Abstract
We report an Egyptian case with Brown–Vialetto–Van Laere syndrome. A five-year-old girl with progressive hearing loss was documented by brainstem auditory evoked potentials (BAEP) as sensorineural deafness, bilateral facial palsy and bilateral partial vocal cord paralysis in the paramedian position. There was no evidence of involvement of the upper motor neurons or spinal motor nerves. There is no similar case in the family.
1 Introduction
The Brown–Vialetto–Van Laere syndrome (BVVL) is a rare disorder characterized by sensorineural deafness followed or accompanied by cranial nerve disorders, usually involving the motor components of the facial and glossopharyngeal to hypoglossal nerves.Citation1,Citation2 It was first described by Brown in 1894,Citation3 and later by Vialetto in 1936Citation4 and Van Laere in 1966.Citation5,Citation6 The age of onset of the first symptoms varies ranging from infancy to the third decadeCitation6,Citation7. Fifty-eight cases of BVVL have been reported in just over a century. Around half of all cases are sporadic.Citation8
The majority of familial cases demonstrate autosomal recessive inheritance, although autosomal dominantCitation1,Citation9 and X-linked inheritanceCitation1 have been suggested in a few families. The female to male ratio is approximately 3:1 in reported cases.Citation7 Recently Green et al. identified a candidate gene, C20orf54, by studying a consanguineous family with multiple affected individuals and subsequently demonstrated that mutations in this gene were the cause of disease in other, unrelated families.
We reported the clinical and neurophysiological features of a patient with deafness, with cranial nerve involvement, and respiratory difficulties. This clinical picture and neurosensorial deafness suggest the diagnosis of pontobulbar palsy with sensorineural deafness or Brown–Vialetto–Van Laere syndrome.
2 Case report
A five-year-old girl was brought up by her parents who noticed progressive hearing loss. This was associated with dysphonia. Video laryngoscope was done and revealed bilateral partial vocal cord paralysis in the paramedian position. Subsequently, she suffered from severe respiratory distress and admitted to a hospital where a permanent tracheostomy was done. Two months later the mother noticed that her girl developed mask face (unable to smile), inability to close both eyes, excessive salivation with food accumulation at vestibules. Bilateral facial nerve paralysis was documented. The patient was referred to our hospital.
On admission, there were no motor or sensory complaints in both upper and lower limbs, and no sphincter disturbances. Prenatal, perinatal, and postnatal histories were free.
Her psychomotor development was normal. Vaccinations were given as scheduled.
Family history revealed positive consanguinity of first degree but there was no family history of similar condition.
By physical examination, the child was conscious, alert not distressed but uncooperative due to hearing loss. Tracheostomy tube was present. She had masked face, opened mouth, excessive salivation, mild deviation of the mouth angle to the left, unable to smile, cannot blow or purse mouth, cannot firmly close the eyes and cannot raise her eye brows. There were wasting and weakness of side to side tongue movement and fasciculations. Muscle tone and power as well as tendon reflexes were normal. There were no signs of wasting or sensory abnormalities in both upper and lower limbs.
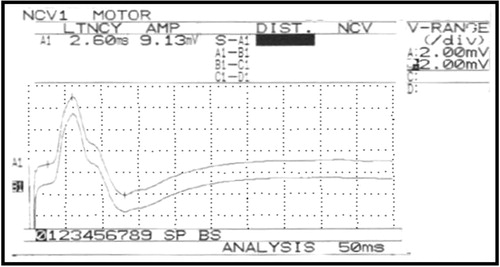
Electrophysiological study revealed: normal motor and sensory conduction studies of the peripheral nerves. Facial nerve conduction study to orbicularis oculi muscles showed low amplitude (left 0.27 mV and right 0.1 mV) and delayed latency (left 4 ms and right 4.4 ms) (). Normal facial conduction study to orbicularis oculi muscle ().
