
Abstract
Despite broad grounds for legal abortion in Zambia, access to abortion services remains limited. Pharmacy workers, a primary source of health care for communities, present an opportunity to bridge the gap between policy and practice. As part of a larger operations study, 80 pharmacy workers, both registered pharmacists and their assistants, participated in a training on medical abortion in 2009 and 2010. Fifty-five of the 80 pharmacy workers completed an anonymous, structured training pre-test, treated as a baseline questionnaire; 53 of the 80 trainees were interviewed 12–24 months post-training in face-to-face interviews to measure the retention of information and training effectiveness. Survey questions were selected to illustrate the principles of a harm reduction approach to unsafe abortion. Bivariate analysis was used to examine pharmacy worker knowledge, attitudes and dispensing behaviours pre-training and at follow-up. A higher percentage of pharmacy workers reported referring women to a health care facility between surveys (47% to 68%, p = 0.03). The number of pharmacy workers who reported dispensing ineffective abortifacients decreased from baseline to end-line (30% to 25%) but the difference was non-significant. However, study results demonstrate that Zambian pharmacy workers have a role to play in safe abortion services and some are willing to play that role.
Résumé
Malgré de vastes motifs d’avortement légal en Zambie, l’accès aux services d’avortement demeure limité. Les pharmacies, sources primaires de soins de santé pour les communautés, offrent la possibilité de combler l’écart entre les politiques et la pratique. Dans le cadre d’une étude plus large sur les opérations, 80 employés de pharmacie (pharmaciens agréés et leurs assistants) ont participé à une formation sur l’avortement médicamenteux en 2009 et 2010. Avant la formation, 55 des 80 employés ont complété un test structuré et anonyme, traité comme questionnaire de référence ; 53 des 80 apprenants ont été interrogés 12–24 mois après la formation dans des entretiens de suivi en face à face pour mesurer la rétention de l’information et l’efficacité de la formation. Les questions de l’enquête ont été sélectionnées pour illustrer les principes de l’approche de réduction des risques de l’avortement clandestin. Une analyse bivariée a été utilisée pour examiner les connaissances, les attitudes et les comportements de dispensation des employés de pharmacie avant et après la formation. Un pourcentage plus élevé d’employés ont répondu qu’ils avaient orienté des femmes vers des centres de soins de santé entre les enquêtes (47% à 68%, p = 0.03). Le nombre d’employés ayant indiqué qu’ils avaient dispensé des produits abortifs inefficaces a diminué entre les chiffres de référence et les données finales (30% à 25%), mais la différence était non significative. Néanmoins, les résultats de l’étude démontrent que les employés de pharmacie zambiens ont un rôle à jouer dans des services d’avortement sûr et que certains sont prêts à l’assumer.
Resumen
A pesar de que el aborto es permitido por amplias causales en Zambia, el acceso a los servicios de aborto continúa siendo limitado. El personal de farmacias, una fuente principal de servicios de salud para las comunidades, presenta una oportunidad para llenar la brecha entre políticas y práctica. Como parte de un estudio más extenso de operaciones, 80 trabajadores de farmacias, tanto farmaceutas titulados como sus asistentes, participaron en una capacitación sobre aborto con medicamentos en los años 2009 y 2010. Cincuenta y cinco de los 80 trabajadores de farmacias contestaron un examen preliminar estructurado anónimo, el cual fue tratado como cuestionario de línea base; 53 de las 80 personas que recibieron capacitación fueron entrevistadas cara a cara 12 a 24 meses después de la capacitación, con el fin de medir la retención de información y eficacia de la capacitación. Las preguntas de la encuesta fueron seleccionadas para ilustrar los principios de un enfoque de reducción de daños con relación al aborto inseguro. Se utilizó el análisis bivariado para examinar los conocimientos, actitudes y comportamientos del personal de farmacias relacionados con despachar medicamentos, antes de la capacitación y durante el seguimiento. Un mayor porcentaje de trabajadores de farmacias informaron referir a las mujeres a una unidad de salud entre encuestas (47% al 68%, p = 0.03). El número de trabajadores de farmacias que informaron despachar abortivos ineficaces disminuyó desde la línea base hasta la línea final (30% al 25%), pero la diferencia fue insignificante. Sin embargo, los resultados del estudio demuestran que los trabajadores de farmacias en Zambia pueden desempeñar un papel en la prestación de servicios de aborto seguro, y algunos están dispuestos a hacerlo.
