Abstract
Background
Pilocytic astrocytomas are the second overall most common pediatric brain tumor. Magnetic resonance (MR) imaging is widely used in the diagnosis and follow up of pediatric patients with pilocytic astrocytomas because of its ability to provide anatomical detail. However conventional MR imaging does not provide information about tissue biochemistry.
Aim of the work
To study the role of proton magnetic resonance spectroscopy in diagnosis of pilocytic astrocytoma in children.
Subjects and methods
This study included seven pediatric patients with histopathologically proven pilocytic astrocytoma. All patients were subjected to full history taking and thorough clinical examination. Magnetic resonance (MR) imaging was performed at 1.5 Tesla MR system using a standard head coil. Imaging included conventional MRI and proton magnetic resonance spectroscopy. Proton magnetic resonance spectroscopy was done using either single or multi-voxel technique. Surgical biopsy was then performed to all patients and correlation with histopathological data was done.
Results
Out of the seven patients included in this study, six were females and one was male with mean age of 9.5 years, the tumor was located in five of them in the posterior fossa, located in right thalamo-peduncular region in one patient and located in the hypothalamic–chiasmatic region in one patient.
MR spectroscopic study showed the same findings in all the lesions including high Cho/NAA and Cho/Cr ratios (3.53 ± 1.5) and (7.21 ± 4.2), respectively, relative low concentration of creatine with increased NAA/Cr ratio (2.32 ± 1.1). Lactate doublet was detected in all cases while no lipid peaks were detected.
Conclusion
Based on the findings in this study we suggest that pilocytic astrocytoma has a specific spectroscopic metabolic profile which could be diagnostic for this type of tumor.
1 Introduction
Pilocytic astrocytomas represent only 5–10% of all cerebral gliomas, but account for nearly about one third of the pediatric glial neoplasms. They are the second overall most common pediatric brain tumor. Their main locations are around the third and fourth ventricles. Nearly half are found in the optic chiasm and hypothalamus and about one third are located in the cerebellar vermis and hemispheres. Brain stem and basal ganglia are less common locations. They are typically tumors of children and young adults. Cerebellar tumors usually have a peak incidence at age of 10. Cerebral hemispheric tumors usually occur a decade later with a peak age of 20. Three quarters of optic pathway lesions occur under 12 years of age.Citation1
Pilocytic astroctomas are well circumscribed but unencapsulated masses which are classified as WHO grade I. Their gross and radiological appearances vary according to location. Those located in the cerebellum tend to be cystic with internal solid mural nodule. Those located in the optic-hypothalamic region tend to be solid and well circumscribed while those located in the brainstem are usually solid and infiltrating and some time tend to be cystic.Citation2
Magnetic resonance (MR) imaging is widely used in the diagnosis and follow up of pediatric patients with pilocytic astrocytomas because of its ability to provide anatomical detail. However conventional MR imaging does not provide information about tissue biochemistry.Citation3
Proton MR spectroscopy is a non invasive in vivo technique that provides additional metabolic diagnostic indices beyond anatomic information and has been used widely in the imaging of brain tumors and other CNS pathologies. Several studies have shown that MR spectroscopy can help differentiate common pediatric brain tumors.Citation4
The purpose of this study is to demonstrate different MR spectroscopic findings of pilocytic astrocytoma in children and to assess if there are certain specific spectroscopic findings which could be considered as diagnostic for this type of tumor.
2 Methods
The present study included seven patients in pediatric age group admitted to Alexandria university hospitals presenting with brain tumors histopathologically diagnosed as pilocytic astrocytomas after surgical biopsy.
All the patients were subjected to thorough history taking and clinical examination, conventional magnetic resonance imaging and magnetic resonance spectroscopic study. Correlation with histopathological data was done in all patients after surgical biopsy.
Magnetic resonance imaging was performed at 1.5 Tesla MR system using a standard head coil on Siemens Magnetom Avanto (Siemens, Erlangen, Germany). Patients were subjected to the following MRI protocols: Axial T2 weighted turbo spin echo (T2 TSE) (repetition time (TR) of 3000 ms, an echo time (TE) of 120 ms, a slice thickness of 4 mm, FOV = 230 × 230 mm), Axial T2 FLAIR (a repetition time (TR) of 8000 ms, an echo time (TE) of 100 ms, TI of 2200 ms, a slice thickness of 4 mm and FOV = 230 × 230 mm), pre-contrast axial T1 weighted spin echo (T1 SE) (a repetition time (TR) of 650 ms, an echo time (TE) of 15 ms, a slice thickness of 4 mm, FOV = 230 × 230 mm), axial, sagittal and coronal T1 weighted spin echo (T1 SE) after intravenous administration of 0.1 mmol/kg of dimeglumine gadopentate (Magnevist, Schering, Berlin, Germany). Patients who needed sedation were given the sedative dose of thiopental sodium 3 mg/kg. Incremental doses were given when needed.
