Abstract
Aim
To examine the validity of US in assessing hand osteoarthritis (OA) and to study the relationship between ultrasonographic findings and OA symptoms.
Methods
This study was carried out on thirty patients with primary hand OA, and fifteen healthy subjects serving as a control group. Patients were classified according to ultrasonographic findings of joint involvement into two subgroups: 15 patients with interphalangeal (IP) OA and 15 patients with IP and first carpometacarpal (CMC) joint OA. All hand joints were examined for tenderness, soft tissue swelling, hard tissue enlargement (nodes), and deformity. Functional assessment by AUSCAN questionnaire, grip and pinch strength measurement and pain assessment by Visual Analogue Scale (VAS) were carried out. Plain X-rays of both hands were taken and classified according to the Kellgren–Lawrence (K–L) grading scale. High resolution US of the hand joints was performed which focused on examining cartilage thinning, joint space narrowing (JSN), and osteophytes (OST).
Results
There was a positive correlation between the K–L grading and US findings regarding JSN and OST. There was a positive correlation of AUSCAN score with cartilage thinning, OST and JSN. There was a negative correlation of grip strength with cartilage thinning and OST. There was a negative correlation between pinch strength and US findings (cartilage thinning, OST and JSN). There was a positive correlation between pain and US findings. Heberden's nodes were associated with underlying distal IP cartilage thinning, OST and JSN. On comparing the two subgroups of patients; patients with both IP and first CMC joint involvement experienced significantly higher levels of pain and disability and had weaker pinch strength.
Conclusions
Ultrasonographic findings correlated with clinical findings as nodes, functional parameters as grip and pinch strength, and pain. The increased detection of OA structural pathology by US may make this a useful tool for hand OA assessment.
1 Introduction
Osteoarthritis (OA) is the most common form of arthritis among the elderly. Joints most affected by this disease are knees, hips and hands.Citation1,Citation2 Hand OA is a highly prevalent condition. It occurs commonly, though not exclusively, in the context of generalized OA, and can result in considerable disability. Although a number of criteria have been used to define hand OA clinically, radiographically or epidemiologically, its diagnosis and classification present certain difficulties due to a number of issues.Citation3 Challenges in diagnosing and classifying hand OA include different diagnostic possibilities (as rheumatoid arthritis, diabetic hand syndrome, gout and psoriatic arthritis), the large number of joints that may be affected, the nature of Heberden's nodes (HN) and Bouchard's nodes and their relationship to underlying OA of the interphalangeal (IP) joints.Citation3
Other challenges include poor correlation between symptoms and structural changes of OA in the same joint, differences between OA of the IP joint and base of the thumb regarding risk factors and prognosis, and lack of consensus regarding the nature and specificity of erosive OA as a discrete subset of hand OA.Citation3 EULAR Standing Committee for International Clinical Studies Including Therapeutics (ESCISIT) task force set out to develop recommendations for the diagnosis of hand OA, using an evidence based format involving both a systematic review of available research evidence and expert consensus opinion.Citation4
Previous epidemiological studies have largely targeted radiographic OA, and most of them have concentrated on knee and hip joints. While symptomatic hand OA should be a focus of studies because it causes disability and has formidable societal and public health impact, few studies have been conducted especially among the elderly.Citation3
Osteoarthritis has traditionally been imaged with conventional radiographs (CR). However, in recent years, novel imaging techniques such as musculoskeletal ultrasonography (US) has been utilized to obtain a better understanding of this disease. Although the application of US to inflammatory diseases has been common and widespread, it has been applied to OA less frequently.Citation5–Citation7
2 Methods
This study was carried out on thirty patients with hand OA, and fifteen healthy age and sex-matched subjects serving as a control group. Patients were classified according to ultrasonographic findings of joint involvement into two subgroups: 15 patients with IP joint OA and 15 patients with IP and first carpometacarpal (CMC) joint OA. Personal data was obtained from patients and controls, which included age, sex, occupation and menstrual history in females, as well as detailed history about their hand condition including morning stiffness, joints involved, relieving and aggravating factors and medications received.
