Abstract
Introduction
Despite advances in perioperative care and operative techniques, urgent colorectal operations are still associated with higher mortality and morbidity than elective surgery.
Aim
This study was to identify the challenge in diagnosis and treatment of emergencies caused by colon carcinoma; and to assess its outcome.
Material and methods
This included 59 consecutive patients treated with emergency surgical intervention for colonic carcinoma; and other 59 patients of elective colonic surgery.
Results
Morbidity rates were 27.1% versus 10.2% after emergency and elective surgery. Rates of 1-, 2- and 3-year survival were 64.4%, 57.6% and 47.5% respectively after emergency surgery; and 71.2%, 62.7% and 50.8% respectively after elective surgery.
Conclusions
Challenge included presentation of undiagnosed patients with difficult or impossible colon preparation, colonoscopy, tissue biopsy or tumor staging; in addition to associated diseases and/or old age. Mortality and morbidity rates after emergency surgery were higher than elective surgery. Selection of the surgical procedure was guided by the tumor staging, co-morbidities and intraoperative assessment. Emergency resection, when possible, could approximate survival of elective resection. Total colectomy could obtain good outcome and survival when compared to other emergency procedures.
1 Introduction
Despite advances in perioperative care and operative techniques, urgent colorectal operations are still associated with higher mortality and morbidity than elective surgery.Citation1 About 10% of all operations for colon carcinoma are performed in emergency situations because of severe preoperative complications. Urgent surgery in colon carcinoma is usually performed for advanced tumors of elderly patients. The diagnosis and treatment can be a challenge for the treating surgeon.Citation2
Severe complications of colonic carcinoma may be the first presentation of colon carcinoma. In addition, the treatment of acutely obstructed carcinoma of the left colon and sigmoid colon still represent a matter of controversy.Citation3 The aim of this study was to identify the challenge in the diagnosis and treatment of emergencies caused by colon carcinoma; and to assess the outcome of these emergencies.
2 Methods
This study included 118 patients treated by surgery for colon carcinoma. This included 59 consecutive patients with emergency presentation of colonic malignancy; in addition to another 59 patients treated by elective colonic surgery. This study was approved by the Ethics Committee in Faculty of Medicine; Alexandria University.
The patients of emergency presentation were subjected to: detailed medical history, complete clinical examination, routine laboratory investigations and abdominal imaging by CT. Plain abdominal X-ray in standing position was done for patients with suspected intestinal obstruction.
Emergency surgical intervention was performed for 59 patients. Evaluation of the patients was done both preoperatively and intraoperatively. For each patient, a preoperative consent was signed for colectomy and intestinal stoma to be able to deal with different conditions. The emergency surgical procedures were determined by the location of the tumor, resectability, associated medical diseases and risk of the procedure. Resection with primary anastomosis was performed for resectable tumors with unloaded colon in patients without associated high risk of leakage. Hartmann's procedure was performed for resectable tumors with associated risk of leakage. Total colectomy was done for resectable tumors with heavily loaded colon. Right hemicolectomy was done for resectable tumors in the right side. Intestinal stoma was performed for unresectable tumors. Intraoperative colonic lavage was done before primary anastomosis.
The early postoperative period of emergency was assessed for any complications. Follow up was done every 3 months during the first year then every 6 months after the first year. The follow up included clinical assessment, tumor markers, abdominal ultrasonography and abdominal CT.
Similar assessment was done for 59 patients treated by elective surgery for colonic carcinoma.
2.1 Statistics
The median and percentage values were calculated for many data. The student t test was used to compare parameters of the two groups. Fisher exact test was used to compare complications of both groups. The value of p was significant if ⩽0.05 The Kaplan Meier survival curves were used to illustrate postoperative survival.
3 Results
Fifty nine patients with emergency presentation of colonic malignancy were included in this study. They were 38 (64.4%) males and 21 (35.6%) females. Their mean age was 59.27 ± 8.07 years. The emergency clinical presentation included intestinal obstruction in 54 (91.5%) patients, acute abdomen due to colonic perforation in 2 (3.4%) patients and accidental discovery during appendectomy and cholecystectomy in 2 (3.4%) patients and bleeding per rectum in one (1.7%) patient. Associated co-morbidities were detected in 15 (25.4%) patients and included uncontrolled diabetes, liver cirrhosis, ischemic heart disease and hypertension.