Despite the broad grounds for legal abortion in Zambia permitted under the Termination of Pregnancy Act of 1972,Footnote* safe abortion services have not been widely available. Unsafe abortion – the termination of an unintended pregnancy either by persons lacking the necessary skills or in an environment lacking the minimal medical standards, or by both – continues to contribute to maternal mortality and morbidity, killing approximately 47,000 women annually worldwide.Citation1 In Zambia, the maternal mortality ratio is 591 deaths for every 100,000 live births; it is estimated that 30% of these deaths are due to unsafe abortion.Citation2–4 Recognizing this problem, the Zambian government and Ministry of Health (MOH) initiated a national strategic assessment of unsafe abortion in 2008 that resulted in a recommendation for the piloted introduction and evaluation of the feasibility and acceptability of safe abortion services.
Access to legal abortion services in Zambia has been limited primarily to urban women who can afford private health care services. The national assessment identified a number of barriers to safe abortion care, including a shortage of trained medical personnel, a fragmented approach to expanding services, a lack of awareness about the dangers of unsafe abortion, limited scope of practice for nurses and midwives, negative attitudes and behaviours among service providers, women’s limited information regarding the legal status of abortion, a limited number of health facilities that perform abortions, and social and religious sentiment against abortion.Citation5
In Zambia, and in many other parts of the world, herbs and traditional medicines have customarily been used to induce abortion and this has proven a difficult practice to change with legal reform alone.Citation6 Pharmacy workers and drug sellers often bridge the gap between policy and practice in their role as community-based confidants and informants, and play an integral part in information dissemination about abortion.Citation7,8 By providing advice about health issues, access to medications, and direct service provision, pharmacies serve as a first source of health care to individuals.Citation7 Pharmacies offer convenience, geographic accessibility, relative anonymity, short waiting times, and relatively inexpensive services compared to that of other health care providers in the formal health system. These advantages may be especially important to people seeking medications for stigmatizing conditions, such as sexually transmitted infections, and for contraception, emergency contraception, and abortion.Citation7 This research provides initial information on whether Zambian pharmacy workers, both registered pharmacists and pharmacy technologists,Footnote* after a one-day training session, are more receptive to selling medication for abortion, to increasing their knowledge of and willingness to sell this medication, and provide information to those asking about or seeking abortion.
Testing a harm reduction approach with pharmacy workers
Survey questions were selected to illustrate the principles of a harm reduction approach to unsafe abortion. Harm reduction is an evidence-based public health and human rights approach to prioritize strategies that reduce harm where policies and practices prohibit, stigmatize and otherwise drive practices underground. The concept of harm reduction was first developed by practitioners working with intravenous drug users to promote interventions such as needle exchanges, which were considered illegal but are effective in preventing transmission of HIV and other blood-borne infections. This approach has also been used to promote home delivery kits in rural areas, and interventions to protect the rights and health of sex workers, even though sex work may be illegal.