All studied subjects underwent general examination as well as local examination of the hand joints; distal interphalangeal (DIP), proximal interphalangeal (PIP), metacarpophalangeal (MCP), firstt CMC and the wrist joints of both hands. All areas were examined for tenderness, soft tissue swelling, nodes and deformities. Each finding was graded on a scale of 0–3, where 0 = normal, 1 = mild, 2 = moderate and 3 = severe. Pain severity was assessed by the Visual analogue scale (VAS).Citation8 They underwent functional assessment using the Australian Canadian Osteoarthritis hand index (AUSCAN) questionnaire,Citation9 which rated their pain, stiffness and limitation of functional activities on a scale of 0 (no problems at all) to 4 (extremely difficult). Grip strength was measured for each hand with a standard dynamometer (using the mean of three attempts). Pinch strength was measured with a pinchmeter for each hand; the mean value of the three trials was recorded. Laboratory investigations, which included erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), rheumatoid factor titer, and uric acid were measured as recommended by EULAR to exclude secondary causes of hand OA.Citation4 Postero-anterior hand radiographs were taken and OA severity was classified according to the Kellgren–Lawrence (K–L) grading scale.Citation10 High resolution US, using Siemens Prima apparatus, utilizing high resolution multi-frequency probe (7.5–10 MHz) was used to assess each joint for: cartilage thinning, osteophytes (OST) and joint space narrowing (JSN), and was subjectively graded from 0 to 3 (none, mild, moderate and severe) by the same ultrasonographer.
2.1 Statistics
Data was analyzed using the Statistical Package for Social Sciences (SPSS ver.17 Chicago, IL, USA). The data was score type and non-parametric tests were applied. Mann Whitney (U) test was used to compare quantitative variables between the two groups. Chi square test was also performed. Spearman rank correlation test was used to test correlations. In all statistical tests used, the level of significance (P) was set at 0.05, below which the results were considered to be statistically significant.
3 Results
Thirty patients diagnosed with primary hand OA; 22 females (73.3%) and 8 males (26.6%) were enrolled in this study. Their median age was 60 years (range: 50–84). The control group consisted of 15 healthy individuals; 10 females (66.6%) and 5 males (33.3%). Their median age was 55 years (range: 42–65). There was no statistically significant difference between the patients and controls regarding age (P = 0.062). All female patients were post-menopausal and all the patients were right-handed. Positive family history of hand OA was present in 18 patients (60%). Regarding their occupations, there were 21 housewives (70%), 1 physician (3.33%), 3 office workers (10%), 3 nurses (10%) and 2 tailors (6.66%).
Heberden's nodes were detected in the right hand in 24 patients (80%), and in the left hand in 4 patients (13.3%). Bouchard's nodes were found in the right hand of 2 patients (6.7%). Tenderness was detected in the right DIP in 3 patients (10.0%), in the left DIP in 1 patient (3.3%), in the right PIP in 1 patient (3.3%), in the right CMC in 4 patients (13.3%) and in the left CMC in 1 patient (3.3%). Deformities were detected in the right DIP in 13 patients (43.3%), in the left DIP in 2 patients (6.7%), in the right PIP in 3 patients (10%) and in the right CMC in 1 patient (3.3%). No soft tissue swelling was detected in any joint.
shows the distribution of the ultrasonographic findings in the different hand joints in the patients. On US, 4 patients had grade 1 cartilage thinning, while 20 had grade 2, and 3 patients had grade 3. Regarding OST, 2 patients had grade 1, 16 had grade 2, and 10 had grade 3 (). As for JSN, 10 patients had grade 1, 6 had grade 2, and 3 had grade 3. The controls had no evidence of OA on plain X-ray, however, on US, 4 of them had evidence of grade 1 cartilage thinning. The most severely affected joint in each hand, detected by US, was used for scoring. There was a statistically significant difference between US findings in the right and left hands of patients, being severer in the right hand (P < 0.01).