The laboratory workup showed anemia in 24 (40.6%) patients, impaired liver functions in 10 (16.9%) patients, elevated CEA in 43 (72.9%) patients and uncontrolled diabetes mellitus in 5 (8.4%) patients.
Plain abdominal X-ray in standing position revealed dilated intestinal loops with multiple air-fluid levels in 54 patients. Abdominal CT visualized the obstructed dilated intestinal loops in 54 obstructed patients; and visualized the tumors in 49 (83%) patients. These tumors were in the recto-sigmoid region in 45 (76.3%) patients, left side of colon in 10 (16.9%) patients, right side of colon in 4 (6.8%) patients.
Emergency operations were done for 54 patients with obstruction, 2 with peritonitis due to tumor perforation one with severe bleeding and 2 accidentally discovered. Resectability was possible in 46 (78%) patients. The resectable tumors were mobile, without distant spread, ascites, para-aortic lymph nodes nor peritoneal seeding. Median operative time was 200 min and median intraoperative blood loss was 500 ml. More data for emergency and elective patients are shown in ().
Table 1 Preoperative demographic, operative and postoperative data.
The data of 59 patients of emergency colonic operations were compared to another 59 elective operations for colon carcinoma. There was no significant difference in age and gender between emergency and elective groups. The intraoperative manifestations of advanced unresectable tumors were more in emergency group () and included fixed tumors, liver metastases, peritoneal seeding, ascites and para-aortic lymph nodes. The surgical procedures for both emergency and elective patients and their outcome are shown in ().
Challenge and difficulties in emergency operations included unprepared colon, neither enough time nor feasibility of full investigations, associated diseases (co-morbidities), tumor perforation with peritonitis and accidental discovery during another operation.
Postoperative complications of emergency patients occurred in 16 (27.1%) patients; while complications of elective surgery were found in 6 patients (10.2%). These data are shown in (). The difference is significant with FE p = 0.032. Survival 1-, 2- and 3-year survival rates of operated emergency patients were 64.4%, 57.6% and 47.5% respectively (). Emergency resection of resectable tumors could achieve outcome and survival approximating the elective resection. The patients treated by total colectomy had 54.5% 3-year survival; this was the best survival among other surgical procedures. The majority of mortality after emergency surgery (62.7%) during follow up was associated with advanced tumor stage, old age >60 years and the presence of associated diseases. The 1-, 2- and 3-year survival rates of operated elective patients were 71.2%, 62.7% and 50.8% respectively. Although the mortality in emergency group is more than elective group, the difference in not significant. This can be explained by our trend of tumor resection in emergency surgery when resectable.
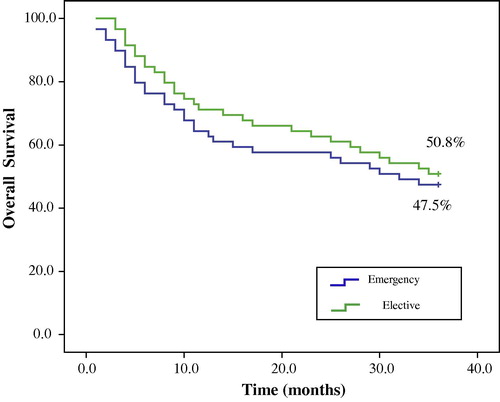
Table 2 Postoperative complications of emergency and elective patients.
