Abstract
Introduction
The calcaneus is the largest and strongest tarsal bone. It is the most commonly fractured tarsal bone and accounts for about 2% of all fractures. The importance of the calcaneal angles in assessing the fractures of calcaneus and planning treatment has been highlighted.
Aim
The purpose of this study was to evaluate the normal calcaneal angles in the Egyptian populations who live in Alexandria and nearby governorates and compare their values to the published data.
Methods
Lateral plain radiographs of 220 normal feet and ankles of 103 males and 97 females with age ranged from 20 to 40 years, were studied retrospectively at El Hadra University Hospital, Alexandria, Arabrepublic of Egypt between June and December 2010. Three of the normal calcaneal angles (Böhler angle–Gissane's angle–calcaneal compression angle) were measured and the mean and standard deviation of each angle were calculated. The relationships between each angle and age, sex, side of the body, occupation, weight, height, and residence of examined persons was tested and compared to previous researches and international figures.
Results
The mean of Böhler angle in the Egyptian population was 30.14 ± 4.182 ranged from 22° to 40°. The mean of Gissane's angle was 122.92 ± 6.952 ranged from 108° to 138°, while the mean of calcaneal compression angle was 31.03 ± 3.82 ranged from 24° to 44°. The measured calcaneal angles are not significantly related to age, sex, and side of the body, residence and occupation of the examined persons except there is significant negative correlation between the Böhler angle and the age which not reported in the previous researches and studies.
Conclusion
The study showed that difference in the mean of the calcaneal angles from other previous studies that reinforce the importance of establishing the normal range of the calcaneal angles in a given population.
1 Introduction
The skeleton of the foot has three segments (the tarsal bones, the metatarsal bones, and the phalanges). There are seven tarsal, five metatarsals, and 14 phalanges.Citation1 The tarsal bones: the talus, calcaneus, navicular, three cuneiforms (medial, intermediate, and lateral), and cuboid.Citation1
The calcaneus is irregularly cuboid in shape and its long axis is directed forwards, upwards, and somewhat laterally.Citation1 It has six articular surfaces: Superior calcaneanl surface: This is formed of three parts; posterior, middle, and anterior. The posterior third is non-articular, rough, and perforated by vascular foramina. The middle third is oval, convex anteroposteriorly and carries the posterior talar facet.Citation1 The anterior third consists of the sulcus-calcanei which completes the sinus tarsi with the talus, in addition to the anterior and middle articular facets.
Anterior surface: The smallest, it is an obliquely set concavo-convex articular facet for the cuboid bone.Citation1
Posterior surface: It is divided into three: a smooth proximal area separated from the tendo-Achilles by a bursa and adipose tissue; a middle area, the largest, limited above by a groove, below by a rough ridge, for the calcaneal tendon; and a distal area inclined downwards and forwards, vertically striated, which is the subcutaneous weight-bearing surface.Citation3
Plantar surface: This is rough, especially proximally as the calcaneanl tuberosity, the lateral and medial processes of which extend distally, separated by a notch. The medial is longer and broader.Citation3 Further distally, an anterior tubercle marks the distal limit of the attachment of the long plantar ligament.Citation3
Lateral surface: Almost flat, it is proximally deeper and palpable on the lateral aspect of the heel distal to the lateral malleolus.Citation3
Medial surface: Vertically concave, its concavity is accentuated by the sustentaculum tali projecting medially from the distal part of its upper border. Superiorly the process bears the middle talar facets and inferiorly a groove continuous with that on the talar posterior surface for the tendon of flexor hallucis longus.Citation3
1.1 Radiographic anatomy
The trabecular pattern within the calcaneus reflects the static and dynamic stresses to which it is repeatedly subjected.Citation2 Traction trabeculae radiate from the inferior cortex of the calcaneus while compression trabeculae converge to support the posterior and the anterior facets.Citation2
