“These are our bottom lines… We are counting on all governments to have the courage to champion the ‘controversial’ issues by addressing the difficult realities, many of which are related to the root causes of inequalities… 1. Keep your Promises. 2. Champion our Sexual Rights. 3. We Demand Economic Justice. 4. Leave us a Healthy Planet. 5. We are Stakeholders, not a Target Group.” (Post-2015 Consultation Youth Statement, October 2013)Footnote1
What a wordstorm the ICPD Beyond 2014 and Post-2015 Sustainable Development agendas have unleashed! What a tsunami of consultations, meetings, reports, statements, shopping lists of wishes and demands, and overflowing expectations has been pouring in from every corner of the globe! I don’t know how the UN Secretary-General deals with it, but my inbox can barely cope. On the other hand, this storm has brought in a treasure trove of comments, policy analysis and critiques, which I’d like to share with you. And the same is true of the excellent papers in this journal issue.
There are two issues I want to emphasise in this editorial which, together, reflect the crux of what this journal issue is about and what I think is going on in the world beyond the verbal explosion:
We have the opportunity to articulate sustainable development goals which avoid the many limitations of the MDGs and broaden the remit of responsibility and commitment to improving global health and human rights. These must of course include health, gender equality, and sexual and reproductive health and rights. There is strong evidence, however, including in these pages, that efforts to implement gender equality are only barely succeeding, and many governments are grossly under-funding health in spite of existing, long-standing commitments, particularly in Africa,Footnote2 though Africa is far from alone. The new goals need to be configured in the recognition that they are inter-dependent and must be based in a human rights approach, which means no one can be left out. Until this commitment can be achieved in principle, a new development paradigm and with it new goals will remain an aspiration that cannot be expected to succeed. | |||||
The MDGs on health scuppered the focus on comprehensive sexual and reproductive health and rights (SRHR) articulated officially for the first time in the ICPD Programme of Action, and MDG5 pretty much narrowed the agenda to reducing maternal mortality, to the detriment of almost all other SRHR issues. Maternal mortality has fallen but not enough and not at all in the poorest countries, while skilled attendance at birth has not risen concomitantly. We SRHR advocates are faced with a number of urgent problems. Specific aspects of health will not become goals, SRHR certainly not. So how can we ensure, this time around, that sexual and reproductive health and rights as a whole get included in the post-2015 sustainable development goal for health, along with all the other pressing health and development issues being championed by others? | |||||
Who is taking the leadership in our movement this time round? Do we have a plan? A strategy?
Some of these issues/questions are immediately outward-looking. They demand global, national and local action from the inter-governmental, governmental, donor, health system and health policy communities, as well as civil society, ultimately looking for solutions at country level. Others are initially inward-looking. We in the SRHR advocacy community are brilliant at articulating our issues and what is needed to achieve them if only…. But we sometimes seem to get stuck there. The opposition to our issues is not getting any weaker. What will be included under all the goals is being debated and negotiated at all levels, right now, within a complex network of players, and those of us who are expert at this work need to be in there as the list of goals and their details are drawn up, negotiated and re-negotiated, every day between now and 15 September 2015. Even more of us should be negotiating at country level with our national leadership. Are enough of us doing this right now? How do we get a consensus among us as to what, besides SRHR and gender equality, our community supports and is fighting for in the wider arena? ICPD was anything but a doddle, but it looks like child’s play by comparison to this.