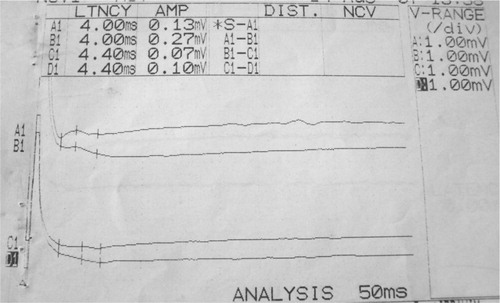
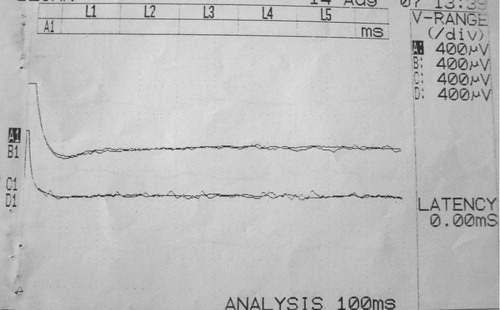
Poor response of the blink reflex (). Needle electromyography to orbicularis oculi and oris muscles showed motor unit drop out and polyphasicity. While muscles of the upper and lower limbs were normal. This was consistent with sever axonal degeneration of the facial nerve bilaterally.
Video laryngoscope revealed; ‘bilateral partial vocal cord paralysis in the paramedian position.
Brain stem auditory evoked potential (BAEP) revealed; bilateral severe sensory neural hearing loss at high frequency. Magnetic resonance image (MRI), blood chemistry, electrocardiogram and echocardiography, were unremarkable.
3 Discussion
The Brown–Vialetto–Van Laere syndrome (BVVL) is a rare neurological disorder of unknown etiology, characterized by progressive pontobulbar palsy associated with sensorineural deafness.Citation6
In our patient sensorineural deafness is the first symptom of the disease. Hearing loss has been consistently described at the onset of the disease both in familiar and non-familiar cases.Citation10
The sensorineural deafness was accompanied by multiple cranial nerve palsies involving the motor components of the 7th, 9th and 12th cranial nerves, but there was no evidence of involvement of the upper motor neurons or spinal motor nerves in our case. Together, the clinical findings suggested a diagnosis of progressive pontobulbar palsy with sensorineural deafness, or BVVL syndrome.
There are several conditions that closely resemble BVVL and that should always be considered in the differential diagnosis. It would be difficult to diagnose BVVL in a patient who initially presents with just sensorineural deafness. The development of other cranial nerve in conjunction with sensorineural deafness is likely to be needed to secure the diagnosis with any degree of confidence. The most closely related condition is the progressive bulbar paralysis of Fazio-Londe,Citation11 where the only distinguishing feature from BVVL is the absence of deafness. Another differential of BVVL is the Nathalie syndrome, which is a rare condition characterized by deafness in conjunction with spinal muscular atrophy, cataract, cardiac conduction defects and hypogonadism.Citation12 The Boltshauser syndrome, which is characterized by distal muscular atrophy with vocal cord paralysis and sensorineural hearing loss, is also very similar to BVVL.Citation13 However, in the former, the brainstem signs are restricted to vocal cord paralysis and the inheritance is likely to be autosomal dominant. Autosomal dominant inheritance is very uncommon in BVVL, with only two families reported.Citation1,Citation9 The Madras motor neuron disease (MMND) is another condition closely related to BVVL.Citation14 MMND is characterized by wasting and weakness of limb muscles, sensorineural deafness and multiple cranial nerve palsies usually affecting cranial nerves VII, IX and XII. Dysfunction of cranial nerves III and VI has not been reported in MMND.Citation15 Interestingly, one reported case of BVVL had a partial right bundle branch block on electrocardiographyCitation8 but our patient had normal echocardiography.
The etiopathogenesis of BVVL syndrome is still unknown and genetic transmission is quite variable; autosomal recessive, autosomal dominant, and X-linked inheritance, as well as autoimmune origin have been considered.Citation1,Citation9,Citation16 Recently, Green et al.Citation17 reported the identification of mutations in the C20orf54 gene as the cause of BVVL syndrome. Also. Bosch et al.Citation18 demonstrated that BVVL syndrome is associated with the riboflavin deficiency that resulted from a defect in the riboflavin transporter, encoded by the C20orf54 gene. As regards our patient there is no family history of similar condition even of hearing loss although there is a positive consangunity between the parents.
Laryngeal dyspnea and stridor due to paralysis of the vocal cords, which may lead to acute hospital admission with the mistaken diagnosis of croup, as was observed in our case, are early and striking manifestations in BVVL syndrome.Citation19
In our patient hearing loss has been reported as the first presentation; however, in case 2 of Gallai et al.Citation19 bulbar weakness at 20 months was the first evident symptom and hearing loss was never documented during life time but only at autopsy. Konstantinos et al.Citation16 reported a male infant with late onset hearing loss, Necropsy in this case revealed severe loss of axons and of myelin of the 8th nerve roots and heavy gliosis in the ventral cochlear nuclei. In our case, however, the deafness was documented by performing BAEP. The recognition of the onset of deafness without performing BAEP may be missed in infants and young children, especially those with simultaneous severe neurological problems.
