Abstract
Background
A hypercoagulable stable has been documented in patients with β-thalassemia. However, the underlying mechanisms are multifactorial. The role of soluble protein C endothelial receptor in hemostatic derangement in these patients has not been investigated.
Design and methods
Plasma soluble EPCR and markers of coagulation have been analyzed in 15 splenectomized patients (group I) and 15 non-splenectomized patients (group II).
Results
We showed significantly higher levels of sEPCR in patients versus the control and in group I more than group II. Levels of sEPCR positively correlated with total leukocytic and platelet counts. No correlation could be established between sEPCR and either age or sex.
Conclusion
The data indicate that high sEPCR levels could be implicated in the hemostatic derangement and endothelial cell dysfunction in patients with β-thalassemia.
1 Introduction
Thalassemia represents the most common hereditary hemolytic anemia which results from partial or complete lack of synthesis of one of the α or β globin chain of Hb.Citation1 β-Thalassemia is the most common type in Egypt with a carrier rate ranging from 5.3% to >9% and a gene frequency of 0.03%.Citation2
Patients with β-thalassemia exhibit thrombotic complications with several published series demonstrating the presence of both arterial and venous thrombosis.Citation3
The pathogenesis of this hypercoagulability is multifactorial implicating reactive oxygen species in the oxidized red cell membrane lipidsCitation4 and loss of their organization,Citation5 alterations in markers of coagulation activation and natural anticoagulant proteins,Citation6 thrombophilic DNA mutations,Citation7 endothelial, monocytic and granulocyte activation.Citation8 Endothelial protein C receptor (EPCR) is a type I transmembrane protein, mainly expressed on the luminal endothelial cell surface of large blood vessels.Citation9 It plays an anticoagulant role in hemostasis by binding to protein C with high affinity and it increases by more than 10 fold the generation of the activated protein C (APC). It also binds to factor VIIa and inhibits its coagulant activity.Citation10,Citation11
The soluble EPCR (sEPCR) is released from EPCR by thrombin, vascular injury or regulated proteolytic cleavage by metalloproteinases.Citation12,Citation13
2 Aim of the work
The aim of the present work was to estimate the plasma levels of sEPCR in patients with β-thalassemia.
3 Design and methods
Thirty adult patients with established β-thalassemia major were enrolled in this study, (15 splenectomized: group I and 15 non-splenectomized: group II) they were recruited from the Hematology Department of the Medical Research Institute. Thirty normal healthy individuals with matched age and sex served as control. They had no any history of venous thrombosis, renal dysfunction or smoking.
All patients and controls gave informed consent for enrollment in accordance with the Declaration of Helsinki and the study was approved by the Medical Research Institute Ethical Committee.
4 Methods
All patients were thoroughly examined. Laboratory investigations included CBC using automated cell counterCitation14 (Sysmex XT-1800i), PT and INR by quick one stage method using calcium thromboplastin, PTT with Kaolin (KCCT) using pathrombin,Citation15 D-dimer by semi-quantitative latex agglutination kit (DiALAB, Austria)Citation15 and estimation of sEPCR by ELISA (Stago diagnostica France).Citation16 Venous samples were withdrawn after 8–10 h fasting and prior to receiving blood transfusion. Plasma was separated immediately, INR, PTT and D-dimer were done at once and the remaining plasma was kept at −40 °C until processed for sEPCR assay.
4.1 Statistical analysis
Results were statistically analyzed using SPSS version 16A. Microsoft excel was used for graphing. All tests were two tailed and a 0.05 level of significance was used. Data were analyzed using the Kolmogorov. Smirnov test and Mann-Whitney test.
5 Results
Group I included six males (40%) and nine females (60%) with their age ranging from 19 to 59 years with a mean of 29.3 ± 12.2 years, while group II included four males (26.67%) and 11 females (73.33%) with their age ranging from 18 to 38 years with a mean of 23.4 ± 5.6 years. History of epistaxis was found in eight patients (26.7%) and history of thrombotic attacks (DVT and pulmonary embolism) in only two patients (6.7%). Clinical examination revealed hepatomegaly in all patients, while splenomegaly was evident in group II. In the other group (group I) none of them had spleen detected clinically due to previous splenectomy.