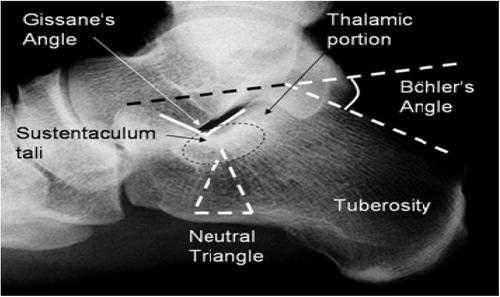
The thalamic portion of the calcaneus is the condensation of bone trabeculae beneath the anterior and posterior facets.Citation2 Within the calcaneal trabeculations, a “neutral triangle” has been defined. It is an area with sparsetrabeculation thought to be used by blood vessels to reach the medullary cavity. This neutral triangle is prone to impaction in the typical compression fracture.Citation2 The cortical bone is especially thin at the lateral wall of the calcaneus, which leads to its bulging in calcaneal fracture ().Citation2
1.2 Histological composition
The calcaneus is composed mostly of cancellous bone and has a very thin cortical shell.Citation4 The exceptions are the cortical thickening that supports the posterior facet, the dense cortical bone in the sustentaculum tali, and the relatively thick cortex in the angle of Gissane's.Citation4 These areas of thickened bone are used as guide to reduction.Citation4
1.3 Joints
1.3.1 The subtalar joint
It is formed between the large concave facet of the body of the talus and the convex posterior articular surface of the superior aspect of the calcaneus.Citation6A loose, thin-walled capsule unites the bones attached to the margins of the articular surfaces.Citation6
Stronger ligaments connect the two bones as the medial, lateral, posterior and the interosseus talo-calcaneal ligaments.Citation6 The subtalar joint (STJ) is defined functionally as a joint formed by all three articulating facets (of the calcaneus and the matching facets of the talus.Citation6
1.3.2 The mid (transverse) tarsal joint
It is also called the Chopart's joint. It is composed of the talonavicular articulation medially and the calcaneocuboid laterally. These separate joints combine functionally to contribute primarily to the inversion–eversion action of the foot.Citation6
There are important angles which are seen on the radiograph (AP and lateral) of the calcaneus and the measurements of these angles are good geometrical indices for assessment of the subtalar joint and calcaneal fragments alignment following calcaneal fractures and their treatment.Citation7
1.4 Lateral view
1.4.1 Tuber joint angle (TJA)–Böhler's angle ()
BA was introduced by Dr. Lorenz Böhler in 1931 as the tuber angle and the range was in his article 30–35. It is a complementary angle subtended on the lateral X-ray by the intersection of two lines.Citation7 The first line is drawn from the highest point of the anterior process to the highest point of the posterior facet. The second line runs tangential to the superior edge of the tuberosity.Citation7 It is known also salient angle, critical angle. It ranges from 25° to 40°, with an average of 30°.Citation7 Anatomic variations of the three references on dry bone which define this angle were very small. Böhler's angle is therefore a good morphologic reference for evolutive study of each patient.Citation7 If the tuberosity is displaced upwards or the articular surface is displaced downwards, the angle may be reduced to 20° or 10° or it may be obliterated altogether, or it may even be represented by a negative angle.Citation7 Therefore, a decrease in this angle may indicate that the weight bearing surface of the oscalcis (the posterior facet) has collapsed, shifting the weight of the body anteriorly.Citation7 In 1931, Böhler proposed that measuring the radiological angle of the tuberosity could be useful in posterior facet fractures of the calcaneus to evaluate initial damage as well as reduction quality. In opposition to the 1998, certain authors considered that the Böhler angle has no prognostic value. Progress in pathological anatomy has helped to better understand posterior facet fractures, justifying the use of a “double measurement”.Citation7 The fundamental fracture line separates the posterior facet into a lowered medial fragment and a pivoted lateral fragment. The double contour of the posterior facet visualized radio graphically allows measurement of a medial Böhler angle and a lateral Böhler angle. It is demonstrated that is the smaller the medial Böhler angle, the greater the subtalar degeneration. Surgical restoration of a satisfactory Böhler angle is a necessary prerequisite for a good outcome.Citation7 “Double measurement” of the Böhler angle on the lateral view contributes to the prognostic value of this historical angle. McLaughlin pointed out that reduction or reversal of this angle indicates only the degree of proximal displacement of the tuberosity and thus limiting its usefulness.Citation7