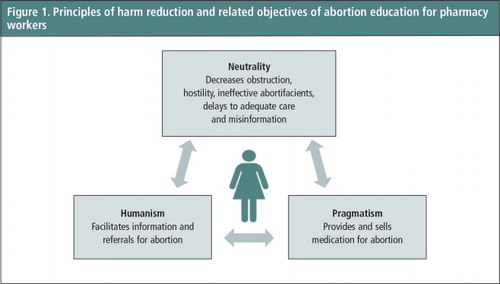
A harm reduction approach to unsafe abortion seeks to reduce abortion-related mortality and morbidity despite the legal setting, by making abortions safer.Citation8,9 The strategy is valuable for countries or contexts where abortion is prohibited or heavily stigmatized, and was first posited by legal scholar Joanna Erdman.Citation9 The three core principles of harm reduction, as posited by Erdman () – neutrality, humanism and pragmatism – were used to create a conceptual framework for analyzing the effects of training on abortion for pharmacy workers.Citation9 The principle of neutrality includes refraining from negative judgments and creating obstruction, and would be demonstrated by improved attitudes, willingness to share information about abortion and a decreased likelihood of providing misinformation. The principle of humanism was measured by increased willingness to address requests related to abortion with accurate information and referrals to services. Finally, pragmatism, the view that women will engage in unsafe abortion and eradication is likely impossible, was demonstrated by the direct provision of medical abortion pills.
Figure 1 Principles of harm reduction and related objectives of abortion education for pharmacy workers
Methodology
The research reported here was conducted as part of a larger multi-faceted operations study evaluating the introduction and scale-up of legal abortion services with manual vacuum aspiration and medical abortion in 28 health facilities in Lusaka and the Copperbelt Province between May 2009 and December 2012. A further objective of the study was to explore the dissemination of new information, particularly by examining the interactions between pharmacy workers, community members and clinicians. A total of 121 clinical trainees, 80 pharmacy trainees, and eight community-based organizations worked to increase the availability and awareness of safe abortion services through service delivery improvements and the introduction of medical abortion with mifepristone and misoprostol. In all, 80 Zambian pharmacists and pharmacy assistants (called pharmacy workers after this) participated in a one-day training session on medical abortion in May, June and August 2009 and May 2010 – including knowledge, clinical updates, referrals for abortion, and abortion values clarification activities. Of the 80, 55 filled in a structured questionnaire about medical abortion stocking and dispensing behaviours, abortion referral practices, attitudes toward clients seeking information on abortion and retention of clinical information for safe self-induction. Findings from interviews with 53 of the original 80 pharmacy workers were conducted 12–24 months later, in order to study the efficacy of the training in line with all three forms of harm reduction. The results of this component of the research are presented here.
More specifically, the training covered medical abortion drugs for gynaecological indications, with a focus on induced abortion. It also included information on the need for empathetic treatment of people seeking information about pregnancy termination and provision of referrals to health facilities for safe abortion services for women who needed this information. In addition to encouraging the direct-to-client sales of misoprostol (mifepristone only became available in Zambian pharmacies during the intervention), a referral system between community members, pharmacy workers, and health workers was developed to close gaps in the service provision of medical abortion pills. Prior to the intervention, most pharmacists had access to misoprostol (Cytotec) in some form, some sold ineffective abortifacients and others carried pills imported from China, known locally as “the Chinese pill” in a variety of dosages. The first importation of mifepristone for limited facility-based, public sector use was released in July 2010. Early in 2012, an international non-governmental organization was able to procure the first shipment of a pre-packaged combined mifepristone and misoprostol package (Medabon) to begin sales to interested pharmacies in the country.
After consulting with the Pharmaceutical Society of Zambia, pharmacies in the study intervention areas that had at least one registered pharmacy worker in the facility were invited to participate in a training session. Fifty-five of 80 pharmacists who were trained in 2009 and 2010 completed an anonymous, structured training pre-test, which was treated as a baseline questionnaire; 53 of the 80 training participants were located and interviewed 12–24 months post-training in face-to-face interviews, to measure the retention of information and the effectiveness of the training. Although all of the pharmacy workers had participated in a training group, the baseline questionnaire and the end-line interviews could not be linked for comparison, because the initial questionnaire was anonymous. Demographic information was collected from the 53 pharmacy workers who were interviewed at follow-up and not on the pre-training questionnaire. The responses in the unlinked questionnaires and interviews were analyzed for changes over time.
