in [38].
- J Bhatia, J Cleland. Methodological issues in community-based studies of gynaecological morbidity. Studies in Family Planning. 31(4): 2000; 267–273.
- M Rani, S Bonu. Rural Indian women's care-seeking behavior and choice of provider for gynecological symptoms. Studies in Family Planning. 34(3): 2003; 173–185.
- JA Pinotti, MLVAA Tojal, ACT Nisida. Comprehensive health care for women in a public hospital in Sâo Paulo, Brazil. Reproductive Health Matters. 9(18): 2001; 69–78.