Sexually transmitted infections (STIs) are a major global cause of acute illness, infertility, long-term disability and death with serious medical and psychological consequences for millions of men, women and infants. There are over 30 bacterial, viral and parasitic pathogens that have been identified to date that can be transmitted sexually. Quantifying the incidence and burden of these infections is important for planning appropriate interventions and advocating for resources, as necessary. This report presents global and regional estimates for 2008 of the incidence and prevalence of four curable STIs – Chlamydia trachomatis, Neisseria gonorrhoeae, syphilis and Trichomonas vaginalis – in adults between 15 and 49 years of age. These estimates were generated using the same approach as used to generate the 2005 global estimates.Footnote*
The 2008 regional prevalence estimates were based on data collected from a series of PubMed searches and complemented by published and unpublished studies brought to the team's attention. The last PubMed search was carried out on 15 September 2011.
Global estimates
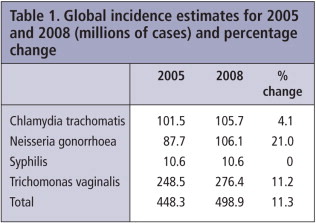
The total number of new cases in adults of the four STIs in 2008 was estimated to be 498.9 million.
| • | 105.7 million cases of C. trachomatis | ||||
| • | 106.1 million cases of N. gonorrhoeae | ||||
| • | 10.6 million cases of syphilis | ||||
| • | 276.4 million cases of T. vaginalis. | ||||
Males accounted for 266.1 million or 53% of the new cases.
At any point in 2008 it was estimated that the number of adults infected with each infection was:
| • | 100.4 million with C. trachomatis | ||||
| • | 36.4 million with N. gonorrhoeae | ||||
| • | 36.4 million with syphilis | ||||
| • | 187.0 million with T. vaginalis. | ||||
The number of adults with one or more infections, however, is less than the sum of the four infections as some individuals will have had multiple infections.
Regional estimates for the four selected STIs
WHO African Region Total incidence in 46 countries with an estimated population in 2008 of 384.4 million adults between the ages of 15 and 49 = 92.6 million
WHO Region of the Americas Total incidence in 35 countries with an estimated population in 2008 of 476.9 million adults between the ages of 15 and 49 = 125.7 million
WHO South-East Asia Region Total incidence in 11 countries with an estimated population in 2008 of 945.2 million adults between the ages of 15 and 49 = 78.5 million
WHO European Region Total incidence in 53 countries with an estimated population in 2008 of 450.8 million adults between the ages of 15 and 49 = 46.8 million
WHO Eastern Mediterranean Region Total incidence in 23 countries with an estimated population in 2008 of 309.6 million adults between the ages of 15 and 49 = 26.4 million
WHO Western Pacific Region Total incidence in 37 countries with an estimated population in 2008 of 986.7 million adults between the ages of 15 and 49 = 128.2 million
Discussion
The 2008 incidence estimates for C. trachomatis, N. gonorrhoeae, and T. vaginalis are slightly higher than the equivalent figures for 2005. These apparent increases may be the result of a number of factors including the increasing number of youths entering the sexually active population each year, social changes that are conducive to the spread of STIs, and changing patterns in prevention and treatment practices.
There is, however, a great deal of uncertainty surrounding the global and regional STI estimates. If these uncertainties are to be reduced a determined effort is needed to obtain relevant data, in particular:
| • | Prevalence data – there is a shortage of good quality prevalence studies. Specifically, there is a need for data from low risk urban and rural populations, disaggregated by age and sex; and for strengthened routine STI surveillance for incidence monitoring. | ||||
| • | Estimates of the duration of infection – the average duration of infection for a pathogen depends upon the pathogen, the health care seeking behaviour of the population, and access to health care. Information on all three of these factors is very limited, leading to imprecise estimates of the duration of infection. | ||||
These data have an important role to play in improving our understanding of the burden of these infections. They are also crucial in helping improve the design and implementation of STI interventions and in lobbying for further resources and political support. Worryingly, the number of prevalence data points that met the 2008 study entry criteria was less than half the number that met the equivalent 2005 entry criteria.
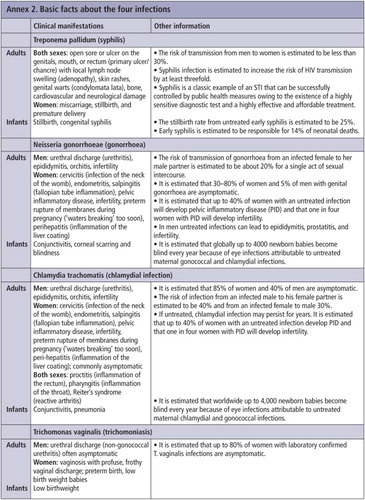
The number of new infections from these four infections highlights the global health problem posed by STIs in general. The direct clinical manifestations of STIs are uncomfortable for those affected, and if they are left untreated, can result in serious complications and sequelae (see Annex 2 next page for some of the complications of the four infections included in this publication). Growing resistance to the common treatment regimens is further compounding the problem.
STIs, apart from HIV, however, are not viewed as a public health priority. STI surveillance and STI prevention and treatment programmes are generally poorly resourced and staffed. This needs to be remedied. These actions will also help support the attainment of Millennium Development Goals 4, 5 and 6 by reducing infant mortality, improving maternal health, and reducing the incidence of HIV. But this will require a concerted effort by national governments, international organizations, funding agencies and individuals. New funding will need to be mobilized and mechanisms put in place to ensure that resources are used efficiently and effectively.
Note
Excerpted from the full report with kind permission of the WHO Department of Reproductive Health and Research. The full report and additional information are available online at: http://apps.who.int/iris/bitstream/10665/75181/1/9789241503839_eng.pdf
Notes
* See Prevalence and incidence of selected sexually transmitted infections, Chlamydia trachomatis, Neisseria gonorrhoeae, syphilis and Trichomonas vaginalis. Methods and results used by WHO to generate 2005 estimates. Geneva, WHO, 2011, for a detailed description of these methods.