Abstract
Background
Treatment of neglected developmental dysplasia of the hip (DDH) in children after the walking age has been a challenge to the orthopedic surgeons. It is usually surgical at this age group.
Methods
The study included 35 patients (42 hips), they had been treated by different combinations of open reduction, femoral (shortening, derotation and varus) and pelvic (Salter or Dega) osteotomy. The age at the time of the operation ranged from 18 to 96 months.
Results
At the end of follow-up (a mean of 33.5 months), the overall final clinical result was excellent in 13 (31%) patients, good in 24 (57%) patients, fair in four (9.5%) patients and poor in one (2.5%) patient satisfactory in 37 (88%) patients and unsatisfactory in five (12%) patients. The radiological end result was Class І (excellent) in 26 (62%) patients, Class II (good) in 11 (26%) patients, Class III (fair) in three (7%) patients and Class ІV (poor) in two (5%) patients. It was satisfactory in 37 (88%) patients and unsatisfactory in five (12%) patients.
Conclusion
We concluded that operative treatment of neglected DDH after the walking age is a technically demanding procedure but when performed properly by an experienced surgeon it gives satisfactory results.
1 Introduction
Developmental dysplasia of the hip (DDH) includes femoral head subluxation or dislocation and/or acetabular dysplasia.Citation1 There will always be children who reach ambulatory age with developmental dysplasia of the hip, either secondary to delayed diagnosis or failed treatment. The treatment of DDH after the walking age group is usually surgical due to the fact that the pathological changes present at this age as severe contracture of the muscles, tendons and capsule around the hip, increased shallowness of the acetabulum, excessive femoral anteversion, hypertrophoid inverted labrum, excessive pulvinar, maldirected acetabulum would make closed reduction very difficult and forcible that may lead to avascular necrosis of the femoral head or redislocation. This has led many authors to advise open reduction in this age group.Citation2 The goals of open reduction are to: (1) safely reduce the dislocated hip and to surgically recreate normal anatomy (as closely as possible) and (2) to reorient the biomechanical relationships such that the development of degenerative hip disease is delayed or prevented. To achieve these goals various pelvic osteotomies had been used. Reshaping osteotomies have had been used, such as the Pemberton and Dega osteotomies, redirectional osteotomies, including the single innominate Salter osteotomy and the triple innominate Steel osteotomy, or salvage procedures when the joint is irreducible and painful such as Chiari and shelf operations.Citation1,Citation3,Citation4

The choice of the type of pelvic osteotomy depends on careful pre-operative assessment of the severity of the acetabular dysplasia and also the age of the patient at the time of treatment.Citation5 The remodeling capacity of the acetabulum decreases steadily in the first 6 or 7 years of life so if the acetabulum contains the femoral head poorly an attempt should be made to improve the acetabular cover.Citation6 Concurrent primary femoral shortening is nearly always necessary in severe cases with a high dislocation before open reduction to allow gentle reduction and avoid pressure on the head. Varus and derotational osteotomies are less required as the acetabular dysplasia is more common.Citation6
Undiagnosed or neglected congenital hip dislocation up to adolescent or adult life may be complicated by labral tears and early osteoarthritis. The treatment at this stage can be either a salvage procedure or hip arthroplasty.Citation7
2 Aim of the work
The aim of this study was to assess the early clinical and radiographic results of surgical treatment of DDH after the walking age.
