Abstract
Background
Airway management is a major responsibility for anesthetist. This study was carried out to evaluate and compare the efficacy of Airtraq (AL) and Macintosh Laryngoscopes (ML) in intubating patients with cervical spine immobilization using manual inline axial stabilization technique (MIAS).
Methods
This randomized controlled study was carried out in Alexandria Main University Hospital on 40 adult ASA I and II patients after written informed consent and approval of the ethical committee, randomly categorized into two equal groups. All patients were subjected to same anesthetic protocol. Group I patients were intubated using AL and group II patients were intubated using ML. Hemodynamic measurements and oxygen saturation were recorded. Intubation criteria for both groups including (duration of intubation procedure, number of attempts, number of optimization maneuvers, Cormack and Lehane grade at laryngoscopy, Intubation Difficulty Scale score (IDS), rate of successful placement of endotracheal tube, neck mobility during laryngoscopy and intubation complications were recorded. Data statistically analyzed using SPSSR software using (t and χ2 tests) and P < 0.05 considered significant.
Results
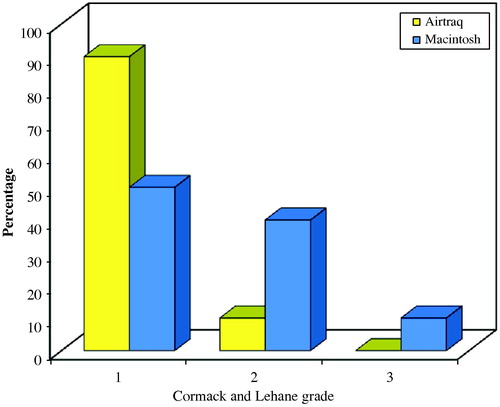
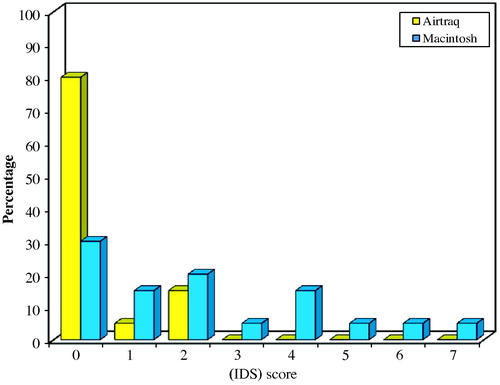
There was statistically significant increase in both heart rate and mean arterial blood pressure values following intubation in ML group than AL, oxygen saturation showed no significant difference between the two groups. Duration of intubation was statistically significant longer in ML group and needed more optimization maneuvers than the AL group, while for the number of intubation attempts; there was no statistically significant difference between the two groups. Both the Cormack and Lehane grading and IDS score values have shown statistically significant higher values in ML group.
Conclusion
The Airtraq Laryngoscope offers a new approach for the management of difficult airway like patients with potential cervical spine injury, it is fast, easy to use, gets an easy view of the larynx without moving the cervical spines or causing hemodynamic stimulation.
1 Introduction
Airway management is a major responsibility for the anesthetist. Difficulties with tracheal intubation significantly contribute to the morbidity and mortality associated with anesthesia.Citation1 The anesthetist should consider strategies to anticipate and manage patients with difficult airways. These include identifying the potential problems, considering different options, and selecting an appropriate plan for the individual patient Citation2.
Endotracheal intubation is frequently required for trauma patients as part of the resuscitative effort or for patients with unstable cervical spine requiring surgery. The potential for cervical spine injury makes airway management more complex in the trauma patient. Cervical spine motion during intubation deserves particular attention in cases with cervical pathology. All types of devices and maneuvers associated with airway management are associated with some degree of cervical spine motion Citation3–Citation6.
Airtraq Laryngoscope (AL) is a new intubation device that has been developed to facilitate tracheal intubation in patients with normal or difficult airways. As a result of the exaggerated curvature of the blade and an internal arrangement of optical components, a high-quality view of the glottis and surrounding structures is provided without alignment of the oral, pharyngeal and tracheal axesCitation7,Citation8. The blade of the Airtraq consists of two side by side channels, one channel acts as a conduit through which a tracheal tube (ETT) can be passed, while the other channel contains a series of lenses, prisms and mirrors that transfers the image from the illuminated tip to a proximal viewfinder, giving a high quality wide-angle view of the glottis, surrounding structures and the tip of the tracheal tube Citation7.
Despite recent developments in airway device technologies, the Macintosh Laryngoscope (ML) is still considered the golden standard for endotracheal intubation since it was first used in 1943 until this day Citation9,Citation10. Conventional intubation with ML requires a direct view of the structures of the larynx, the line of vision needed for this demands extension of the head and flexion of the cervical spine to align the oral, pharyngeal and tracheal axes. The movements of the cervical spine involved in this procedure are highly complex from the functional–anatomical point, however, using of MIAS may provide some safety, yet it will add more difficulty in visualizing the larynx using conventional laryngoscopes Citation11.