Quantitative data were entered and checked for consistency using EpiData version 6.0 (EpiData Association, Odense, Denmark) in Lusaka, Zambia, and imported into Stata version 11.0 (College Station, TX, USA) for further descriptive analysis. Bivariate analysis was used to examine pharmacist knowledge, attitudes and dispensing behaviours pre-training and at follow-up. Unadjusted chi-square statistics and their corresponding p-values were used to identify bivariate associations between categorical variables pre- and post-intervention; statistical significance was defined as p < 0.05.
The study protocol was reviewed and approved by the US-based Allendale Institutional Review Board and the University of Zambia Research Ethics Committee in Lusaka, Zambia. Questionnaires to assess a limited number of the pharmacy workers’ baseline characteristics and knowledge of medical abortion pre-training were used to explore training effectiveness. Questionnaires were anonymous and self-administered, and consent was obtained orally by the training group. No incentives were given for participation in the training; however, participants were provided with a meal and reimbursed for transport expenses. During follow-up, the interviews were carried out by trained data collectors, and standard, written, informed consent procedures were followed prior to conducting the interviews. Although some pharmacy workers could not be located, no one refused to participate. No incentives or remuneration were given to the pharmacy workers for completing a follow-up interview.
Findings
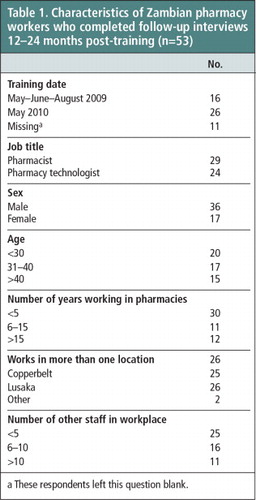
The pharmacy workers interviewed after the training were 68% male (Table 1), and 62% were over 30 years of age. Almost half (45%) were pharmacy technologists. Although almost two-thirds were trained on medical abortion in 2010 in the Copperbelt Province, they were almost evenly split in their workplaces between the Copperbelt Province (47%) and Lusaka (49%). The respondents in both studies were relatively inexperienced; 57% had worked in the pharmacy industry for five years or less. In both surveys almost half worked in more than one location and, in general, in large pharmacies with a large number of other staff.
Table 1 Characteristics of Zambian pharmacy workers who completed follow-up interviews 12–24 months post-training (n = 53).Footnotea
All but one pharmacy worker reported that women had sought their advice on unplanned pregnancies at one time (data not shown), confirming their importance in that role in their communities. Nearly all of the respondents reported feeling that it was their responsibility to provide information on abortion to women who requested it. Finally, the proportion of pharmacy workers who reported dispensing unsafe or ineffective abortifacients to women seeking abortion such as emergency contraceptive pills and contraceptives, or uterotonics such as pitocin or oxytocin, decreased from baseline to end-line from 30% to 25% but this difference was not significant (Table 2).
Table 2 Pharmacy workers’ attitudes and dispensing behaviours pre-training and at follow-up 12–24 months laterFootnotea.Footnoteb
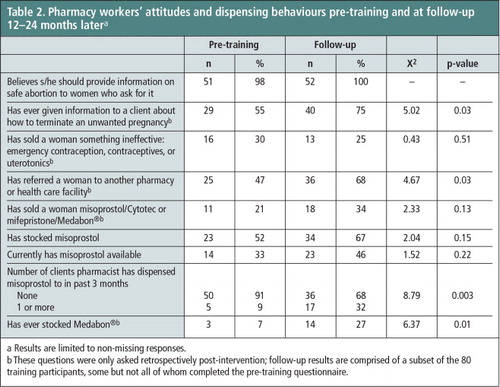
Between the baseline questionnaires and the interviews, the proportion of pharmacists reporting having given information to a woman about pregnancy termination also increased significantly, from 55 to 75% (p = 0.03; ). A higher percentage also reported referring women to a health care facility for services or information, rising from 47% to 68% (p = 0.03).