3 Patients and methods
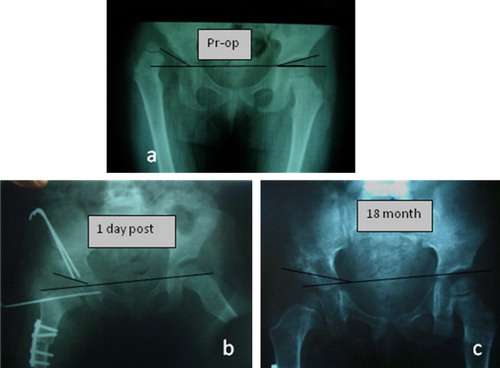
Thirty-seven patients (31 females and six males) with 42 involved hips with typical DDH were included. They presented with variable degrees of congenital maldevelopment of the acetabulum or the proximal part of the femur or both. The right hip was involved in 24 (57%), while the left in 18 (43%). The youngest age was 18 months and the oldest was 96 months with an average of 36.5 months. Eight patients had prior conservative treatment in the form of closed reduction and adductor tenotomy. According to the Tönnis classificationCitation8 (Grade 1: Capital femoral ossification center is medial to Perkins line, Grade 4: Ossification center is above superior acetabular rim. Forty-one hips had a grade 4 dislocation while one had a grade 2 dislocation. Three patients had a history of breech presentation, one of them had a history of a twin pregnancy. In 20 patients the average intra-operative blood transfusion was 116 cc, 22 patients did not receive blood. All patients in this study were subjected to clinical examination pre-operatively and at the end of follow-up. Trendelenburg test, limping, hip stability in supine position, presence or absence of deformity and the range of motion were assessed at the last patient visit. Clinical evaluation of patients was done according to a combination of modified MacKay criteria and modified Harris hip score ().Citation9,Citation10 Antero-posterior radiographs were used to measure the acetabular index (AI) and the center-edge angle (CEA) pre-operatively, post-operatively and at the end of follow-up. Changes in the femoral head as regards sphericity and the radiodensity were also looked at. Values of the acetabular index greater than 30° were considered abnormal and indicative of impending dislocation. All patients in this study had an acetabular index above 30 degrees which were considered abnormal. The average acetabular index pre-operatively was 44 ± 2.5° (range, 38°–49°). All patients in this study had negative CEA pre-operatively, except one patient whose CE angle was 10° pre-operatively. Radiological evaluation at the end of follow-up was done according to the modified Severin radiographic criteria ().Citation9
Table 1 Modified MacKay criteria and modified Harris hip score.
Table 2 Modified Severin radiographic criteria.
All patients in this study were subjected to one-stage operative treatment in the form of: open reduction, pelvic osteotomy (Salter or Dega) and/or femoral derotation and shortening followed by a period of immobilization in a hip spica cast for about 2 months (). The plan of treatment in this work has been based on the pre-operative clinical and imaging findings, together with intra-operative findings.
Table 3 Methods of treatment.
4 Surgical techniques
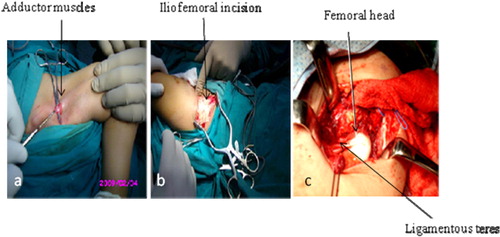
All operations were done under general anesthesia. Adductor tenotomy was done as a first step in 35 patients. Open reduction was done through a curved antero-lateral incision starting at the middle of the iliac crest 1 cm below it and extended anterior, inferior and medially up to a point where the anterior superior iliac spine becomes centered midway in the incision, it was done in all patients in this study () except 2 where the femoral head was reduced without opening the hip, under image guidance but femoral shortening and varus derotation osteotomy as well as Salter osteotomy were added to achieve stability.
Femoral osteotomy was done through a separate lateral femoral incision and fixed with a small fragment dynamic compression plate in 40 patients (). It was in the form of shortening, varus and derotation.