A new development paradigm on health: what should it look like
What is the new development paradigm everyone I know is calling for? What should the health goal be so that it does not narrow down the aspiration of “health for all” but promotes it? What health goal would be an appropriate home for our issues? The World Bank supports “universal health coverage” (UHC) as the health goal. The World Health Organization did as well, at least until recently, though some have reported that they are beginning to think it should treated as a means, but not as the goal itself. I hope that view prevails and that the Bank comes to see it that way too. One UK-based network defines the core components of UHC to include “universal access to quality health services that match the needs of the population and respond to country-specific disease burdens; and universal financial risk protection that eliminates cost as a barrier to accessing health care”. They add that “international support to overcome legal and political barriers to health access for the poorest and most marginalised” must also be provided.Footnote3
That definition sounds very, very good potentially, but isn’t the real point of UHC the “coverage” side mainly, that is, how is health care paid for? Isn’t that another form of narrowing the agenda? And what is/are the model(s) for ensuring coverage? For example, consider the conclusion of a case study published this year of Mexico’s considerable efforts to implement a version of UHC: “When it comes to health care in Mexico, ‘universal’ has never meant equal, particularly when it comes to access to adequate care for the country’s 52 million uninsured.”Footnote4 This outcome, that the most vulnerable are the worst served, may be the unintended result of the “inverse equity hypothesis”,Footnote5 that is, when new programmes are rolled out, the rich get the benefit first, and inequity and inequality increase unless specific measures are taken to prevent them. UHC is apparently meant to stop inverse equity from occurring, but according to Gita Sen, citing Davidson Gwatkin, there is as yet no evidence as to whether UHC can and will indeed deliver on avoiding this problem (Gita Sen, Presentation, UNFPA consultation on women’s health, Mexico City, October 2013).
Hence, there are potentially important weaknesses in both the comprehensiveness and implementation of universal health coverage – and as Gita Sen points out, this will include inequity of access due to gender inequalities as well. She has also raised the question of what “coverage” assumes in terms of the strengths and weaknesses of specific health systems, which can affect their ability to implement universal programmes in the first place (Gita Sen, Presentation, UNFPA consultation, Mexico City, October 2013). Moreover, UHC does not encompass within itself, at least as conceived to date, a rights-based approach nor a focus on all the other determinants of health in addition to health services.
And hence, it would appear that universal health coverage is not the answer. I find it worrying, however, that I have heard almost no views at all on this question from my SRHR colleagues one way or the other, though many of us agreed in Mexico City that it was urgent we talk about it. So I’m very glad to be able to publish a paper on it, with an SRHR perspective, in this journal issue.
Another worrying issue, before UHC can be put to bed, are some apparently unchallenged assumptions about “coverage” in relation to private vs. public ownership and control of health care — and of health care financing — underlying different concepts of UHC. For example, the question of who owns the means of financing health care, let alone the means of providing health care itself, are, as far as I can judge, the elephant in the room. The current hegemonic assumption of the need for private sector involvement in health care and health care financing, for example, remains to be challenged. Where does the SRHR movement stand on this issue, given the extent to which SRHR services are privatised, that is, provided outside the public health system, in most countries today? The weaknesses of governments and their limited ability to develop, staff and run good quality health systems, let alone their other social welfare, education and economic responsibilities, are undeniable. But isn’t that a direct and deliberate consequence of national and international policy, not an immoveable fact of life?
A 2012 paper by London & SchneiderFootnote6 argues that “while neoliberal globalisation is associated with increasing inequalities, global integration has simultaneously strengthened the dissemination of human rights discourse across the world”. They explore the “seeming contradiction” that “globalisation is conceived as disempowering nation states' ability to act in their populations’ interests, yet implementation of human rights obligations requires effective states to deliver socio-economic entitlements, such as health. Central to the actions required of the state to build a health system based on a human rights approach is the notion of accountability.”
So before we talk about what the health goal should be, the prior question is how to develop effective states that are able to deliver entitlements such as to health. London & Schneider call for the strengthening of national parliamentary oversight, to prioritise pro-poor protections and increase leverage for resources for the health sector within parliamentary processes, and for civil society action to hold public officials accountable and enable civil society mobilization. They also call for a critical assessment of state incapacity to meet claims to health rights, and point out that this raises questions as to “the diffusion of accountability rife under modern international aid systems”.Footnote6 Thus, the role of international aid also needs to come under the microscope. If we wish to create new paradigms, there’s a lot of groundwork to be done first.
A third issue is whether civil society, including SRHR advocates, is strong and resourced enough to be able to hold international agencies and governments to account. As a 2010 global survey by AWID of over 1,100 women’s organisations showed, there’s not much money in the kitty. The survey found that “vast resources are becoming available under the broad umbrella of development” but although there is significant interest in investing in women and girls individually, funding for women’s organisations is negligible. In 2010, the median annual income of over 740 women’s organizations around the world was only US $20,000. AWID also points out that while “mechanisms and sources of development financing and philanthropy are becoming increasingly diversified, economic growth and return on investment are the priority, with human rights and well-being taking a back seat” and “private sector interest in and approaches to development, philanthropy and women and girls infiltrating traditional development and funding sectors”.Footnote7 Does the SRHR community have a view on these changes? What do we need in the way of human and other resources to succeed in the role of holding governments and donors accountable? Are we currently strong enough at the country level especially to do this? How are the health policy and health rights movements more broadly responding to this? When will we all start working together?