Figure 2 Pharmacy worker stocking behaviours and referrals pre-intervention and at follow-up according to harm reduction principles, 2009 to 2011a
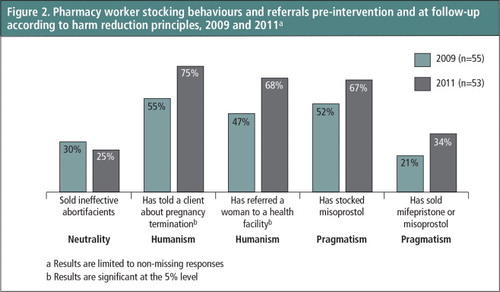
Some pharmacy workers adopted (or already had) pragmatic attitudes about abortion and responded by stocking and selling medical abortion drugs to accompany the clinical information given at their training. Stocking both misoprostol and Medabon® became more common among these pharmacies during the intervention period; stocking misoprostol increased from 33% to 46% (not significant) and Medabon® or mifepristone from 7% to 27% (p = 0.01; Table 2), respectively. Pharmacy workers also estimated selling misoprostol to more clients than they had at baseline with almost one-third estimating that they had sold misoprostol to one or more clients in the previous three months, an increase from 9% at baseline (p = 0.003). At end-line, 34% of pharmacy workers reported having sold a medical abortion product to a customer since training, an increase over the 21% of pharmacists who reported doing so at baseline, though this was non-significant.
Discussion and recommendations
As has been previously shown by researchers using a harm reduction framework to defend and argue for women’s access to information, resources and support to use misoprostol for self-induction, harm reduction shifts the conversation about abortion from its legal status to a focus on protecting women’s health.Citation8 In Zambia, although the concept of harm reduction was applied post-intervention, it translated the abstract concepts of neutrality, humanism and pragmatism into real terms. Our findings contribute further evidence about the pivotal role of pharmacy workers in promoting safer abortions in their communities.
Working with pharmacists provides an alternative to facility-based care for reaching women with information and, if desired and possible, medication for induced abortion. However, direct-to-client sales of medical abortion drugs is only one way of improving their knowledge and understanding of abortion. Pharmacy workers are convenient and inexpensive resources, and often the first source of information on health and illness in a community. Although most countries, including Zambia, prohibit pharmacists from selling abortion medications directly to women and men, their role as advisors, referral agents and sales agents is changing as these activities are more frequently being viewed as acceptable transgressions in the global debate on the right to safe, legal abortion.
While public access to mifepristone remains limited to Zambian public health facilities, in 2009 the misoprostol variants of medical abortion were more widely known by women, pharmacy workers and health care workers for their abortifacient qualities. However, all misoprostol products were registered only for uses other than abortion (including other gynaecological uses) so the information related to abortifacient properties among clinicians and pharmacists was limited and the information on the bioethics of dispensing these drugs almost absent.Citation10 As a result, a higher percentage of pharmacists reported selling women ineffective drugs, perhaps even unknowingly, and potentially delaying women from getting the care they needed. Eliminating these behaviours and barriers and helping pharmacy workers to provide women with more accurate evidence-based information, as happened in the follow-up interviews, is a core principle of the humanistic approach to making abortion safer.
An abortion induced with misoprostol alone is up to 90% effective through the first nine weeks of pregnancy and up to 87% effective from 9–13 weeks.Citation11 Medical abortion with a combined regimen of mifepristone followed by misoprostol is up to 98% effective when used as recommended.Citation12 During this study, having a legal abortion with medication in a health facility was a legal option in the intervention areas, and referrals to health facilities increased in the period between the questionnaire and the interviews. Providing women with referrals to health facilities was an integral part of the training provided, yet even where this option exists, as it does in some parts of Zambia, some women are too ashamed, afraid or lack the knowledge or ability to navigate the formal health system to obtain a legal abortion as has also been found in studies in Cambodia, Ethiopia and South Africa.Citation6,13–15 Ensuring that pharmacy workers reflect on their responsibility to respect women’s autonomy and choices and provide them with evidence-based information on their options, including self-induction, to mitigate as much harm as possible, was also an integral component of the training provided.