This study was carried out to evaluate and compare the efficacy of both the Airtraq and the Macintosh laryngoscopes in intubating patients with cervical spine immobilization while applying the Manual inline axial stabilization technique (MIAS) as regards the ease of intubation during neck immobilization.
2 Methods
This randomized controlled study was carried out in Alexandria Main University Hospital on 40 adult ASA I and II patients after taking a written informed consent from each patient and approval of the ethical committee. Patients were randomly categorized into two equal groups (twenty each). Patients with mallampati III and IV, thyromental distance less than 6 cm, risk of gastric aspiration and with cervical injury or instability were excluded from the study. All patients were subjected to the same anesthetic protocol; using intravenous (IV) midazolam 0.04–0.05 μg/kg as premedication, pre oxygenation for at least 3 min, General Anesthesia(GA) using (IV fentanyl 1–1.5 μg/kg, IV propofol 2–3 mg/kg and IV atracurium 0.5 mg/kg). All patients were monitored by using Hewlett Packard Viridian 24 multichannel monitor.
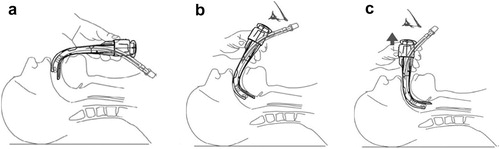
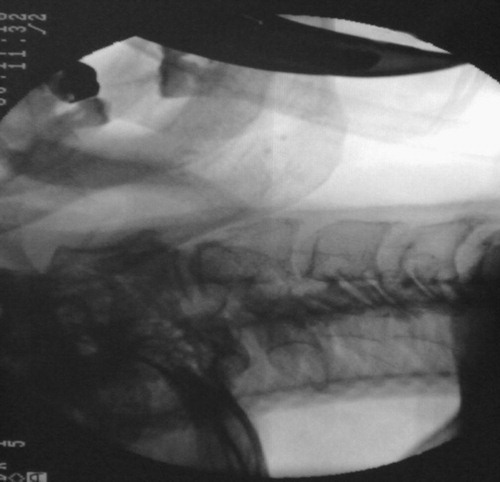
After the onset of neuromuscular blockade, the neck was immobilized using MIAS, holding the sides of the neck and the mastoid processes, and thus preventing flexion/extension or rotational movement of the head and the neck Citation3. C-arm was used to do imaging for each patient, one image taken before intubation after applying MIAS, and the other one taken during intubation with the MIAS applied. The two images were then compared to document if any movement had occurred during the intubation procedure by the two devices. C-spine motion was examined at four areas: the occiput-C1 junction, C1–C2 junction, C2–C5 motion segment, and C5-thoracic motion segment.Citation12 Group I patients were intubated using AL, to use the Airtraq device, the blade must be inserted into the mouth in the midline, over the centre of the tongue, the tip positioned in the vallecula, look through the eyepiece until you see the epiglottis and the vocal cords then advance the ETT until seeing it passing through the vocal cords. After verifying ETT placement, hold it and slid the Airtraq backward and make sure that ETT has not moved Citation13. () Group II patients were intubated using ML, the blade of ML was introduced to the right of the tongue, advanced into the hypopharynx, pushing the tongue to the left, and then the laryngoscope was lifted upward and forward, without changing the angle of the blade, to expose the vocal cords Citation10.
Hemodynamic measurements including (heart rate and mean arterial blood pressure) and oxygen saturation were recorded before induction of GA, before intubation, just after intubation and at 2 min interval for the first 5 min after intubation. Intubation criteria for both groups including (duration of intubation procedure which is the time taken from insertion of the blade of the laryngoscope between the teeth until the endotracheal tube (ETT) is passed through the vocal cords and confirmed by auscultation the chest for bilateral equal air entry, number of intubation attempts, number of optimization maneuvers required and rate of successful placement of the ETT in the trachea) were recorded. The Cormack and Lehane grade at laryngoscopy and intubation difficulty scale score IDS were recorded Citation14,Citation15 ( and ). Complications during ETT (lip or tongue bruising and teeth clicking) were also recorded.
Table 1 The Cormack and Lehane grade at laryngoscopyCitation13.
Table 2 The Intubation Difficulty Scale (IDS) score: Citation14 The IDS score is the sum of the following seven variables.
3 Statistical analysis
Data were analyzed by using SPSSR software (Statistical package for social science for personal computers) using (t and χ2 tests), data were expressed as mean ± SD and P < 0.05 considered significant.
4 Results
There were no statistically significant differences between the two studied groups as regards demographic data (age, sex, weight and ASA physical status) (). Hemodynamic changes were analyzed in the present study; there was statistically significant increase in both heart rate and mean arterial blood pressure values at all periods following intubation in group II (ML group), while group I (AL group) showed no statistical significant changes. ( and ) As regards the percentage of oxygen saturation, there was no significant difference between the two groups. ().