Magnetic resonance spectroscopy (MRS) single or multi-voxel (CSI) was done by using point resolved spectroscopy (PRESS) sequences. Multi-voxel spectroscopy was performed using intermediate echo time of 135 ms (TR 1500 ms, FOV 160 mm) or short echo time of 30 ms (TR 1500 ms, FOV 160 mm) When multi-voxel spectroscopy was not possible because of the small size of the lesion, we used singe voxel spectroscopy (cubic voxel of 2 cm side length) of intermediate TE 135 ms (TR 1500 ms) or short TE 30 ms (TR 1500 ms).
Spectra were generated by the standard Siemens scanner software. Peak assignment was as follows: N-acetyl aspartate (NAA) at 2.0 ppm shift; choline (Cho) at 3.2 ppm; creatine (Cr) at 3.02 ppm and myo-inositol (mIns) at 3.65 ppm. The software also determined the area under each of these peaks by fitting them to standard curves. The areas under the peaks are proportional to the metabolite concentrations. Metabolite ratios (i.e. Cho/Cr, Cho/NAA, NAA/Cho, etc.) were calculated automatically by the workstation software.
3 Results
This study included seven patients with histopathological diagnosis of pilocytic astrocytoma, six were females and one was male with mean age of 9.5 years, the tumor was located in five of them in the posterior fossa, located in right thalamo-peduncular region in one patient and located in the hypothalamic–chiasmatic region in one patient.
3.1 Conventional MRI study
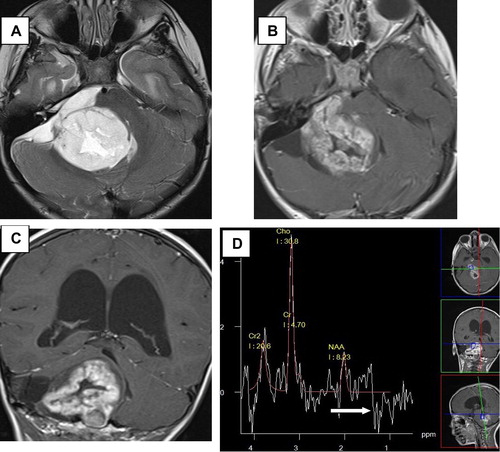
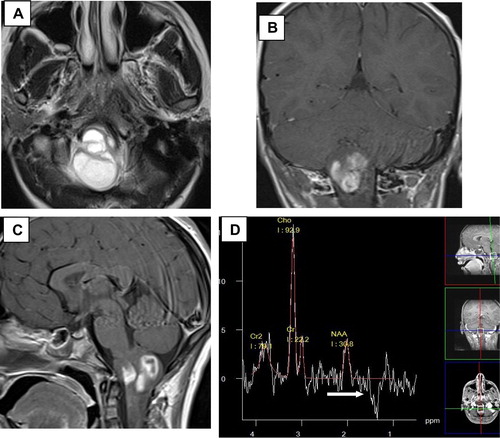
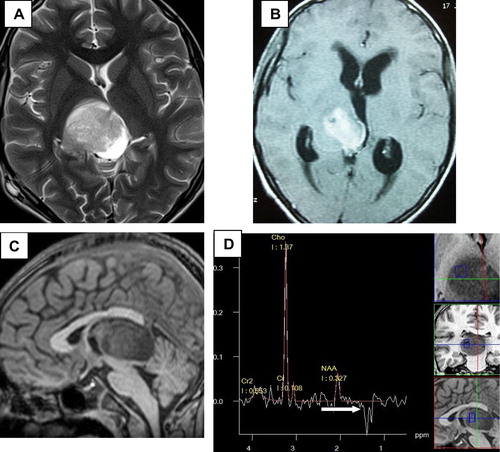
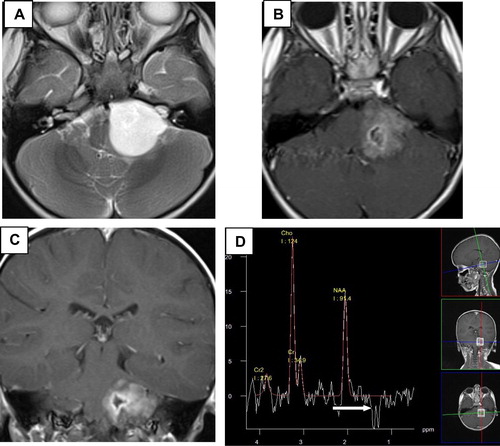
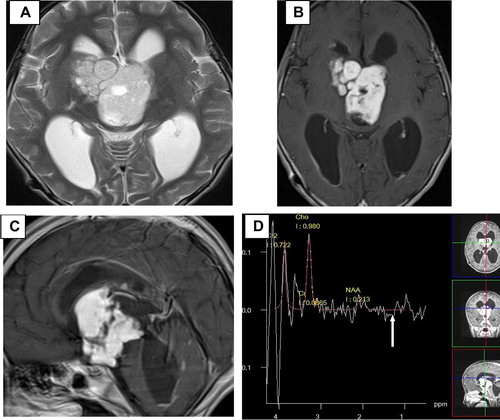
All the lesions showed heterogeneous signal with mixed solid and cystic components notably exhibiting hypointense signal in T1WI and hyperintense signal in T2WI. All of the lesions showed heterogeneous enhancement after contrast administration.
3.2 MRS analysis
| • | Increased Cho/NAA ratio; ranging from 1.35 to 6.07 with mean ratio 3.53 ± 1.5. | ||||
| • | Increased Cho/Cr ratio; ranging from 1.64 to 12.75 with mean ratio 7.21 ± 4.2. | ||||
| • | Increased NAA/Cr ratio; ranging from 0.27 to 3.5 with mean ratio 2.32 ± 1.1. | ||||
| • | Decreased Cr/Cho ratio; ranging from 0.08 to 0.61 with mean ratio 0.21 ± 0.19. | ||||