Pharmacy workers in this study also acted pragmatically and responded to both the need and demand from women seeking abortions. Both stocking and sales of medical abortion drugs increased during the study period in the pharmacy shops concerned, and the number of pharmacy workers reporting having sold misoprostol in the three-month period prior to the interview also increased significantly. In spite of increased awareness about facility-based abortion services and a willingness of pharmacy workers to provide referrals to these services, these data indicate that the demand for medical abortion drugs is still being met by some pharmacy workers. These findings are in line with other international research. Although abortion was decriminalized in Ethiopia in 2006, research conducted in 2008 estimated that only one-third of all abortions took place in health facilities.Citation16 In a study conducted in Cambodia, where abortion in the first trimester is unrestricted, 37% of women seeking post-abortion care in 2005 had already attempted termination prior to seeking care; 80% had sought advice or assistance from someone who sold medications.Citation13 Women in Zambia also deserve to benefit from scientific advances regarding safe induced abortion, whether or not they reach a health facility.Citation9
These study results demonstrate that Zambian pharmacy workers have a role to play in safe abortion services and that some are willing to play that role, even though they may choose to not sell medical abortion products directly.
Although direct-to-client sales of medical abortion products increased in the period of this study, in view of the generally low level of direct sales of medical abortion products, future trainings for pharmacy workers may need to offer simplified information on misoprostol alone – as well as additional materials for use in pharmacies – to provide accurate information to women who prefer to seek abortion information in the community. Simpler messages may allow for better retention and recall if this information is sought infrequently. As shown in other research conducted in Viet Nam and India, this intervention was most successful at improving attitudes and instigating referrals to health facilities, in line with the design of the study.Citation17,18
There were several limitations to this study. All data were retrospective and self-reported, rather than observed, and as such were prone to temporal and social desirability biases. A study design that matches pre- and post-intervention results and utilizes a control group of pharmacists who have not participated in training on medical abortion would provide better evidence on whether changes in behaviours are sustained over time and that they are related to the intervention and not solely the changing environment.
Efforts should be made to strengthen the human rights and harm reduction arguments in order to improve direct provision but this should not preclude a focus on other important objectives and reasons to improve information on abortion among pharmacy workers. Furthermore, factors besides training, such as availability and distribution of medications, may greatly affect the outcome of direct-to-client provision; efforts are needed in this area long after any training is completed. Interventions need to carefully assess the legal context, policy environment and availability of abortifacients but should honestly discuss the objectives of the training, including improving direct-to-client sales of proven effective medical abortion pills. Interventions for pharmacists also need to focus on eliminating barriers and address the ethics, benefits and risks of these behaviours. Whenever possible, training for pharmacy workers should also include the development of active referral networks for women who want and need information on facility-based abortion services. Honesty and willingness to address this topic could help improve availability of medical abortion and make abortion safer in Zambia and around the globe.
Acknowledgements
This research was funded by the Consortium for Research on Unsafe Abortion in Africa and its principal donor, the UK Department for International Development.
Notes
* The Termination of Pregnancy Act of 1972 permits abortion in Zambia under the following circumstances: the pregnancy causes a risk to the life of the pregnant woman; risk of injury to the physical or mental health of the pregnant woman; risk of injury to the physical or mental health of any existing children of the woman, greater than if the pregnancy were terminated; or if there is substantial risk of fetal malformation. Further amendments to the Penal Code allow abortion in cases of rape and incest.
* Diploma holders a level below registered pharmacists, who are not allowed to have their own dispensaries.
a These respondents left this question blank.
a Results are limited to non-missing responses.
b These questions were only asked retrospectively post-intervention; follow-up results are comprised of a subset of the 80 training participants, some but not all of whom completed the pre-training questionnaire.