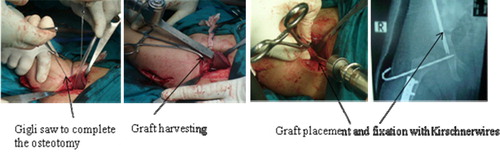
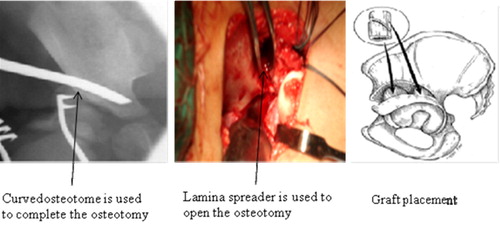
Pelvic osteotomy (Salter or Dega) was done through the anterior incision of open reduction ( and ). Salter osteotomy was done in 34 hips with mild dysplasis (AI < 45°) while Dega osteotomy was done in eight hips with severe dysplasia (AI > 45°). Both were done through the anterior incision of open reduction. Salter osteotomy was completed by a gigli saw and the graft was taken from the iliac crest. Dega osteotomy was completed by a curved osteotome and the graft was taken from femoral shortening osteotomy. Capsuloraphy was done in all cases with open reduction.
5 Method of statistical analysis
Statistical analysis was done using the statistical program for social sciences (SPSS)-version 9.0. T-test was used to analyze the relations between the obtained results and the different variables. Five percent level of significance was chosen.
6 Results
The patients were followed both clinically and radiologically for mean duration of 33.5 months (range, 12–120 months). At the end of follow-up, final clinical and radiological results were evaluated ( and ). The overall final clinical results were excellent in 13 patients (31%), good in 24 (57%), fair in 4 (9.5%) and poor in one patient (2.5%), satisfactory (excellent and good) in 37 patients (88%) and unsatisfactory (fair and poor) in five patients (12%). The radiological end result was Class I (excellent) in 26 patients (62%), Class II (good) in 11 (26%), Class III (fair) in three (7%) and Class ІV (poor) in two patients (5%). The results were satisfactory in 37 (88%) patients and unsatisfactory in five (12%) patients. No patient had Severin Class V or VІ.
Table 4 The overall final clinical result.
Table 5 The final radiological result.
6.1 Relation between the radiographic parameters and the final outcome variables
Acetabular index (AI) improved in all hips at final evaluation. The mean pre-operative AI was 44 ± 2.5°. At the end of follow-up it was reduced to an average of 23 ± 3° (range, 20°–30°) and there was statistically significant difference between the pre-operative AI and that at the final evaluation (t = 3.13, p = 0.00). Center edge angle (CEA) improved in all patients at the end of follow-up except in two patients (10°, 15°) where the femoral head was subluxed. CEA pre-operatively was negative in all patients except one (10°). The average CEA post-operatively was 31 ± 9° (range, 10–50) and there was statistically significant difference between pre-operative CEA and that at the final evaluation (t = 2.18, p = 0.00). Neither the pre-operative nor the post-operative AI had a statistically significant effect on the final clinical outcome (t = 3.690, p = 0.800 and t = 4.995, p = 0.603, respectively) while the final clinical outcome was significantly affected by CEA at the end of follow-up (t = 4.52, p = 0.001).
6.2 Relation between the clinical parameters and the final outcome variables
The mean age had no statistically significant effect on the final outcome (t = 1.398, p = 0.08). When the hips were divided into two groups (less than 36 months old and 36 months or more) there was still no statistically significant difference between the two groups (t = 0.079, p = 0.626). The final outcome also was not affected by sex (t = 1.819, p = 0.906), side affected (t = 0.621, p = 0.986) and whether the patient had been subjected to previous conservative treatment or not (t = 0.930, p = 0.583). Furthermore, the overall final result was not significantly affected by the amount of shortening (t = 7.330, p = 0.108). The mean derotation was 20.4 ± 5°. The overall final result was not significantly affected by the degree of derotation (t = 4.930, p = 0.935). The average duration of surgery was 2.2 h (range, 1.5 –2.5). The overall final results were not significantly affected by the duration of surgery (t = 0.643, p = 0.421).