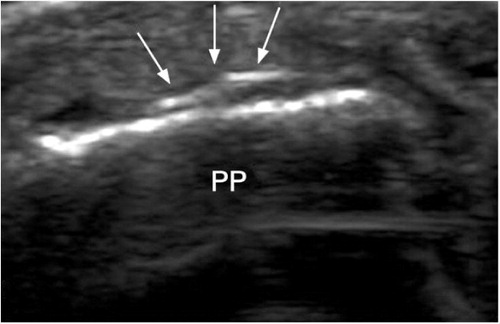
Table 1 Distribution of the ultrasonographic findings in the different hand joints in the patients (expressed as percentage of patients).
On correlating the various parameters, there was a positive correlation between K–L grading and US findings of JSN (P = 0.001) and OST (P = 0.002). There was a negative correlation between grip strength and cartilage thinning (r = −0.579, P = 0.001) and between grip strength and OST (r = −0.490, P = 0.001). No significant correlation between grip strength and JSN was detected (r = −0.276, P = 0.069). There was a negative correlation between pinch strength and all US findings (cartilage thinning, JSN and OST; P = 0.001 in each). There was a positive correlation between all US findings and VAS (P < 0.001 in each). There was a positive correlation of the AUSCAN total score with the US findings: Cartilage thinning (P = 0.008), JSN (P = 0.001) and OST (P = 0.01). There was a positive correlation between functional impairment measured by AUSCAN function subscale and VAS (r = 0.754, P = 0.001). However, there was no correlation between AUSCAN function and grip strength (r = −0.112, P = 0.632). There was an association between HN and US findings (). Patients with combined IP and CMC joint involvement had significantly higher VAS and AUSCAN scores and weaker pinch strength compared to those with only IP joint involvement ().
Table 2 Relation between Heberden's nodes and underlying US findings in the studied subjects.
Table 3 Comparison between group A (IP joint affection) and group B (IP and first CMC joint affection).
4 Discussion
In view of the previously published literature, OA is the leading cause of musculoskeletal morbidity in the elderly.Citation11 Knee, hip, IP and the first CMC joints are mostly involved.Citation12 Disability directly related to hand OA has largely been ignored, although several studies have shown a significant impact of OA on hand strength and function.Citation13,Citation14
The order of involvement of the hand joints in this study was comparable with other findings; DIP joints and first CMC joints were involved more often, followed by the PIP and MCP joints. Kellgren et al.Citation15 and Egger et al.Citation16 reported similarly that MCP joints had the lowest frequency, in contrast to Van Saase et al.,Citation14 who reported a higher prevalence of OA in MCP than in PIP joints. Chaisson et al.Citation17 also reported this inconsistency.
In the current work, there was a statistically significant difference between the patients and controls regarding AUSCAN score, VAS and grip strength. Similar observations were reported by Bagis et al.,Citation18 who studied the effect of hand OA on grip and pinch strength and hand function in postmenopausal women. They noted that patients with hand OA had lower grip and pinch strength than normal controls, and there were significant differences according to the grades of OA. Kjeken et al.Citation19 reported that hand OA had important functional consequences in terms of pain, reduced hand mobility and grip force, activity limitations, and participation restrictions.
In the current study, right hand joints were more severely affected compared to the left hand as regards cartilage thinning (P = 0.005), OST (P = 0.005) and JSN (P = 0.007). This is in agreement with Acheson et al., who suggested that almost every joint in the right hand of right-handed people of either sex had more frequent and severer disease than their left hand.Citation20
Osteoarthritis has been traditionally imaged using CR; this has been regarded as the reference technique in OA for a long time.Citation21 Recent years have witnessed an increasing interest of research in this field confirming a more widespread use of US for imaging different aspects of rheumatic pathology, including OA.Citation22,Citation23 Regarding the correlation between the K–L scale and US findings, there was a positive correlation between K–L scale and both JSN (P = 0.001) and OST (P = 0.002), whereas there was no correlation with cartilage thinning. A similar study was conducted by Keen et al.Citation24 who compared the detection of OST and JSN by US and CR in hand OA. They reported that CR had very low sensitivity in demonstrating minimal cartilage involvement in early disease.Citation24 Möller et al.Citation25 evaluated the reliability and validity of a novel US imaging method to measure MCP and PIP finger joint cartilage. They found the US method of direct visualization and quantification of cartilage in MCP and PIP joints objective, reliable, valid, and useful for diagnostic purposes in patients with arthritis.Citation25