The protracted cases may show a steady progression or a streaking irregular course with relapsing phases followed by periods of arrest and even partial improvement. Piccolo and co-workersCitation20 described the case of a sporadic BVVL with recovery from respiratory muscle failure. Gallai and coworkersCitation19 reported two cases characterized by improvement of dysphagia and motor performances. De Grandis and coworkersCitation9 described a case with clinical and neurophysiological improvement as well. The case we described showed a stationary course.
Investigations are usually done to exclude other causes or confirm the clinical signs of the patients. Neurophysiological studies demonstrate changes consistent with chronicCitation21–Citation24or activeCitation7,Citation8,Citation25 denervation in muscles. Motor nerve conduction velocities are usually normal.
Sensory action potentials are rarely reduced.Citation7,Citation9 The electrophysiological study of our patient showed poor response of the blink reflex with low amplitude of facial nerve conduction study and delayed latency that indicate severe loss of axons and myelin in the roots of the 7th cranial nerves. Normal peripheral conduction study with normal needle electromyography to muscles of the upper and lower limbs are going with the absence of spinal nerve involvement.
Brainstem auditory evoked potentials were abnormal when performed in 17 cases,Citation7,Citation1,Citation23,Citation26–Citation32as in our patient.
There are no MRI changes in our patient, although others reported changes in MRI in the form of atrophy of the brainstemCitation30,Citation31 and cerebellum,Citation30–Citation32 or hyperintensity in the brainstem nuclei.Citation26,Citation32
There is no specific treatment for BVVL. Supportive care and symptomatic treatment are the mainstays of management for this child. Steroids and immunoglobulins have been tried in several cases.Citation6,Citation33
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 3 December 2011
References
- S.A.HawkinsN.C.NevinA.E.HardingPontobulbar palsy and neurosensory deafness (Brown–Vialetto–Van Laere syndrome) with possible autosomal dominant inheritanceJ Med Genet271990176
- H.V.PrabhuM.J.S.BrownBrown–Vialetto–Van Laere syndrome: a rare syndrome in otologyJ Laryngol Otol11962005470472
- C.H.BrownInfantile amyotrophic lateral sclerosis of the family typeJ Nerv Ment Dis211894707716 Quoted from Ref. [6]
- E.VialettoContributo alla forma ereditaria della paralisi bulbare progressiveRiv Sper Freniat401936124 Quoted from Ref. [6]
- J.Van LaereParalysie bulbo-pontine chronique progressive familiale avec surdité. Un cas de syndrome de KlippelRev Neurol1151966289295 Quoted in Ref. [6]
- S.SathasivamBrown–Vialetto–Van Laere syndrome reviewOrphanet J Rare Dis320089
- K.A.VoudrisA.SkardoutsouA.VagiakouInfantile progressive bulbar palsy with deafnessBrain Dev242002732735
- A.MégarbanéI.DesguerresE.RizkallahV.DelagueR.NabboutA.BaroisBrown–Vialetto–Van Laere syndrome in a large inbred Lebanese family: confirmation of autosomal recessive inheritance?Am J Med Genet922000117121
- D.De GrandisP.PassadoreM.ChinagliaF.BrazzoR.RavenniP.CudiaClinical features and neurophysiological follow-up in a case of Brown–Vialetto–Van Laere syndromeNeuromusc Disord152005565568
- José AugustoMalheirosSarah TeixeiraCamargosJosé Teotoniode OliveiraFrancisco E.C.CardosoAbrazilian family with Brown Vialetto Van Laere syndrome with autosomal recessive inheritanceArq Neuropsiquiatr65120073235
- M.A.McShaneS.BoydB.HardingE.M.BrettJ.WilsonProgressive bulbar paralysis of childhood. A reappraisal of Fazio-Londe diseaseBrain115199218891900