7 Complications
Four patients had complications in this study, one had supracondylar fracture of the femur on the operated side during removal of the cast two and half month after the operation, This fracture was treated by above knee plaster cast, The final clinical outcome in this patients was fair (score: 80) due to moderate limitation of hip movement and limping, the final radiological outcome was graded as Severin Class II due to abnormalities in the shape of the head and neck of the femur (AVN) and was classified as grade 4 () according to Kalamchi and McEwen classificationCitation11 (grade 1 reflects changes confined to the ossific nucleus, grade 4 indicates total physeal and head injury). Two patients had a subluxed hip (), both had unsatisfactory results, one had a fair final clinical outcome (score: 80) and the other had poor final clinical outcome (score: 60) and both had a Severin Class ІV. One patient had stiffness of the hip that probably was due to prolonged immobilization in the cast. The clinical score was fair (80) although radiographic Severin Class I.

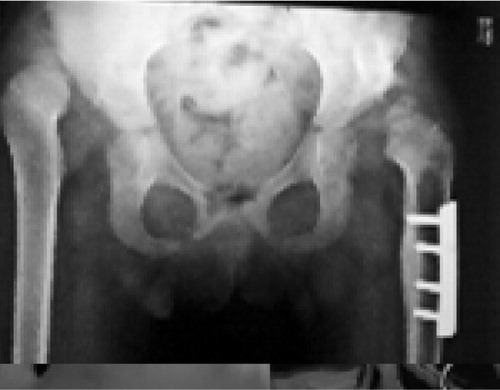
8 Case presentation ( and )
9 Discussion
There always will be children who reach ambulatory age with developmental dysplasia of the hip, either secondary to delayed diagnosis or failed treatment. Once identified, treatment of developmental dysplasia of the hip in this age group is based largely on the experience of the surgeon. Although treatment varies from closed reduction to open reduction with combined femoral and pelvic osteotomies, the goals are largely to obtain a concentric reduction without recurrence of subluxation or dislocation and without stiffness or avascular necrosis. Despite concerns that open reduction leads to joint stiffness and increased incidence of avascular necrosis, the merits of open reduction in this age group are clear. It provides visual confirmation of the adequacy of reduction while generally exposing the femoral head to less trauma. In addition, open reduction gives the surgeon the opportunity to assess the amount of acetabular dysplasia.Citation12
In this age group, Zionts and MacEwenCitation13 found that closed reduction was associated with a high rate of avascular necrosis (23.7%) and a high incidence of secondary procedures for recurrent subluxation or persistent acetabular dysplasia. They found that nearly 66% of their patients treated with traction, adductor tenotomy, and closed reduction under general anesthesia required secondary surgical procedures. Similarly, Mardem-BeyandMacEwenCitation14 found that 66% of children of walking age with developmental dysplasia of the hip who had undergone closed reduction required additional surgery, compared with 33% of such patients treated with open reduction.
Several types of pelvic osteotomies to stabilize the reduced hip in older children have been described. In this study we used Salter osteotomy for cases with mild acetabular dysplasia and Dega osteotomy for cases with severe acetabular dysplasia. Galpin et al.Citation15 cautioned against posterior instability with Salter osteotomy when it is combined with derotation femoral osteotomy. In this study there was no resubluxation associated with Salter osteotomy.
Excessive femoral neck anteversion is usually present in cases of DDH but it is clinically not apparent in these patients when the hip is in a subluxed or dislocated position, but it becomes so when the hip is reduced at open reduction where the head is usually reduced and becomes stable after internally rotating the hip. This was found to be true in this study, as 40 of 42 hips included were found to need a femoral derotational osteotomy after reducing the femoral head in the acetabulum under vision. The average derotation angle was found to be 20°.