Regarding the correlation between clinical signs and US findings, HNs were found to be associated with OSTs, cartilage thinning and JSN. All patients with HN had cartilage thinning, 95.8% of those patients had OST and 70.8% had JSN. These findings are in accordance with a study conducted by Thaper et al.Citation26; they showed that digital nodes are associated with underlying radiographic changes of IP joint OA, but this association was stronger for OST. They proposed that because nodes evolve slowly to reach their maximum size, the radiographic JSN manifests later in the course of node development and that established nodes affecting both medial and lateral aspects of the joint are a good clinical marker for this change.Citation26
In this study, no associations were found between Bouchard's nodes and any of the US findings. The stronger relationship between HN and radiographic changes seen at DIP joints might be explained anatomically. The presence of lateral bands over PIP joints may influence OST growth making it less distinct than at DIP joints.Citation26 However, Cicuttini et al.Citation27 noted that DIP OST and HN were weakly correlated. This different conclusion may be accounted for in part by the population studied. They studied middle-aged female twins with a mean age of 56 years, whereas we studied both women and men with a median age of 60 years. Such a demographic difference might result in our population having more patients with fully established nodes. This can be explained by the fact that nodes are formed by endochondral ossification, thereby a temporal difference might be expected, in that new (radiolucent) fibrocartilage might form a palpable swelling some time before calcification and ossification make it apparent on radiographs.Citation27 It may also be due to lack of a clear definition of HN in the literature.
As regards the correlation between functional parameters and underlying US findings, a negative correlation between grip strength and both cartilage thinning (r = −0.579, P = 0.001) and OST findings (r = −0.49, P = 0.001) was detected on US. Baron et al.Citation28 did not find correlations between objective hand function and OA, or between hand strength and OA. They suggested that the deterioration of the objective hand function and strength was related to the neuromuscular condition rather than articular degeneration.
In the current study, AUSCAN total score was positively correlated with US findings of cartilage thinning (P = 0.008), JSN (P = 0.001) and OST (P = 0.01). This was in disagreement with Patrick et al.Citation29 who suggested that hand function was not consistent with the extent of radiologic change. However, their study as well as other previous studies used CR as an assessment tool; none of them used US for evaluation. In this study, AUSCAN function score was positively correlated with pain assessed by VAS (P = 0.001). Özkan et al.Citation30 and Jones et al.Citation31 also reported this association between hand function and pain. Bagis et al.Citation18 and Jones et al.Citation31 implied that tenderness and pain had a negative effect on hand function.
There was no correlation between AUSCAN function score and grip strength. The hand OA patients had difficulty in carrying a bundle and handling small objects. Similarly, Zhang et al.Citation32 investigated the effects of symptomatic hand OA on the self-reported functional limitation and implied that symptomatic hand OA affects writing, carrying, and handling or fingering small objects. They suggested that hand OA affects the activities that require precise pinch grip more than power grasp.Citation32
The impact of functional limitations in the IP joints can differ from that in CMC joints, consequently, in the current work, US findings were used as a point of differentiation between the two subgroups of patients; those with only IP joint involvement and those with IP and first CMC joint affection. First CMC joint alone was not considered as a single entity because none of our patients had only CMC joint arthritis. Both patient subgroups were compared as regards VAS, AUSCAN, grip and pinch strength. Patients with symptoms at both sites experienced significantly higher levels of pain (P = 0.035) and functional impairment assessed by AUSCAN (P = 0.006). Although no cutoff values are available for AUSCAN, differences on the function subscale between those with and without CMC involvement seemed clinically relevant. Based on that, it seems that CMC joint OA adds more to pain and disability in symptomatic hand OA than IP joint OA alone. Bijsterbosch et al.Citation33 reported the same conclusion.
There was no significant difference in grip strength measurements between the two patient subgroups, whereas there was a significant decrease in pinch strength in those with both IP and CMC joint affection. Jones et al.,Citation31 who assessed patients by grip strength, did not support the hypothesis that first CMC OA is of greater clinical significance than DIP OA. They proposed that it is possible if they had included pinch strength in their evaluation this may have modified their conclusion.