- C.W.CremersB.G.Ter HaarT.J.Van RensThe Nathalie syndrome. A new hereditary syndromeClin Genet81975330340
- E.BoltshauserW.LangT.SpillmanE.HofHereditary distal muscular atrophy with vocal cord paralysis and sensorineural hearing loss: a dominant form of spinal muscular atrophyJ Med Genet261989105108
- E.MeenakshisundaramK.JagannathanB.RamamurthyClinical pattern of motor neuron disease seen in younger age groups in MadrasNeurol India18Suppl 31970109112
- A.NaliniB.K.YaminiN.GayatriK.ThennarasuR.GopeFamilial Madras motor neuron disease (FMMND): study of 15 families from southern IndiaJ Neurol Sci2502006140146
- Konstantinos A.VoudrisAngelikiSkardoutsouEleni A.VagiakouInfantile progressive bulbar palsy with deafness case reportBrain Dev242002732735
- P.GreenM.WisemanY.J.CrowH.HouldenS.RiphagenJ.P.LinBrown–Vialetto–Van Laere Syndrome, a ponto-bulbar palsy with deafness, is caused by mutations in C20orf54Am J Hum Genet862010485489
- A.M.BoschN.G.AbelingL.IJlstH.KnoesterW.L.PolA.E.StroomerBrown–Vialetto–Van Laere and Fazio Londe syndrome is associated with a riboflavin transporter defect mimicking mild MADD: a new inborn error of metabolism with potential treatmentJ Inherit Metab Dis342011159164
- V.GallaiJ.M.HockadayJ.T.HughesD.J.LaneD.R.OppenheimerG.RushworthPonto-bulbar palsy with deafness (Brown–Vialetto–Van Laere syndrome). A report on three casesJ Neurol Sci501981259275
- G.PiccoloE.MarchioniM.MaurelliF.SimonettiF.BizzettiF.SavoldiRecovery from respiratory muscle failure in a sporadic case of Brown–Vialetto–Van Laere syndrome with unusually late onsetJ Neurol2391992355356
- S.DiptiA.-M.ChildsJ.H.LivingstonA.K.AggarwalM.MillerC.WilliamsBrown–Vialetto–Van Laere syndrome: variability in age at onset and disease progression highlighting the phenotypic overlap with Fazio-Londe diseaseBrain Dev272005443446
- Ö.F.AydinD.ÖzcelikelN.SenbilY.K.Y.GürerBrown–Vialetto–Van Laere syndrome; the first Turkish caseActa Neurol Belg1042004111113
- S.SathasivamS.O'sullivanA.NicolsonP.J.TilleyP.J.ShawBrown- Vialetto-Van Laere syndrome: case report and literature reviewAmyotroph Lateral Scler Other Motor Neuron Disord142000277281
- R.J.DavenportC.J.MumfordThe Brown–Vialetto–Van Laere syndrome: a case report and literature reviewEur J Neurol119945154
- R.RamachandranNairM.ParameswaranA.S.GirijaVialetto–Van Laere syndrome in two sisters born to consanguineous parentsPediatr Neurol302004354355
- R.KoulR.JainA.ChackoA.AlfutaisiJ.HashimJ.ChackoPontobulbar palsy and neurosensory deafness (Brown–Vialetto–Van Laere syndrome) with hyperintense brainstem nuclei on magnetic resonance imaging: new finding in three siblingsJ Child Neurol212006523525
- J.M.AbarbanelP.AshbyA.Marquez-JulioK.R.ChapmanBulbo-pontine paralysis with deafness: the Vialetto–Van Laere syndromeCan J Neurol Sci181991349351
- H.NemotoS.KonnoN.NomotoN.WakataT.KuriharaA case of Brown–Vialetto–Van Laere (BVVL) syndrome in JapanClin Neurol452005357361
- J.MiaoH.LiH.LinC.SuY.LiuG.LeiSevere sleep disordered breathing in a patient with Brown–Vialetto–Van Laere syndrome: polysomnographic findingsJ Neurol Sci2632007214217
- D.A.FrancisJ.R.PonsfordC.M.WilesP.K.ThomasL.W.DuchenCase report. Brown–Vialetto–Van Laere syndromeNeuropathol Appl Neurobiol1919939194
- A.F.KocH.BozdemirY.SaricaMental retardation associated with Brown–Vialetto–Van Laere syndromeAmyotroph Lateral Scler Other Motor Neuron Disord4120035253
- J.A.MalheirosS.T.CamargosJ.T.de OliveiraF.E.C.CardosoA Brazilian family with Brown–Vialetto–Van Laere syndrome with autosomal recessive inheritanceArq Neuropsiquiatr6520073235
- V.GallaiJ.M.HockadayJ.T.HughesD.J.LaneD.R.OppenheimerG.RushworthPonto-bulbar palsy with deafness (Brown–Vialetto–Van Laere syndrome)J Neurol Sci501981259275