Schoenecker and StreckerCitation16 found that femoral diaphyseal shortening to be superior to traction as an aid in operative reduction of developmental dysplasia of the hip with a decreased rate of avascular necrosis and a decreased rate of redislocation. TönnisCitation8 concluded that sufficient shortening and dissection of the iliopsoas tendon and rectus femoris tendon are of great importance in preventing increased pressure and ischemic necrosis. In this study, we found that femoral shortening was needed in most of cases (95%).
A few investigators have evaluated the long term functional and radiographic outcome of a one-stage operation for the treatment of DDH in children after the walking age. Most of these studies used different combinations of surgical treatment without standardizing a fixed surgical protocol for treatment as well as differences in patient selection, length of follow-up, and classification systems. This made it difficult to compare their results with ours. Galpin et al. in a study of 33 hips in 25 patients, 2 years of age or older treated by one-stage surgical method, they reported satisfactory results clinically in 85% of their patients and radiographically in 75%.Citation15 Ryan et al.Citation17 reported their results of operative treatment of cases of DDH as follows: seven hips had excellent results; 11 good results, four fair results and three poor results. Eleven hips had evidence of osteonecrosis. They suggested that a one-stage operative procedure consisting of open reduction, femoral shortening and pelvic osteotomy (if necessary) for previously untreated DDH in children who are three to ten years old can result in remodeling of the acetabulum and a functional hip. Nakamura et al.Citation18 reported: excellent results in five joints, good in three and fair in three. In this study, 37 hips (88%) had good or excellent clinical and radiological results at the final follow-up.
The upper age limit for open reduction and the remaining potential for acetabular remodeling are controversial. Ok et al.Citation19 concluded that, if there is a high likelihood of achieving a functionally good hip joint with biological remodeling, an open reduction is a reasonable strategy for an untreated dislocation in patients, even those older than 8 years of age. Although many authors suggest an upper age limit of 8 years for treatment, they found that joint remodeling continued even after this age after a concentric reduction of the developmentally dislocated hip. In this study we found no relationship between the age at the time of treatment and the final outcome.
In the current study two patients (4.5%) had resubluxation of the hip. Rudolf et al.Citation20 reported 3 of 54 hips with redislocation, GrillCitation21 reported 12 of 50 hips with redislocation and resubluxation. Ruszkowski and PucherCitation22 reported one of 33 hips in 26 children with redislocation. In this study one patient (2.3%) had a distal femoral fracture during the early period of mobilization after cast removal. GrillCitation21 reported 5 of 50 hips with distal femoral fracture. One patient (2.3%) in this study developed avascular necrosis of the femoral head at the time of final examination and classified as grade 4 according to Kalamchi and McEwen.Citation11 Zionts and MacEwenCitation13 identified major AVN in approximately 5% of their patients. Ryan et al.Citation17 reported 11 out of 25 hips (44%) with avascular necrosis. There is a wide variation in the incidence of AVN between different studies that may be due to different classification systems used in different periods of follow-up or different methods of both conservative and surgical treatments.
10 Conclusion
One-stage surgical treatment of DDH after the walking age is an excellent method. For successful surgery, open reduction with removal of all soft tissues impairing reduction as well as optimal positioning of the head into the acetabulum together with a proper capsuloraphy should be done. Correction of acetabular dysplasia by Salter or Dega osteotomies is very important to achieve a stable reduction of the hip. Femoral shortening should be performed in cases where tight reduction is achieved to avoid pressure on the femoral head and development of AVN. Femoral derotational osteotomy is usually required with femoral shortening as most of the cases have excessive femoral neck anteversion while varus osteotomy is not necessary in every case.
Conflict of interest
The authors have no conflict of interest to declare.
Notes
Available online 25 February 2012
Peer review under responsibility of Alexandria University Faculty of Medicine.
References
- Beaty H. Congenital and developmental dysplasia of the hip. In: Canale T, editor. Cambell's operative orthopaedics. volume 2.9th ed. St Louis, Boston, Chicago, London, Toronto, Baltimore: CV Mosby Company; 1998. p. 1079–117.