1.4.2 Crucial angle of Gissane's (GA)
On lateral radiograph, there are two thick and strong cortical struts that exist within the calcaneus and extend from the front of the bone to the posterior facet (the densities of the subchondral bone of the posterior facet and that of the anterior and middle facets).Citation10 These struts are angled, and the angle supports the lateral process of the talus. This angle was termed “the crucial angle” by Gissane's. It ranges from 120° to 140° with an average of 130° ().Citation10 The angle gives some information about the relationship of the posterior, anterior, and middle facets. Axial compression forces, with the talus acting as a bursting wedge, will disrupt the subtalar joint and distort the crucial angle.Citation10
1.4.3 Calcaneal pitch angle (CPA)
It is subtended by two lines originating at the lowest point on the calcaneus, one joining it to the head of fifth metatarsal bone and the other to the lowest point of the calcaneocuboid joint. It ranges from 15° to 44°, with an average of 28° (). It is the actual measurement of the longitudinal arch of the foot. It is reduced with displaced intra-articular fractures.Citation10
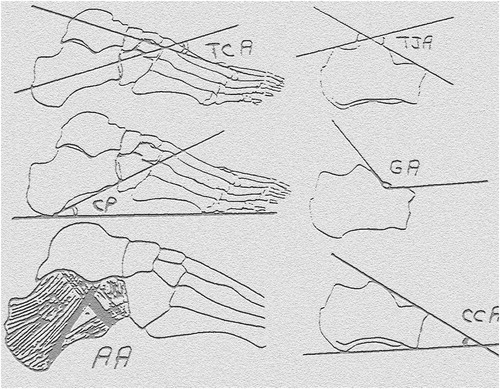
1.4.4 Calcaneal compression angle (CCA)
It is derived from a line in the plane of the inferior surface of the calcaneus, while the other line is identical to the first line of the Böhler's angle.Citation7 It ranges from 18° to 42°, with an average of 36°. It can be used as an alternative method for assessing intra-articular calcanean fractures, in particular, when there is extensive depression and rotation of the superior aspect of the oscalcis (). It represents the height of the calcaneus and its reduction occurs in collapse and comminution of the bone.Citation10
1.4.5 Lateral talo-calcaneal angle (TCA)
It is the angle between the long axis of the talus and that of the oscalcis. It measures the inclination of the talus over the oscalcis, so it can be used as a measurement of the hindfoot alignment. It increases with valgus angulation of the hindfoot and diminishes with talipes equino varus approaching parallelism (). An increase of TCA frequently raises the possibility of flat foot, metatarsus varus and it is reversed in congenital vertical talus.Citation10
1.4.6 Apical angle of pseudo cystic triangle (AA)
The angle between anterior and posterior compression trabeculae groups which increases with osteoporosis and disrupted in comminuted fractures ().Citation7
1.4.7 Variation of the calcaneal angles measurement in adults
| (1) | Traumatic variation of the normal calcaneal angles (calcaneal fracture). According to the distortion of the normal calcaneal angles, two types of calcaneal fracture: the first one (intra-articular) distorts the calcaneal angles while the second one (extra-articular) doesn't distort the calcaneal angles.Citation3 | ||||
| (2) | Non-traumatic variation (pes-cavus, flat foot and hind foot deformities).Citation10 | ||||
2 Methods
The work included 200 adult cases (180 cases unilaterally examined clinically and radiologically and 20 cases bilaterally examined clinically and radiologically) taken randomly from persons presented to El Hadara University Hospital with problems affecting sites rather than the lower limbs. The youngest person in the study was 20 years old and the oldest one was 60 years old with a mean age 40 ± 20. There were 103 males and 97 females with the ratio about 51.5:48.5. There was 10 males bilaterally examined radiologically and clinically and another 10 females were bilaterally examined. So there were about 113 male's feet and 107 female's feet. The right foot was examined in about 112 normal person's feet and the left side was examined in about 108 normal case's feet. There were 70 manual workers, 25 farmers, 65 office workers, 24 unemployed, and 36 house wives. There were about 80 persons who live in urban areas and about 120 persons who live in the ruler areas with the ratio 2:3. There were about five persons classified as underweight, about 59 persons as normal weight class, 89 persons as Overweight, and 67 person's feet in obese in different classes.