4 Discussion
The emergency presentation of complicated colonic cancer is a challenge in diagnosis and treatment. Emergency surgical management of colon cancer remains controversial and is still associated with increased risk of morbidity and mortality.Citation4–Citation7 Currently, the mechanisms that worsen the prognosis of complicated colon cancer are still not well known. Complicated colon cancer presents in more advanced stages and have a worse overall long-term prognosis than uncomplicated tumor. Tumor stage is the most important prognostic factor for cancer of colon. In addition, the outcome is affected significantly by the associated medical diseases. Acute bleeding from tumors of the gastrointestinal tract is not the absolute sign of the patient being inoperable. In the majority of patients’ emergency presentation, resection is feasible. Advanced age is not a contraindication to radical surgery in case of colorectal emergency in the elderly.Citation8–Citation12
In this study, all patients with colonic carcinoma presenting as an emergency condition were neither diagnosed nor investigated before presentation. Intestinal obstruction, bleeding or perforation were the first signs of presentation of colonic carcinoma. The obstructing tumors were not visualized by abdominal CT in 10 (16.9%) patients. Ultrasonography could not give good data in the presence of dilated intestinal loops. Usually there was no available tissue biopsy. Colonoscopy was impossible for emergency obstruction and unprepared colon. Also severe bleeding in unprepared colon hindered colonoscopy and made the colon full of blood clots. Also, the presence of other medical diseases affected the fitness of many patients. Preoperative accurate staging was usually difficult.
The treatment of the obstruction due to left colon carcinoma beyond left flexure is not standardized. Current surgical options are intraoperative lavage and resection of the colonic segment involved with primary anastomosis, subtotal colectomy with primary anastomosis, colostomy followed by resection, and resection of the colonic segment involved with end colostomy (Hartmann's procedure) requiring a second operation to reconstruct the colon. In addition, the endoscopic colonic stent can effectively decompress the obstructed colon, allow colon preparation and elective resection.Citation12
The patients can be classified according to colorectal tumors emergency score (CTES), based on 4 risk factors: colonic perforation, serum albumin, concurrent cardiovascular disease and chronic renal insufficiency. Each patient is ranked low (CTES <4), moderate (CTES 4–12) or high (CTES >12). The choice of surgical treatment can be guided by this classification. When the condition of the patient permits, it is preferable to perform primary anastomosis.Citation13
Restorative colectomy with primary anastomosis should only be regarded when the risk is favorable. In high risk patients, Hartmann's procedure is widely used especially for patients presenting with left colon cancer-associated obstruction or perforation. The procedure can be performed after complete tumor resection or as a palliative procedure.Citation5,Citation14–Citation16
Urgent subtotal or total colectomy with primary anastomosis is a safe and efficient procedure in the management of acutely obstructed neoplasm of the left colon. It allows treating in one stage the cancer and the obstruction, bearing minimal mortality, acceptable morbidity and satisfactory postoperative functional results.Citation3 Subtotal colectomy is still very useful in cases of synchronous tumors or proximal bowel damage. Simple colostomy has no role other than for palliation or use in very ill patients who would not survive any other procedure. The surgeon's experience often affects the surgical decision.Citation16
Colorectal surgeons are more likely to perform single stage operations with primary anastomosis than non-colorectal surgeons.Citation17 For appropriately selected patients, laparoscopic emergent colectomy appears safe with experienced surgeons.Citation18 Also, emergency laparoscopically-assisted right hemicolectomy for obstructing right-sided carcinoma is feasible and safe with favorable short term clinical outcomes.Citation19
The most important complication in emergency colonic surgery is anastomotic leakage. This leakage is commonly due to the impossibility of a correct preparation of the colon in emergency.Citation20
Manual decompression of colon alone is as good as colonic irrigation in the management of the left-sided colon. However, on-table antegrade colonic irrigation should be reserved for the loaded colon that may interfere with stapling, when resection margins are limited as in low anterior resection, and when the surgeon is less experienced.Citation21
In this study, complications occurred in 16 (27.1%) patients of emergency group and included intestinal leakage, bleeding, wound infection, abdominal wall sinus, incisional hernia, intestinal obstruction and recurrence. This rate of complications was significantly higher after emergency surgery than the rate after elective surgery (18.2% versus 10.2%).
Merkel et al.Citation2 found that the rates of surgical and non-surgical postoperative complications were higher in urgent surgery than in elective surgery (28.8% versus 19.8%) and also postoperative mortality was significantly higher (10.1% versus 4.0). The rates of locoregional recurrences and distant metastases were significantly higher after emergency surgery. Urgent surgery was found to be an independent prognostic factor for distant metastasis (relative risk 1.80) and cancer-related survival (relative risk 1.6).