- Tachdjian MO. Deformities of the lower limb. In: Tachdjian MO, editor, Pediatric orthopaedic. volume 1.1st ed. Philadelphia, London, Toronto: W.B. Sunders Company; 1972. p. 129–76.
- E.LiptonJ.RichardA new modified technique of triple osteotomy of the innominate bone for acetabular dysplasiaClin Orthop43420057885
- L.StuartJ.ScottR.DennisDevelopmental hipdysplasia and dislocation (part II)J Bone Joint Surg Am85-A200320242035
- Staheli LT. Developmental hip dysplasia. In: Staheli LT, editor, Practice of pediatric orthopaedics. chapter 7.2nd ed. Philadelphia, Baltimore, New York, London, Hong Kong, Sydney: Lippincott Williams and Wilkins; 2006. p. 166–81.
- Benson MK, Macnicole MF. Developmental dysplasia of the hip. In: Benson MK, Macnicole MF, Fixsen JA, editors, Children's orthopaedics and fractures. volume II.2nd ed. London, Edinburgh, New York, Philadelphia, Toronto: Churchill Livingstone; 2002. p. 359–381.
- W.H.HarrisR.B.BourneI.OhIntra-articular acetabular labrum: a possible etiological factor in certain cases of osteoarthritis of the hipJ Bone Joint Surg Am61-A41979510514
- D.TönnisSurgical treatment of congenital dislocation of the hipClin Orthop25819903340
- C.E.BadgleyCorrelation of clinical and anatomical facts leading to a conception of tile etiology of congenital hip dysplasiasJ Bone Joint Surg Am25-A1943503
- C.E.BadgleyEtiology of congenital dislocation of the hipJ Bone Joint Surg Am31-A1949341
- A.KalamchiG.D.MacEwenAvascular necrosis following treatment of congenital dislocation of the hipJ Bone Joint Surg Am621980876888
- R.K.AshlyL.J.LarsenP.M.JamesReduction of dislocation of the hip in older childrenJ Bone Joint Surg Am54-A1972545550
- L.E.ZiontsG.D.MacEwenTreatment of congenital dislocation of the hip in children between the ages of one and three yearsJ Bone Joint Surg Am68-A1986829
- T.H.MardamG.D.MacEwenCongenital hip dislocation after walking ageJ Pediatr Orthop21982478486
- R.D.GalpinJ.W.RoadD.R.WengerJ.A.HerringJ.G.BirchOne stage treatment of congenital of the hip in older children, including femoral shorteningJ Bone Joint Surg Am7I-A1989734741
- P.L.SchoeneckerW.B.StreckerCongenital dislocation of the hip in children: Comparison of the effects of femoral shortening and of skeletal traction in treatmentJ Bone Joint Surg Am66-A198421
- M.G.RyanL.O.JohnsonD.S.QuanbeckB.MinkowitzOne-stage treatment of congenital dislocation of the hip in children three to ten years old: functional and radiographic resultsJ Bone Joint Surg Am80-A1998336344
- S.NakamuraS.NinomiyaY.TakatoriS.MorimotoT.UmeyamaLong-term outcome of rotational acetabular osteotomy: 145 hips followed for 10–23 yearsActa Orthop Scand691998259265
- I.Y.OkS.J.KimJ.H.OkOperative treatment of developmental hip dysplasia in children aged over 8 yearsJ Pediatr Orthop16-B2007256261
- G.RudolfR.ChristofP.GertM.HansK.GabrieleF.GrillTreatment options for developmental dislocation of the hip after walking ageJ Pediatr Orthop142005139150
- F.GrillTreatment of hip dislocation after walking ageArch Orthop Trauma Surg1021984148153
- K.RuszkowskiA.PucherSimultaneous open reduction and Degatransiliac osteotomy for developmental dislocation of the hip in children under 24 months of ageJ Pediatr Orthop2552005695701