| • | Lactate doublet was detected in all cases. | ||||
| • | No lipid peak was detected. | ||||
shows a summary of the spectroscopic MRI findings in the seven patients included in the study.
Table 1 Summary of the spectroscopic MRI findings in the seven patients included in the study.
– show a demonstration for the MRI conventional and spectroscopic findings in five patients included in the study.
4 Discussion
In our study, we had seven patients with histopathologically proven pilocytic astrocytoma, five of them were in the posterior fossa and the remaining two were in supratentorial location and we found that pilocytic astrocytomas had specific metabolic profile that was demonstrated in all our cases, with no notable difference between supra- and infratentorial ones.
The spectra of pilocytic astrocytoma revealed high Cho/NAA and Cho/Cr ratios (3.53 ± 1.5) and (7.21 ± 4.2), respectively, relative low concentration of creatine with increased NAA/Cr ratio (2.32 ± 1.1). Lactate doublet was detected in all cases while no lipid peaks were detected.
Our results were in agreement with the previous studies which evaluated the role of MRS in the assessment of pilocytic astrocytoma.
Hwang et al.Citation5 found that pilocytic astrocytoma has relatively high Cho/NAA and Cho/Cr ratios (3.4 ± 2.14) and (3.46 ± 1.46) respectively with an elevated lactate doublet which was observed in all the studied cases. No dominant lipid peak was observed.
Cicel et al.Citation6 stated that pilocytic astrocytomas exhibit elevated lactate, and Cho and diminished levels of NAA, Cr, and mIns, and in contrast to Hwang et al.,Citation5 Cecil et al.Citation6 stated that elevated lipid was also found.
Our study was also in agreement with Panigrahy et al.Citation7 who found that the pilocytic astrocytoma had relatively low Cr and increased NAA/Cr ratio (1.8 ± 1.2) as compared to (2.32 ± 1.1) in our study.
Wang et al.Citation8 used long-echo-time MRS to classify pediatric cerebellar tumors with accuracy about 85% by using Cr/Cho and NAA/Cho ratios. They found low-grade astrocytomas and ependymomas had higher NAA/Cho ratio as compared to primitive neuroectodermal tumors.