Advanced tumor staging is a basis for poor long-term survival in emergency colorectal cancer.Citation22,Citation23 Radical operations can be fulfilled in emergency operations. Resection with free resection margins has a good effect on survival which may be similar to survival after elective surgery.Citation8,Citation10
Charbonnet et al.Citation23 found that 70% of patients who underwent emergency surgery for obstructive/perforated left-sided colonic carcinoma had a curative resection with 5-year survival rate of 40%. Delayed resection seems to be a safer procedure and provided a better oncologic outcome compared with primary resection in obstructive left-sided colorectal cancer under emergency situations.Citation24
In a study by Tarcoveanu et al.Citation25 the factors with a significant negative influence on survival included age over 70 years, emergency surgery related to cancer complications and advanced stage. Sato et al.Citation26 found that the prognosis was significantly better in patients who received adjuvant chemotherapy, male patients, age >50 years and fewer than 13 dissected lymph nodes.
In this study, there was challenge in treatment; the type of surgical procedure depended on the final intraoperative decision. Complications occurred in patients with obstruction, unprepared colon, old age >60 years and/or associated diseases. The majority of mortality after emergency surgery (62.7%) during follow up was associated with advanced tumor stage, old age >60 years and the presence of associated diseases.
In addition, the unresectable advanced tumors were the real challenge in surgical treatment. One-, two- and three-year survivals after emergency surgery were less than survivals in elective patients. The difference was not significant and this can be explained by the policy of excision of all resectable tumors in emergency conditions followed by either primary anastomosis, Hartmann's procedure or total colectomy.
5 Conclusion
There is much challenge in the diagnosis and treatment of emergency conditions of colon carcinoma. The challenge included emergency presentation of undiagnosed uninvestigated patients with difficult or impossible colon preparation, colonoscopy, tissue biopsy or tumor staging. In addition to associated diseases or old age in many patients. Mortality and morbidity rates after emergency surgery were higher than those rates after elective surgery of colon carcinoma. The selection of the surgical procedure was guided by the tumor staging, tumor location and associated diseases (co-morbidities). Total colectomy could obtain good outcome and survival when compared with other emergency procedures. Advanced unresectable tumors are the real challenge in treatment. The policy of excision of resectable tumors in emergency surgery can improve survival to approximate elective surgery.
Notes
Available online 23 January 2012
Peer review under responsibility of Alexandria University Faculty of Medicine.
References
- J.KimR.MittalV.KonvalianJ.KingM.J.StamosR.R.KumasOutcome analysis of patients undergoing colorectal resection for emergent and elective indicationsAm Surg73102007991
- S.MerkelC.MeyerT.PapadopoulosT.MeyerW.HohenbergerUrgent surgery in colon carcinomaZentralbl Chir132120071625
- C.TohmeG.ChakhtouraB.AbboudR.NounR.SarkisH.IngeaP.FarahA.GhossainSubtotal or total colectomy as surgical treatment of left-sided occlusive colon cancerJ Med Liban5642008198202
- I.A.PirletK.SlimF.KwiatkowskiF.MichotB.L.MillatEmergency preoperative stenting versus surgery for acute left-sided malignant colonic obstruction: a multicenter randomized controlled trialSurg Endosc256201118141821
- L.LepreA.MeroG.CancriniB.FrezzaL.VenturiniS.M.TiernoF.TomassiniG.CostaEmergency colonic surgery: analysis of risk factors predicting morbidity and mortalityChir Ital615–62009565571