A full workup including history taking, clinical examination and radiological evaluation were performed for every person examined. All cases were assessed clinically and functionally and the cases with abnormal finding (gait abnormality, congenital, or acquired deformity, weakness of the muscle power) were excluded from this study. Angles of oscalcis (Böhler angle, Gissane's angle, and calcaneal compression angle) will be studied and analyzed. On these radiographs the reference lines were drawn for angle measurement with a chin graph pencil on translucent sheet placed over the radiographs. The angles were measured by two investigators separately also each one of the investigators measured the angles two times with different intervals by using hand-held geniometer. Angles of oscalcis were measured and the mean and the standard deviation of each angle were calculated. The relationship between each angle and age, gender, weight, occupation, residence, and side of body was tested and compared to international figures. The relationships between each measured angles were assessed.
2.1 Statistical analysis
After data collection, the results will be tabulated as frequency distribution for different qualitative values. The arithmetic mean and standard deviation and median were calculated for quantitative variables. All that results were compared with results of previous studies. SPSS (statistical package of social sciences) 13.0 software was used in statistical analysis also dependent t-test was used to compare paired samples (comparison of the angles according to the side), independent t-test was used to compare the angles according to the sex), distribution of the angles within different age groups was compared with one way analysis of variance (ANOVA) test. The level of significance was set at p < 0.05, and compared the results of the present study with those of Didia and Dimkpa's study on the Nigerian population, those of Askel Seyahi's study on the Turkish population and those of Khoshhal ‘s study on Saudi population.
3 Results
The mean of the Böhler angle in the study was 30.141 ± 4.182 and ranged from 22° to 40°. The mean of the Gissane's angle was 122.9 ± 6.952 and ranged from 108° to 138°. The mean of the calcaneal compression angle was 31.03 ± 3.862 and ranged from 24° to 44° (). In that study the Böhler angle has the highest mean 31.27 in the age group between 20 and 30 years old, however, the lowest mean 29.30 was found in the age group between 30 and 40 years old. The Gissane's angle has the highest mean 125.08 in the age group between 41 and 50 years old, however, the lowest mean 120.63 was found in the age group between 51 and 60 years old. The calcaneal compression angle has the highest mean 31.75 in the age group between 41 and 50 years old, however, the lowest mean 30.61was found in the age group between 31 and 40 years old (). There was a significant negative correlation between the age and the measurement of Böhler angle which means that with aging the measurement of Böhler angle is reduced. However, insignificant correlation was found with the calcaneal compression angle and the Gissane's angle between different age groups (). In that study, the mean of the Böhler angles in males was 29.84 ± 4.08 ranged from 22° to 38° and the mean in females 30.44 ± 4.30 ranged from 24° to 40°. The mean of the Gissane's angle in the males was 122.2 ± 7.00 ranged from 108° to 136° and in the females 123.64 ± 6.90 ranged from 108° to 138°. The mean of the calcaneal compression angle in the males was 30.82 ± 4.28 with range from 24° to 44° and the mean was in females 31.24 ± 3.35 with range from 24° to 36°. There were no statistically significant differences between the measured angles and the sex. In that study, the mean of the Böhler angle of the right side of the examined feet was 30.20 ± 4.20 ranged from 22° to 40°. However, the mean of the angle in the left side of the examined feet was 30.08 ± 4.21 ranged from 24° to 38°. The mean of the Gissane's angle of