Marshall et al.Citation34 investigated the relationship of OA at different hand joints and found that pain and functional limitations were highest in participants with both thumb and finger OA. This is in agreement with Dahaghin et al.,Citation35 who examined the relation between hand pain and OA of the different hand joints and showed that OA of the base of the thumb had the strongest association with hand pain. This supports the hypothesis that OA of the first CMC joint has a greater impact on pain than the other hand joints, due to the prominent role of the thumb in hand function.Citation35
5 Conclusion
Ultrasonographic findings correlated well with clinical findings as nodes, functional parameters as grip and pinch strength, and pain. The increased detection of OA structural pathology by US may make this a useful tool for hand OA assessment.
Notes
Available online 9 September 2011
Peer review under responsibility of Alexandria University Faculty of Medicine
References
- D.T.FelsonEpidemiology of hip and knee osteoarthritisEpidemiol Rev101988128
- J.NiuY.ZhangM.LaValleyC.E.ChaissonP.AliabadiD.T.FelsonSymmetry and clustering of symptomatic hand osteoarthritis in elderly men and women: the Framingham StudyRheumatology422003343348
- M.KloppenburgT.StammI.WattF.KainbergerT.E.CawstonF.N.BirrellResearch in hand osteoarthritis: time for reappraisal and demand for new strategiesAnn Rheum Dis66200711571161
- W.ZhangM.DohertyB.F.LeebL.AlekseevaN.K.ArdenJ.W.BijlsmaEULAR evidence-based recommendations for the diagnosis of hand osteoarthritis: report of a task force of ESCISITAnn Rheum Dis682009817
- A.LagnoccoE.FilippucciA.OssandonA.CiapettiF.SalaffiS.BasiliHigh resolution ultrasonography in detection of bone erosions in patients with hand osteoarthritisJ Rheumatol12200523812383
- B.MöllerH.BonelM.RotzetterP.M.VilligerH.R.ZiswilerMeasuring finger joint cartilage by ultrasound as a promising alternative to conventional radiograph imagingArthritis Rheum612009435441
- R.AltmanG.AlarconD.AppelrouthD.BlochK.BorensteinK.BrandtThe American Collage of Rheumatology criteria for the classification and reporting of osteoarthritis of the handArthritis Rheum33199016011610
- Wall PD, Melzack R, Katz J. Pain measurement in persons in pain, rating scales. Textbook of pain I, vol. 33, 3rd ed. UK: Longman Group; 1994. p. 338–9.
- K.D.AllenR.F.DeVellisJ.B.RennerV.B.KrausJ.M.JordanValidity and factor structure of the AUSCAN Osteoarthritis Hand Index in a community-based sampleOsteoarthr Cartil152007830836
- J.H.KellgrenLawrence JS: Radiological assessment of osteoarthrosisAnn Rheum Dis161957494502
- R.C.LawrenceC.G.HelmickF.C.ArnettR.A.DeyoD.T.FelsonE.H.GianniniEstimates of the prevalence of arthritis and selected musculoskeletal disorders in the United StatesArthritis Rheum411998778799
- J.A.BuckwalterJ.MartinH.J.MankinSynovial joint degeneration and the syndrome of osteoarthritisInstr Course Lect492000481489
- K.L.DominickJ.M.JordanJ.B.RennerV.B.KrausRelationship of radiographic and clinical variables to pinch and grip strength among individuals with osteoarthritisArthritis Rheum52200514241430
- J.L.Van SaaseL.K.van RomundeA.CatsJ.P.VandenbrouckeH.A.ValkenburgEpidemiology of osteoarthritis: Zoetermeer survey. Comparison of radiological osteoarthritis in a Dutch population with that in 10 other populationsAnn Rheum Dis481989271280
- J.H.KellgrenR.MooreGeneralized osteoarthritis and Heberden's nodesBMJi1952181187
- P.EggerC.CooperD.J.HartD.V.DoyleD.CoggonT.D.SpectorPatterns of joint involvement in osteoarthritis of the hand: the Chingford StudyJ Rheumatol22199515091513