An elevated lactate peak reflects anaerobic metabolism; surprisingly, this is not well correlated with tumor grade in the pediatric population.Citation6
Kugel et al.Citation9 reported the lack of correlation between lactate signal and tumor grade. High lactate signal could be found in both benign and malignant tumors.Citation5
Sutton et al.Citation10 found lactate peak in nearly all 25 pediatric gliomas studied, regardless of grade.
Multiple mechanisms were suggested by Hwang et al.Citation5 to explain the high lactate concentration in this benign tumor. They suggested that high lactate concentration may be due to abnormal number or dysfunction of mitochondria, which would interfere with the process of oxidative phosphorylation and electron transport, alterations in proportional oxygen delivery, and oxygen extraction or usage by tumor or anaerobic glycolysis by tumor cells.
In three cases, and by using multi-voxel spectroscopy due to the large size of the lesions, we found no metabolic abnormalities outside the enhancing tumor bed reflecting its benign non aggressive behavior of this WHO grade I tumor. That was also demonstrated in a previous study by Morales et al.Citation11 who found an elevation in Cho/Cr ratios in the peritumoral regions of two cases of pilomyxoid astrocytoma in comparison with pilocytic astrocytoma, reflecting the more aggressive and infiltrative behavior of the former tumor.
Harris et al.Citation12 observed that the MRS spectra of pilocytic astrocytomas have low signal to noise ratio which may be due to their low cellularity compared with other tumors and this characteristic may be a useful discriminator for these tumors.
Finally based on the findings of our study in correlation with the findings of the previously mentioned studies we could suggest that pilocytic astrocytoma has a specific metabolic profile which is characterized by low creatine, elevated choline/creatine and N-acetyl aspartate/creatine ratios with the presence of lactate doublet at 1.3 p.p.m. So we recommend that MR spectroscopy should be a part of the routine MR examination for cases with suspected pilocytic astrocytoma as it could increase the imaging diagnostic efficiency of such tumors even before surgical removal and histopathological examination.
Notes
Available online 23 January 2012
Peer review under responsibility of Alexandria University Faculty of Medicine.
References
- P.Tortori-DonatiA.RossiR.BiancheriM.L.GarrèA.CamaBrain Tumors. Pediatric Neuroradiology2005SpringerBerlinp.329–436
- T.Y.PoussaintDiagnostic imaging of primary pediatric brain tumors. Diseases of the brain, head & neck, spine2008SpringerBerlinp.277–87
- T.Y.PoussaintMagnetic resonance imaging of pediatric brain tumors: state of the artTopics in Magnetic Resonance Imaging1262001411433
- D.P.SoaresM.LawMagnetic resonance spectroscopy of the brain: review of metabolites and clinical applicationsClin Radiol64120091221
- J.H.HwangG.F.EgnaczykE.BallardR.S.DunnS.K.HollandW.S.BallJrProton MR spectroscopic characteristics of pediatric pilocytic astrocytomasAJNR Am J Neuroradiol1931998535540
- K.M.CecilB.V.JonesMagnetic resonance spectroscopy of the pediatric brainTop Magn Reson Imaging1262001435452
- A.PanigrahyM.D.KriegerI.Gonzalez-GomezX.LiuJ.G.McCombJ.L.FinlayQuantitative short echo time 1H-MR spectroscopy of untreated pediatric brain tumors: preoperative diagnosis and characterizationAJNR Am J Neuroradiol2732006560572
- Z.WangL.N.SuttonA.CnaanJ.C.HaselgroveL.B.RorkeH.ZhaoProton MR spectroscopy of pediatric cerebellar tumorsAJNR Am J Neuroradiol169199518211833
- H.KugelW.HeindelR.I.ErnestusJ.BunkeR.du MesnilG.FriedmannHuman brain tumors: spectral patterns detected with localized H-1 MR spectroscopyRadiology18331992 Jun701709
- L.N.SuttonZ.WangD.GusnardB.LangeG.PerilongoA.R.BogdanProton magnetic resonance spectroscopy of pediatric brain tumorsNeurosurgery3121992195202
- H.MoralesL.KwockM.CastilloMagnetic resonance imaging and spectroscopy of pilomyxoid astrocytomas: case reports and comparison with pilocytic astrocytomasJ Comput Assist Tomogr3152007682687
- L.M.HarrisN.DaviesL.MacPhersonK.FosterS.LateefK.NatarajanThe use of short-echo-time 1 H MRS for childhood cerebellar tumours prior to histopathological diagnosisPediatric Radiology3711200711011109