shows the hematological data of patients compared to the controls where the mean Hb concentration in patients was 7.6 ± 1.1g/dl while in the control group it was 13.2 ± 0.8 g/dl. The mean WBC count was 9.8 ± 2.9 × 109 L−1 in the cases whereas it was 6.9 ± 1.5×109 L−1 in the control group. As regard the platelet counts, it had a mean of 428.1 ± 193.9 × 109 L−1 in the patients group and a mean of 318.8 ± 70.6 × 109 L−1 in the control group. Nucleated RBCs were found in the peripheral blood of all the cases with a mean of 21.9 ± 38.6/100WBCs while they were absent in the peripheral blood of the control group. The absolute reticulocytic count ranged from 47,500 to 345,000 in the patients with a mean of 130,500 ± 11.2 while it ranged from 24,000-81,000 in the controls with a mean of 42,000 ± 1.3. Statistical analysis showed that there was statistical significant difference between patients and controls as regard Hb values, RBC counts, MCV, WBC counts(P = 0.000), platelets counts (P = 0.020) as well as normoblasts and reticulocytic counts (P = 0.000). On comparing the hematological parameters of group I and group II, platelet counts had a mean of 561.5 ± 150.7 × 109 L−1 in group I which was significantly higher than its mean values in group II (294,6 ± 130.4 × 109 L−1) (P = 0.000) as well as the normoblasts count which ranged from 5.0 -222.0/100WBCs with a mean of 34.0 ± 52.5 /100WBCs in group I whereas it ranged from 4.0 – 16.0/100WBCs with a mean of 9.8 ± 3.5/100WBCs in group II and the difference was statistically significant (P = 0.000) as shown in . Analysis of variance showed statistically significant difference between all thalassemic patients and normal control (P = 0.000) as regard the coagulation parameters as the mean INR was 1.2 ± 0.2 in patients and was 1.04 ± 0.01 in controls. On comparing both groups, the mean INR values in group I are higher than that of group II but with no statistical significant difference ( and ).
Table 1 Hematological parameters in patients compared to control.
Table 2 Hematological parameters in group I compared to group II.
Table 3 Coagulation parameters in patients compared to control.
Table 4 Coagulation parameters in group 1 compared to group 2.
As regard sEPCR level, it was significantly higher in patients than control (P = 0.008) (). Although group I had a higher mean level of plasma sEPCR compared to group II, yet the difference was not statistically significant (P = 0.709) (). But still there was a significant difference when each group was separately compared to the control (P = 0.021 and 0.048, respectively) ( and ).
Table 5 sEPCR level in patients compared to control.
Table 6 sEPCR level in group 1 compared to group 2.
Table 7 sEPCR level in group 1 compared to control.
Table 8 sEPCR level in group 2 compared to control.
D-dimer test was negative in all the studied groups (data not shown).
5.1 Correlation studies
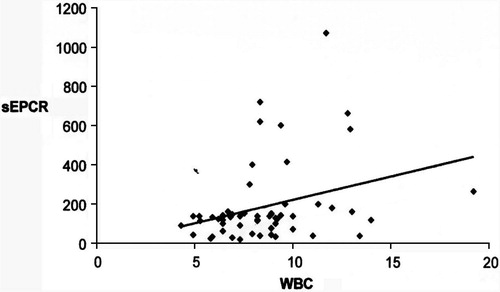
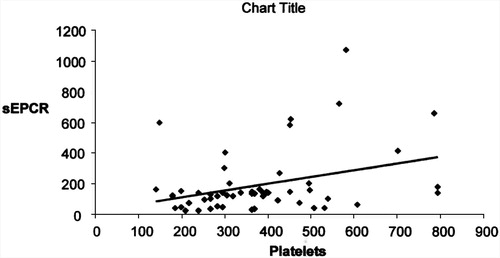
A significant positive correlation was observed between sEPCR and total leukocytic count (P = 0.015) as well as platelet count (P = 0.020) ( and ), respectively. But no correlation was found between sEPCR and age or sex.
6 Discussion
Profound hemostatic derangements are observed in patients with β-thalassemia. The chronic hypercoagulable state in these patients is multifactorial, and endothelial dysfunction has emerged as a causal factor in this hypercoagulability.Citation17,Citation18
In the present study, sEPCR was significantly higher in thalassemic patients than the control (P = 0.008). This may reflect a state of hypercoagulability, possibly induced by endothelial injury secondary to oxidative stress or platelet activation with subsequent release of procoagulant proteins. This is evidenced by the positive correlation with platelet count. A higher platelet count was observed in patients compared to the control (P = 0.02) especially in splenectomized patients (P = 0.000).