- C.E.ChaissonY.ZhangT.E.McAlindonM.T.HannanP.AliabadiA.NaimarkRadiographic hand osteoarthritis: incidence, patterns, and influence of pre-existing disease in a population based sampleJ Rheumatol24199713371343
- S.BagisG.SahinY.YapiciO.CimenC.ErdoganThe effect of hand osteoarthritis on grip and pinch strength and hand function in postmenopausal womenClin Rheumatol222003420424
- I.KjekenH.DagfinrudB.Slatkowsky-ChristensenP.MowinckelT.UhligT.K.KvienActivity limitations and participation restrictions in women with hand osteoarthritis: patients’ descriptions and associations between dimensions of functioningAnn Rheum Dis64200516331638
- R.M.AchesonY.K.ChanA.R.ClemettNew Haven survey of joint diseases. XII. Distribution and symptoms of osteoarthrosis in the hands with reference to handednessAnn Rheum Dis291970275286
- W.GrassiG.LamannaA.FarinaC.CerviniSonographic imaging of normal and osteoarthritic cartilageSemin. Arthritis Rheum281999398403
- A.IagnoccoE.FilippucciA.OssandonA.CiapettiF.SalaffiS.BasiliHigh-resolution ultrasonography in detection of bone erosions in patients with hand osteoarthritisJ Rheumatol32200523812383
- C.L.LeeM.H.HuangC.Y.ChaiC.H.ChenJ.Y.SuY.C.TienThe validity of in vivo ultrasonographic grading of osteoarthritic femoral condylar cartilage: a comparison with in vitro ultrasonographic and histologic gradingsOsteoarthr Cartil162008352358
- H.I.KeenR.J.WakefieldA.J.GraingerE.M.A.HensorP.EmeryP.G.ConaghanAn ultrasonographic study of osteoarthritis of the hand: synovitis and its relationship to structural pathology and symptomsArthritis Rheum59200817561763
- I.MöllerD.BongE.NaredoE.FilippucciI.CarrascoC.MoraguesUltrasound in the study and monitoring of osteoarthritisOsteoarthr Cartil162008S4S7
- J.C.GersterG.RappoportJ.M.GinalskiPrevalence of periarticular calcifications in pyrophosphate arthropathy and their relation to nodal osteoarthritisAnn Rheum Dis431984255257
- F.M.CicuttiniJ.BarkerJ.D.HartT.D.SpectorRelation between Heberden's nodes and distal interphalangeal joint OST and their role as markers of generalised diseaseAnn Rheum Dis571998246248
- M.BaronE.DutilL.BerksonP.LanderR.BeckerHand function in the elderly: relation to osteoarthritisJ Rheum141987815819
- M.PattrickS.AldridgeE.HamiltonA.ManhireM.DohertyA controlled study of hand function in nodal and erosive osteoarthritisAnn Rheum Dis481989978982
- B.ÖzkanD.KeskinH.BodurN.BarçaThe effect of radiological hand osteoarthritis on hand function Clin Rheumatol26200716211625
- G.JonesH.M.CooleyN.BellamyA cross-sectional study of the association between Heberden nodes, radiographic osteoarthritis of the hands, grip strength, disability and painOsteoarthr Cartil92001606611
- Y.ZhangJ.NiuM.Kelly-HayesC.E.ChaissonP.AliabadiD.T.FelsonPrevalence of symptomatic hand osteoarthritis and its impact on functional status among the elderly: the Framingham studyAm J Epidemiol156200210211027
- J.BijsterboschW.VisserH.M.KroonT.StammI.MeulenbeltT.W.J.HuizingaThumb base involvement in symptomatic hand osteoarthritis is associated with more pain and functional disabilityAnn Rheum Dis692010585587
- M.MarshallD.Van der WindtE.NichollsH.MyersE.HayK.DziedzicRadiographic hand osteoarthritis: patterns and associations with hand pain and function in a community-dwelling sampleOsteoarthr Cartil17200914401447
- S.DahaghinS.M.A.Bierma-ZeinstraAz.GinaiH.A.P.PolsJ.M.W.HazesB.W.KoesPrevalence and pattern of radiographic hand osteoarthritis and association with pain and disability (the Rotterdam study)Ann Rheum Dis642005682687