AWID and many others among us are concerned that human rights have been made “contentious” and are being pushed to a back seat. The world cannot afford for human rights to take a back seat if it’s serious about development, however. Nor can the world afford to depend on companies like Coca-Cola to help the Tanzanian Ministry of Health and the Global Fund to Fight AIDS, TB and Malaria to improve the country’s national supply chain so that essential medicines can reach remote areas,Footnote8 presumably alongside great quantities of a very unhealthy soft drink. This example of a so-called public-private partnership, presumably funded from the profits from that unhealthy soft drink, is surely an unethical undertaking, in spite of frustration with national health system weaknesses. Yet such partnerships are on the rise in both development and humanitarian work, as more companies seek new sources of influence, profit and power, cloaked in the credibility of “philanthropy”. Despite soaring profits from unhealthy food, nutrition remains a crucial global problem, manifested in both malnutrition and obesity, with major health consequences such as diabetes and high blood pressure. “Big food” is as important a global health issue as “big pharma”. Malnutrition is an issue of poverty, unemployment, and damaging agricultural policies. Intersectoral collaboration that is pro-poor could ameliorate some of the poor health outcomes that the health sector ends up having to deal with (Gita Sen, Presentation, UNFPA consultation, Mexico City, October 2013).
And as we are talking new paradigms, what about the seemingly impossible goal of eliminating poverty, the least achieved goal of the MDGs, but still an overarching goal of the sustainable development goals? The 2008 report of the WHO Commission on the Social Determinants of Health,Footnote9 affirmed that “social injustice was killing on a grand scale, with a toxic combination of ‘poor social policies and programmes, unfair economic arrangements, and bad politics’ being responsible for producing and reinforcing health inequalities. [The report] provides a comprehensive, evidence-based picture of pervasive inequalities in health in many countries, demonstrating the presence of a social gradient in health outcomes associated with the unfair distribution of the social determinants of health.”Footnote10 In other words, the richest 20% don’t want the poorest 40% to get what they’ve got, do they? What’s the strategy for addressing that barrier? Does the global leadership at both UN and governmental level have a strategy for that?
This brings me back to the crux of the issue: the need to emphasise both UN and UN Member States’ responsibilities for improving the health of their populations and for respecting, protecting, and fulfilling the right to the highest attainable standard of health. States can’t do this alone, especially not those with low tax bases and incomes, weak infrastructure, poor financial management, and politicians in charge who are corrupt, don’t give a toss about or don’t support internationally agreed goals themselves. Nor can national governments really expect the help they need to come from external funding sources with their own agendas (i.e. tax avoidance, trade advantages, political influence and security concerns) and are actually operating a contemporary version of neo-colonialism and treating countries like dependents.
So, speaking as a public health and human rights advocate, my answer to the question of what the sustainable development goal for health should be is this: first, we need a transformative development paradigm anchored in human rights and a new global and national economic order, grounded in the recognition of pressing environmental issues that require urgent global action on the part of every country, especially those polluting our planet the most. Then, within a broad human rights approach to all the sustainable development goals, of the options on the table for the health goal:
Universal health coverage | |||||
Health for all by (fill in date) | |||||
Some weedy ideas about fulfilling human well-being, or | |||||
The right to the highest attainable standard of health (“the right to health”) | |||||
the choice seems quite clear. Having rejected UHC, the “right to health” is the only one on this list that makes any sense at all. “Health for all” is optimistic, inclusive and aspirational, as it was when Halfdan Mahler made it the slogan of the World Health Organization, with the aim of achieving health for all by the year 2000. I liked it then and I like it now, but it’s a slogan, and not heavy-duty enough as a sustainable development goal, which has to be complex if it’s to be any good but also needs clear delimiting and a base in human rights. My vote, hands down, is for the “right to health”. And to enforce it, as opposed to continuing to treat it as aspirational, I think the Joint Action and Learning Initiative’s proposal of a framework convention on health, summarised in a paper here, is worth exploring. The “right to health” has been included in a number of UN human rights documents, starting with the Universal Declaration of Human Rights in 1948. Today, given how difficult it has proved to achieve, I think the “right to health” deserves its own convention and a mechanism for holding States parties accountable for implementing it.