the right side of the examined persons was 124.06 ± 7.13 ranged from 108° to 138°, however, the mean of the angle in the left side of the examined persons was 121.73 ± 6.62 ranged from 108° to 136°. The mean of the calcaneal compression angle of the right side of the examined persons was 30.51 ± 3.73 ranged from 24° to 40°, however, the mean of the calcaneal compression angle of the left side of the examined persons was 31.58 ± 3.89 ranged from 24° to 44° (). There was no statistically significant difference between the measured angles (BA–GA–CCA) and the side. In that study, the highest mean of Böhler angle was 31.67 ± 4.55 in the office worker however, the lowest mean 28.40 ± 3.75 was found in the farmer. The highest mean of Gissane's angle was 123.80 ± 9.67 in the un-employed and the lowest mean of Gissane's angle 121.80 ± 6.36 was found in the farmer. The highest mean of calcaneal compression angle was 32 ± 6.11 in the unemployed and the lowest mean was 30 ± 4.71 in the farmer (). There was no statistically significant difference between the measured angles and the occupation. In that study, the mean of the Böhler angle of the urban residents was 29.50 ± 4.31 with the range from 24° to 40° while the mean of the angle in the rural residents was 30.59 ± 4.07 with the range from 22° to 38°. The mean Gissane's angle of the urban residents was of a mean 124.63 ± 6.79 with the range from 108° to 138° while the mean of the angle in the rural residents was of a mean 121.78 ± 6.88 with the range from 108° to 136°. The mean calcaneal compression angle of the urban residents was of a mean 30.50 ± 4.10 with the range from 24° to 40° while the mean of the angle in the rural residents was 31.39 ± 3.62 with the range from 24° to 44° (). There was no statistically significant difference between the measured angles and the residence. In that study, the highest mean of Böhler angle was 31.02 ± 3.80 in normal persons regarding the body mass index (18.5–24) with the range of measurement from 22° to 40° while the lowest mean of was 27.60 ± 3.29 in underweight persons regarding the body mass index (less than 18.5). The highest mean of Gissane's angle was 123.68 ± 6.44 in obese class I regarding the body mass index (30–34.9) with the range of measurement from 108° to 138° while the lowest mean of Gissane's angle was 118.40 ± 7.13 in underweight persons regarding the body mass index with the range of measurement from 108° to 126°. The highest mean of calcaneal compression angle was 31.74 ± 3.70 in normal persons regarding the body mass index with the range of measurements from 26° to 44° while the lowest mean of calcaneal compression angle was 28.40 ± 3.58 in underweight persons regarding the body mass index less than with the range of measurement from 24° to 32° (). There was negative correlation between the body mass index and both (Böhler angle and the calcaneal compression angle) which mean that with increase the body mass index will decrease both (Böhler angle and calcaneal compression angle) measurement. However, this correlation was not statistically significant. Also there was no significant correlation between the Gissane's angle and the body mass index. In that study, there was significant positive correlation between the Böhler angle and the calcaneal compression angle; but there was no significant correlation between the Gissane's angle and the both Böhler angle and the calcaneal compression angle ().
Table 1 Normal ranges and means of the calcaneal angles reported in previous studies compared to the present study.
Table 2 Pearson correlation between age and different measured angle.
Table 3 Relation between different measured angle and the age.
Table 4 Relation between different measured angle and residence.
Table 5 Relation between different measured angle and body mass index.
Table 6 Relation between different measured angle and side.
Table 7 Relation between different measured angle and occupation.
Table 8 Correlation between BMI and different measured angles.