References
- World Health Organization. Safe Abortion: Technical and Policy Guidance for Health Systems. 2nd ed., 2012; WHO: Geneva.
- Central Statistical Office Z Ministry of Health Z Tropical Diseases Reasearch Centre, et al. Zambia Demographic and Health Survey 2007. 2009; Macro International: Calverton, MD.
- D Webb. Attitudes to ‘Kaponya Mafumo’: the terminators of pregnancy in urban Zambia. Health Policy and Planning. 15(2): 2000; 186–193.
- RN Likwa, A Biddlecom, H Ball. Abortion statistics in Zambia: ‘A research brief for reproductive health programming, policy and research implications’. Issues Brief (Alan Guttmacher Institute). 3: 2009; 1–4.
- Ministry of Health. Standards and guidelines for reducing unsafe abortion morbidity and mortality in Zambia. 2009; MoH: Lusaka.
- Guttmacher Institute. Making Abortion Services Accessible in the Wake of Legal Reforms: A Framework and Six Case Studies. 2012; Guttmacher Institute: New York.
- RK Sneeringer, DL Billings, B Ganatra. Roles of pharmacists in expanding access to safe and effective medical abortion in developing countries: a review of the literature. Journal of Public Health Policy. 33(2): 2012; 218–229. 10.1057/jphp.2012.11.
- A Hyman, K Blanchard, F Coeytaux. Misoprostol in women’s hands: a harm reduction strategy for unsafe abortion. Contraception. 87(2): 2013; 128–130. 10.1016/j.contraception.2012.10.020.
- JN Erdman. Harm reduction, human rights, and access to information on safer abortion. International Journal of Gynecology and Obstetrics. 118(1): 2012; 83–86. 10.1016/j.ijgo.2012.04.002.
- RY Lee, R Moles, B Chaar. Mifepristone (RU486) in Australian pharmacies: the ethical and practical challenges. Contraception. 2014 Aug 15; 10.1016/j.contraception.2014.08.003. Epub ahead of print.
- H von Hertzen, G Piaggio, NTM Huong. Efficacy of two intervals and two routes of administration of misoprostol for termination of early pregnancy: a randomised controlled equivalence trial. Lancet. 369(9577): 2007; 1938–1946.
- H von Hertzen, NT Huong, G Piaggio. Misoprostol dose and route after mifepristone for early medical abortion: a randomised controlled noninferiority trial. BJOG. 117(10): 2010; 1186–1196. 10.1111/j.1471-0528.2010.02636.x.
- T Fetters, S Vonthanak, C Picardo. Abortion-related complications in Cambodia. BJOG. 115(8): 2008; 957–967. 10.1111/j.1471-0528.2008.01765.x.
- H Gebreselassie, T Fetters, S Singh. Caring for women with abortion complications in Ethiopia: national estimates and future implications. International Perspectives on Sexual and Reproductive Health. 36(1): 2010; 6–15. 10.1363/ipsrh.36.006.10.
- RK Jewkes, T Gumede, MS Westaway. Why are women still aborting outside designated facilities in metropolitan South Africa?. BJOG. 112(9): 2005; 1236–1242.
- S Singh, T Fetters, H Gebreselassie. The estimated incidence of induced abortion in Ethiopia, 2008. International Perspectives on Sexual and Reproductive Health. 36(1): 2010; 16–25.
- D Lara, K Abuabara, D Grossman. Availability of medical abortion pills and the role of chemists: a study from Bihar and Jharkhand, India. Reproductive Health Matters. 13(26): 2005; 65–74.
- TD Ngo, MH Park, TH Nguyen. Pharmacy workers’ knowledge and provision of abortifacients in Ho Chi Minh City, Vietnam. International Journal of Gynecology and Obstetrics. 117(2): 2012; 187–188. 10.1016/j.ijgo.2011.12.017.