- C.CocoA.VerboA.MannoC.MattanaM.CovinoG.PedrettiL.PetitoG.RizzoA.PicciocchiImpact of emergency surgery in the outcome of rectal and left colon carcinomaWorld J Surg2911200514581464
- A.K.SakantamisD.PissasK.PsarrasS.RafailidisK.BallasG.MarakisT.E.PavlidiDoes emergency surgery affect resectability of colorectal cancer?Acta Chir Belg10822008219225
- S.BiondoE.KreislerM.MillanJ.Marti-RaqueD.FraccalvieriT.GoldaJ.De OcaA.OsorioR.FrderaR.SalazarF.Rodriquez-MorantaX.SaniuanLong-term results of emergency surgery for colon cancer compared with elective surgeryCir Esp82220078998
- P.BuchwaldF.OlofssonE.LorincI.SykStandard protocol for assessment of cancer colon improves the quality of pathologyColorectal Dis1332011e33e36
- A.P.MikhailoyA.M.DanilovA.N.NapalkoyE.V.RybakovaI.I.GubkovAcute gastrointestinal bleedings of tumourous etiologyVestn Khir Im II Gerk165120067981
- A.SakantamisK.PapanicolaouD.PissasK.PsarrasS.RafailidisK.BallasG.MarakisT.E.PavlidisSafety of bowel resection for colorectal surgical emergency in the elderlyColorectal Dis882006657662
- F.StipaA.PigazziB.BasconeA.CimitanG.VillottiA.BurzaA.VitaleManagement of obstructive colorectal cancer with endoscopic stenting followed by single-stage surgery: open or laparoscopic resection?Surg Endosc226200814771481
- C.LorussoP.PalazzoD.MerliccoEvaluation of operative risk in emergency treatment of neoplastic left colon obstruction: personal experienceAnn Ital Chir7642005353355
- H.LippertI.GastingerU.SchmidtH.PtokP.MroczkowskiP.StubsD.GranowskiR.KubeSurgical practices for malignant left colonic obstruction in GermanyEur J Surg Oncol36120106571
- F.MeyerF.MaruschA.KochL.MeyerS.FuhrerF.KockerlingH.LippertI.GastingerEmergency operation in carcinomas of the left colon: value of Hartmann's procedureTech Coloproctol82004226229
- V.TrompetasEmergency management of malignant acute left-sided colonic obstructionAnn R Coll Surg Engl9032008181186
- R.SinghalP.HullM.BudhooManagement of left sided colorectal emergencies. Results of a postal questionnaireMinerva Chir6262007437441
- S.W.LeeT.SonadaK.TrenchevaJ.W.MilsomJ.BleierG.M.NashMinimally invasive surgery is safe and effective for urgent and emergent colectomyColorectal Dis1252010480484
- S.S.NgR.Y.YiuJ.C.LiJ.F.LeeK.L.LeungEmergency laparoscopically assisted right hemicolectomy for obstructing right-sided colon carcinomaJ Laparoendosc Adv Surg Tech A1662006350354
- M.SanoA.G.RizzoE.CingariA.IlaquaG.LemmaM.BarbusciaF.LemmaAcute neoplastic colic obstructions: therapy and postoperative complications. Our experienceG Chir3011–122009482486
- A.Z.SuleM.MisaunoA.S.OpaluwaE.OjoOne-stage treatment of left-sided large bowel emergenciesEast Afr Med J85220088084
- S.K.WongB.B.JalaludinM.J.MorganA.S.BerthelsenA.MorganA.H.GatenbyS.B.FuthamTumor pathology and long-term survival in emergency colorectal cancerDis Colon Rectum5722008223230
- P.CharbonnetP.GervazA.AndresP.l.BucherB.KonradP.MoreResults of emergency Hartmann's operation for obstructive or perforated left-sided colorectal cancerWorld J Surg Oncol6200890
- J.K.JiangY.T.LanT.C.LinW.S.ChenS.H.YangH.S.WangS.C.ChangJ.K.LinPrimary vs. delayed resection for obstructive left-sided colorectal cancer: impact on patient outcomeDis Colon Rectum5132008306311
- E.TarcoveanuD.FerariuA.NistorL.FortuP.PopaD.VintilaC.N.NeacsuS.O.GeorgescuLong-term results after surgery for colorectal adenocarcinoma, stage I–III. Problems of prognosisRev Med Chir Soc Med Nat Iasi11142007932939
- H.SatoK.MaedaK.SugiharaH.MochizukiK.KotakeT.TeramotoS.KameokaY.SaitoK.TakahashiT.HiraiM.OhueK.ShirouzuY.SakaiT.WatanabeK.HirataK.HatakeyamaHigh-risk stage II colon cancer after curative resectionJ Surg Oncol104120114552