Moreover, there are a substantial number of UN covenants and conventions, all of which are legally binding on States,Footnote11 as well as several non-binding commitments,Footnote12 all of which have been ratified by the great majority of States. They need a huge amount of work to be made operative in countries. Why don’t we use them more as sources of goal-setting – much of the world has already agreed to them. Finally, there is the Universal Periodic Review of the Human Rights Council, which involves a review by UN Member States of the human rights records of Member States, and provides the opportunity for each State to declare what actions they have taken to improve the human rights situations in their countries and fulfil their obligations.Footnote13 Surely this should be included as part of the accountability process at global level.
Moreover, there would be great value in increasing the visibility and responsibility of the already existing UN-appointed bodies whose task it is to hold everyone accountable for implementing these commitments, at both global and regional levels.Footnote14
As for our movement ensuring that SRHR is included as an integral part of the health goal, I can only reiterate the obvious – it requires advocacy, negotiation and involvement in the larger global health policy agenda, and working with the broader health policy, right-to-health and development movements, as well as within SRHR and gender equality advocacy networks. I doubt anyone needs reminding that building networks at national level, which engage with national policymakers and parliamentarians, and with national leaders who will be involved in the global agenda, is at least as important as haunting the corridors of the UN week after week. Consigning politicians and religious leaders to history whose stance against sexual and reproductive health and rights is detrimental to the public health is also a crucial task. Moreover, as shown in these pages, a huge task remains to convince and garner support from those who say they support women and girls, or believe in (some) rights, but whose actual policies lead to headlines such as this: “Canada slams war rape; abortion stance murky.”Footnote15
Papers in this journal issue
The papers in this journal start with the history of the global consensus achieved with the ICPD Programme of Action in 1994, presented in an international consultation on human rights in July 2013 by Nafis Sadik. Others describe the road that led to the Millennium Development Goals (MDGs) in 2000, and critique the strengths and shortcomings of MDG targets and indicators, their intended and unintended consequences, and the limited measures that have been used, such as definitions of accountability, to take the development agenda forward. A number of the papers contain country case studies; they look at national research data and specific policies; they expose and critique weaknesses in budgets, expenditure and sources of funding. They show the disconnect between international agreements and country-level realities. One makes it clear that the move of childbirth out of the forest into the home has been an important step forward for women, MDG targets notwithstanding. These are in-depth, hard-hitting, thought-provoking papers, and their messages are worth taking on board. Still others look at what the parameters are for determining the sustainable development goals and the future. They discuss what the new development framework must address, and using words like “transformational”, they demand a better world.
Perhaps the most important message for SRHR advocates published here is this:
“Going forward, there is likely to be a strong emphasis on environmental and sustainable development, the first two pillars of Rio+20, as opposed to the third pillar of social development, as happened in Rio… when negotiations became difficult. Governance concerns, sexual and reproductive health and rights and accountability modalities all got pushed aside. A further caveat that tempers the optimism engendered by the new UNFPA framework is the “cautious” approach to language on sexual and reproductive health and rights in several recent reports, which do not move beyond the language of ICPD. Thus, the stage is set for future negotiations. The process leading up to the post-2015 development agenda is complex, but many… people want to see sexual and reproductive health and rights included as a priority in the new sustainable development goals. There is no option other than to move forward within the modalities being set at the highest levels. The one thing we cannot afford to allow again is what happened with the MDGs in 2000; this time, we must not leave the room empty-handed. (Haslegrave)
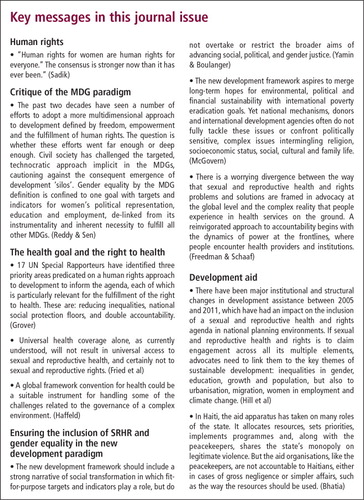
Teacher reads to children at Los Amiguitos de Membol, a nursery school in a poorneighbourhood of Guayaquil, Ecuador, 2009

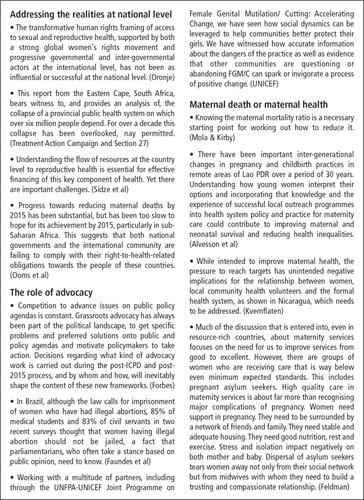
A little girl has just received her birth certificate from the Urban Law Centre, run by the Committeefor Legal Aid to the Poor, Orissa district, India.