Setiabudy et al.Citation19 found higher platelet count in splenectomized versus non-splenectomized group. The hazards of thrombosis especially following splenectomy may range from portal vein thrombosis to pulmonary embolism and deep vein thrombosis.Citation19–Citation21 As platelets play an important role in the pathogenesis of thrombosis, autopsy based studies by Fucharoen and his colleaguesCitation22 in a large number of thalassemic patients documented striking pulmonary artery occlusions as well as another study done by Taher et al. had estimated the prevalence of thrombotic events in β-thalassemia in 9% of the patients.Citation23
In agreement with our findings, Mohren et al.Citation24 and Van't Riet et al.Citation25 also reported thromboembolic complications in splenectomized patients.
On the other hand, a higher mean platelet volume (MPV) was found in group I compared to group II reflecting a state of platelet hyperactivity. The enhanced platelet function added to the higher platelet number constitutes a double risk of hypercoagulability in splenectomized patients. These findings coincide with those of Setiabudy et al.Citation19 and they highlight the role of the platelets in inducing endothelial damage which is followed by enhanced production of sEPCR.
In the present study, D-dimer test was negative in all studied groups even in patients with the highest plasma levels of s EPCR which confirmed the study of Setiabudy et al.Citation19 who reported normal D-dimer in all their studied thalassemic patients.
In addition, we demonstrated a positive correlation between sEPCR and total leukocytic count (TLC). This was attributed to the fact that the activated neutrophils and monocytes in thalassemic patients release their proteolytic enzymes with production of free oxygen radicals as well as inflammatory cytokines that damage the endothelium which eventually produce EPCR degradation into its soluble form. This agrees with Boossma et al.Citation26 who studied plasma levels of sEPCR in cases of Wagener granulomatosis and found a positive correlation between their levels and disease activity.
As regards the INR and PTT, they were found prolonged in 86.7% and 83.3% of the patients and were statistically significant compared to the control (P = 0.000, P = 0.000), respectively. Similarly, Naithani et al.Citation27 found prolongation of INR in 40.7% and PTT in 46.3% of their patients.
Epistaxis was found in 26% of our patients in agreement with the findings of Naithani et al.Citation27 study, in which sixteen out of the studied 54 thalassemic patients had bleeding manifestations. Altered liver functions, and poor chelation might be risk factors for altered hemostasis in these patients. In their study, they reported low protein C, protein S and antithrombin III as well as Eldor et al.Citation17 and Sivgar et al.Citation28 who found significantly decreased levels of these anticoagulant proteins which were explained by combined consumption and liver dysfunction.
In the present study, no correlation was found between sEPCR and age as our patients were adults. Recently, Orhon et al.Citation29 reported higher levels in healthy children compared to healthy adults. Similarly, Kuraswa et al.Citation28 found a negative correlation between sEPCE level and age of the pediatric group, but they failed to establish this negative correlation in the adult group. The higher level of sEPCR in healthy children suggests a regulatory mechanism for the protein C system over the first years of life, as the highest level of sEPCR in their study, was found in the first year of life.Citation28
As regards gender, we could not establish a relation between gender and sEPCR. On the contrary, Orhon et al.Citation29 found higher levels in males and were attributed to environmental factors including smoking.
In conclusion, our study documented increased sEPCR in patients with β-thalassemia which could be implicated in the hemostatic derangement in these patients. Hence, close monitoring of the hemostatic system in thalassemia is highly recommended especially with increasing age and in splenectomized patients to avoid the morbid complications of hypercoagulability .
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 25 September 2012
References
- Thein SL, Rees D. Hemoglobin and the inherited diseases of globin synthesis. In: Hoffbrand Av, Catovsky D, Tuddenham EG, Green AR, editors. Postgraduate haematology, 6th ed., vol. 6, 2011. p. 83–107.