4 Discussion
Our study revealed a wide range for calcaneal angles in the Egyptian population, as previously reported for other populations in previous studies ().Citation4,Citation5,Citation8,Citation9 BA was between 22° and 40° and GA was between 108° and 138° and CCA 24° and 44°. As both calcaneal angles generally decrease during calcaneal fractures, the lower limit of the angles should be of greater interest. However, after some fractures the angles may remain in normal limits especially in the individuals with a wide Böhler or Gissane and calcaneal compression angle. In such cases, the degree of displacement may be misjudged and an inappropriate correction may be planned. Thereby their wide ranges probably reduce the utility of calcaneal angles in clinical practice. Didia and Igbigbi, who assessed the calcaneal angles in black Africans showed an ethnic and geographic variability for these angles.Citation5 Igbigbi found that the mean BA in women was greater than those of men and he noted that the previous studies failed to show this relation because of their limited sample sizes.Citation4 Our series involved a larger group of subjects and did not reveal a statistically significant BA difference between the sexes. This result was in agreement With all the previous studies except Igbigbi's study.Citation4 Comparison according to the side should be done on the same subject. That is one must compare the right and left side angles of the subjects whose both feet X-rays are available, rather than comparing the mean of all of the right sided and left sided X-rays in the study group. Only the study of Khoshhal evaluated the relation of the calcaneal angles and the side in this manner, and did not reveal any relation according to the side.Citation8 We also compared the sides on the same subjects and did not find any relation. This result suggests that in unilateral calcaneal fractures the calcaneal angles of the intact side may be taken as an individual reference value. The relation of the calcaneal angles with age should ideally be assessed on the X-rays of the same individual, taken at different ages. Our cross sectional study enabled only to make an analyze between the different age groups and no significant correlation was found between age and calcaneal angles except with BA which show negative correlation between age and BA which is not mentioned in the previous studies and researches.Citation9 There was also no significant difference between the mean calcaneal angles of the different age groups. These results suggest that an old X-ray of a patient with calcaneus fracture cannot be considered to assess the normal calcaneal angles for this individual which not in agreement with other previous studies. The mean BA of our series was significantly different than those of the previous series, confirming the previously reported ethnic and geographic variability for this angle. The distribution of the BA was significantly different from Nigerian and Saudi Arabian population.Citation5,Citation8 The mean GA was significantly different from the previous reports.Citation9
5 Conclusion
Calcaneal angles have a wide range of normal limits and distribution in different populations. Therefore, their normal limits and distribution of should be defending for a given population. The range of 22°–40° for the BA and 108°–138° for the GA can be taken as the normal ranges for the Egyptian population. The calcaneal compression angle was not studied before. The range of the calcaneal compression angle was wide range from 24° to 44° also there was significant correlation between the Böhler angle and the calcaneal compression angle so can be used as reserve for BA in extensive communication of posterior facet of the oscalcis. There is no significantly correlation between the calcaneal angles and the sex, side of the body, occupation, residence, and body mass index; however, Böhler angle is significant correlated with the age which means that it decreases with aging. However, there is no correlation between both calcaneal compression angle and Gissane's angle with the age.
Notes
Available online 1 February 2012
Peer review under responsibility of Alexandria University Faculty of Medicine.
Related Research Data
References
- A.MiricB.M.PattersonPathoanatomy of intra-articular fractures of the calcaneusJ Bone Joint Surg (Am)802-A1998207212
- A.DaftaryA.H.HaimsM.R.BaumgaertnerFractures of the calcaneus: a review with emphasis on CTRadiographics255200512151226
- R.SandersP.FortinT.Di PasqualeA.WallingOperative treatment in 120 displaced intra-articular calcaneal fractures. Results using a prognostic computed tomography scan classificationClin Orthop Relat Res29019938795
- P.S.IgbigbiA.V.MutesasiraCalcaneal angle in UgandaClin Anatomy162003328330
- B.C.DidiaJ.N.DimkpaThe calcaneal angle in Nigerians. Relation to sex, age, and side of the bodyJ Am Poditar Med Assoc891999472474
- D.G.WrightM.E.DesalB.S.HendersonAction of the subtalar and ankle joint complex during the stance phase of walkingJ Bone Joint Surg (Am)46-A1964361367
- L.BöhlerDiagnosis, pathology, and treatment of fractures of the oscalcisJ Bone Joint Surg (Am)1319317589
- K.I.KhoshhalA.F.IbrahimN.A.Al-NakshabandiM.M.ZamzamA.A.Al-BoukaiM.M.ZamzamiBöhler's and Gissane's angles of the calcaneus in the Saudi populationSaudi Med J25200419671970
- A.SeyhaiS.UludagL.O.KoyuncuA.C.AtalarM.DemerhanThe calcaneal angles in the Turkish populationActa Orthop Traumatol Turc432009406411
- D.J.HakT.L.GautschA review of radiographic lines and angles used in orthopedicsAm.J orthop1995590611