Notes
2 “Twelve years after African governments pledged in the Abuja Declaration to allocate at least 15% of their annual budgets to health care by 2015, just six countries had met this goal… Moreover, about a quarter of African Union member states have regressed and are now spending less on health than they were in 2001.” African governments still underfunding health. Irin News. 23 July 2013. http://www.irinnews.org/report/98459/african-governments-still-underfunding-health.
3 Network of UK-Based Global Health Networks. Draft Policies for Global Health in Party Manifestos, source unknown.
4 Ocejo A. Health, Citizenship, and Human Rights Advocacy Initiative: Improving Access To Health Services in Mexico. International Budget Partnership Impact Case Study No. 15, July 2013. http://papers.ssrn.com/sol3/papers.cfm?abstract_id=2326607.
5 Victora CG, Vaughan P, Barros FC, et al. Explaining trends in inequities: evidence from Brazilian child health studies. Lancet 2000;356(9235):1093–98.
6 London L, Schneider H. Globalisation and health inequalities: can a human rights paradigm create space for civil society action? Social Science & Medicine 2012;74(1):6–13.
7 Arutyunova A, Clark C. Watering the Leaves, Starving the Roots: The Status of Financing for Women's Rights Organizing and Gender Equality. Association for Women’s Rights in Development. 2013. http://www.awid.org/Library/Watering-the-Leaves-Starving-the-Roots.
8 Irin. Global Analysis: What future for private sector involvement in humanitarianism? 26 August 2013. http://www.irinnews.org/report/98641/analysis-what-future-for-private-sector-involvement-in-humanitarianism.
9 World Health Organization. Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health. Geneva: WHO; 2008. www.who.int/social_determinants/final_report/.
10 Marmot M, Bell R. Fair society, healthy lives. Public Health 2012;126(Suppl. 1):S4–10.
11 International Convention on the Elimination of All Forms of Racial Discrimination 1965; International Covenant on Civil and Political Rights 1966; International Covenant on Economic, Social and Cultural Rights 1966; Convention on the Elimination of All Forms of Discrimination Against Women 1979; Convention against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment 1984; Convention on the Rights of the Child 1989; International Convention on the Protection of the Rights of All Migrant Workers and Their Families 1990; Convention on the Rights of Persons with Disabilities 2008.
12 E.g. the Vienna Conference on Human Rights Declaration and Programme of Action (1993), ICPD Programme of Action (1994), and Beijing Platform for Action (1995), as well as Rio+20 The Future We Want.
13 UN Human Rights, Office of the UN High Commissioner for Human Rights. Universal Periodic review. http://www.ohchr.org/EN/HRBodies/Upr/Pages/UPRMain.aspx.
14 Three regional human rights treat bodies (Europe, InterAmerica, Africa), two regional human rights courts (Europe, Inter-America), treaty monitoring bodies (e.g. CEDAW), special rapporteurs (including on the right to health), specialised agencies for monitoring (e.g. WHO, UNFPA, UNAIDS), policy-setting bodies such as the Commission on the Status of Women and Commission on Population and Development, Human Rights Council, Office of the UN High Commissioner for Human Rights – and no doubt I’ve left many more out.
15 Ditchburn J. Canada slams war rape, abortion stance murky. Canadian Press, 27 September 2013. http://globalnews.ca/news/869355/canada-slams-war-rape-abortion-stance-murky/.