- A.ElbeshlawyI.YossryPrevention of hemoglobinopathies in EgyptHemoglogin332009420
- K.I.AtagaM.D.CappelliniE.A.Rachmileuritzβ-Thalassemia and sickle cell anaemia as paradigms of hypercoagulabilityBJH1392007313
- D.TavazziDucalG.GraziadeiA.CominoG.FiorelliM.D.CapalliniMembrane-bound iron contributes to oxidative damage of beta-thalassemia intermedia erythrocytesBJH11220014850
- S.GandrilleEndothelial cell protein C receptor and the risk of venous thrombosisHaematologica932008812816
- M.RiewaldR.J.PetrovanA.DonnrM.RufActivated protein C signals through the thrombin receptor PAR1 in endothelial cellsJ Endotoxin Res92003317321
- P.A.ZallouaShbaklottY.A.MouradS.KoussaTahertIncidence of thromboembolic events in Lebanese thalassemia intermedia patientsThrombosis Haemostaisis892003767788
- P.ButhepS.RummavasR.WisedpanichkijS.FucharoenIncreased circulating activated endothelial cells, vascular endothelial growth factor, and tumour necrosis factor in thalassemiaAm J Hematol702002100106
- S.GhoshU.R.PendurthiA.SteinoeC.T.EsmonV.MohanL.RaoEndothelial cell protein C receptor acts as a cellular receptor for factor VIIa on endotheliumJ Biol Chem28220071184911857
- J.Lopez-SagasetaR.MontesC.PuyN.DiezK.FukudomeJ.HermidaBinding of factor VIIa to the endothelial cell protein C receptor reduces its coagulant activityJ Thromb Haemost5200718171824
- J.XuD.QuN.L.EsmonC.T.EsmonMetalloproteolytic release of endothelial cell protein C receptorJ Biol Chem275200060386344
- J.M.GuY.KatsuraG.L.FerrellP.GrammasC.T.EsmonEndotoxin and thrombin elevate rodent endothelial cell protein C receptor mRNA levels and increase receptor shedding in vivoBlood95200016871693
- D.QuY.WangN.L.EsmonC.T.EsmonRegulated endothelial protein C receptor shedding is mediated by tumor necrosis factor-converting enzyme/ADAM17J Thromb Haemost52007395402
- Bain BJ, Lewis SM, Bates I. Basic hematological techniques. In: Bain BJ, Lewis SM, Bates I, editors. Dacie and Lewis practical hematology, 10th ed., vol. 3, 2006. p. 25–7.
- Laffan M, Manning R. Investigations of haemostasis. In: Bain BJ, Lewis SM, Bates I, editors. Dacie and Lewis practical hematology, 10th ed., vol. 16, 2006. p. 379–440.
- R.LequinEnzyme immunoassay (EIA)/enzyme-linked immunosorbent assay (ELIZA)Clin Chem51200524112415
- A.EldorE.A.RachmilewitzThe hypercoagulable state in thalassemiaBlood9920023643
- A.M.HassnM.A.FallouziPortal vein thrombosis following splenectomyBr J Surg872000362373
- R.SetiabudyP.A.WahidiyatL.SetiawanPlatelet aggregation and activation in thalassemia major patients in IndonesiaClin Appl Thromb/Hemost142008346351
- F.S.FujitaS.LyassPortal vein thrombosis following splenectomy: identification of risk factorsAm J Surg692003951956
- M.IkadaM.SekimotoHigh incidence of thrombosis of the portal vein system after laparoscopic splenectomy: a prospective study with contrast enhanced CT scanAnn Surg2412005205216
- S.FucharoenP.WinichagonThalassemia and abnormal hemoglobinInt J Hematol7620028389
- A.TaherH.Isma'eelG.MehioD.BignaminiA.KattamisE.A.RachmilewitzPrevalence of thromboembolic events among 8,860 patients with thalassaemia major and intermedia in the Mediterranean area and IranThromb Haemost962006488491
- M.MohranMarkmannV.DworochakThromboembolic complications after splenectomy for hemolytic diseasesAm J Hematol762004143146
- M.Vant RietJ.W.BurgerDiagnosis and treatment of portal vein thrombosis following splenectomyBr J Surg87200012291233
- M.M.BoomsmaD.J.Stearns-KurosawaC.A.StegmanE.RaschiP.L.MeroniS.KurosawaPlasma levels of soluble endothelial cell protein C receptor in patients with Wegener's granulomatosisClin Exp Immunol1282002187194
- R.NaithaniJ.ChandsaS.NarayanThalassemia major on the verge of bleeding or thrombosisHematology1120065761
- S.T.SivgerF.A.KuypersL.StylesPulmonary hypertension in thalassemia: association with platelet activation and hypercoagulable stateAm J Hematol812006670675
- F.S.OrhonH.FrgunY.EginB.UlukolS.BaskanN.AkarSoluble endothelial protein C receptor levels in healthy populationJ Thromb Thrombol2920104651