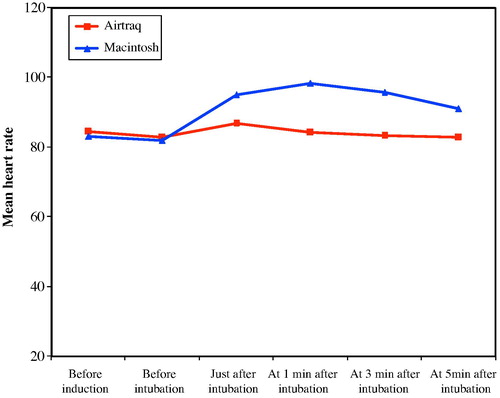
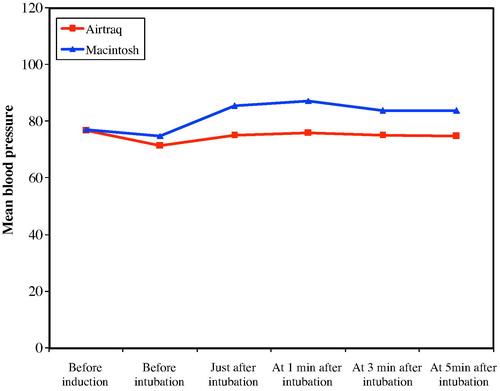
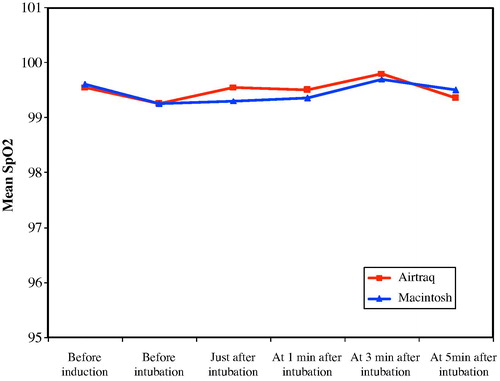
Table 3 Demographic data.
Duration of the intubation procedure was significantly longer in ML group than AL group (34.3 ± 12.27 s in AL group versus 48.75 ± 21.57 s in ML group), while for the number of intubation attempts, although it was less in the AL group, yet there was no statistically significant difference between the two groups. Both devices needed some optimization maneuvers, especially in the ML group which had statistically significant more optimization maneuvers than AL group (0.10 ± 0.031 in AL group versus 0.85 ± 0.081 in ML group). ().
Table 4 Intubation criteria.
Both the Cormack and Lehane grading at laryngoscopy and IDS score values have shown statistically significant difference between both groups, where the ML group had statistically significant higher values indicating increased difficulty at intubation (P = 0.021 and 0.022 respectively). ( and ) There were no significant statistical differences between the two groups as regards rate of successful ETT placement (). There were no statistical significant differences between the two groups as regards the complications (lip or tongue bruising and teeth clicking) although the ML group showed some complications while the AL group did not show any of them ().
Comparing C-spine motion in patients underwent AL and direct ML for intubation, in both groups, cervical spine immobility was achieved in all patients successfully by applying MIAS with no statistical significant differences (), ( and ).

5 Discussion
Airway management remains a vital primary skill for anesthetist through history, many devices and instruments have been used to ease the burden of this crucial technique. Despite advances in medical technology, emergent orotracheal intubation continues to challenge even the most experienced anesthetist Citation16.
The present study was carried out to evaluate and compare the efficacy of both the AL and ML laryngoscopes in intubating patients with cervical spine immobilization using MIAS, by comparing each group alone, in AL group both heart rate and mean arterial blood pressure did not show statistically significant changes during the intubation procedure while in ML group, there was statistically significant increase in heart rate and mean arterial blood pressure at all periods following intubation when compared to the preinduction values. On comparing the two groups together; the AL resulted in significantly less stimulation of heart rate and blood pressure after tracheal intubation in comparison with the ML. This finding could be attributed to the fact that the AL provides a view of the glottis without a need to align the oral, pharyngeal and tracheal axes, and therefore requires less force to be applied during laryngoscopy, while when using the ML during application of MIAS, which did not allow alignment of the three airway axes, more lifting force and more manipulations were exerted to get a glottic view.
Similar results were documented by Maharaj et al.Citation17 when compared AL with the ML for intubating patients with cervical spine immobilization while performing MIAS. AL group showed less hemodynamic stimulation and pressor effects than the ML group. These findings were the result of the absence of head/neck manipulations as well as the shorter duration of the intubation trials by the AL. The same results were reported by Costello et al. Citation18 in their study to evaluate the AL and ML in patients at increased risk for difficult tracheal intubation.
In the present study regarding the oxygen saturation during the intubation procedure, in both groups it was preserved above 96% and no desaturation was documented as the intubation attempts were interrupted by mask ventilation. When considering the duration of the intubation procedure, duration of intubation attempts were significantly shorter with the AL group when compared to the ML group. This can be explained by the fewer maneuvers required in the AL group to improve the glottis exposure compared to the ML group where there was more difficulty to obtain a view of the glottis while performing MIAS. Similar results were documented by Maharaj et al., Citation17 AL required statically significant shorter time for the intubation procedure with mean value 13.2 ± 5.4 s versus 20.3 ± 12.2 s for the ML. On the other hand, Chalkeidis et al. Citation19 in their comparative study between the AL and ML for routine airway management have disagreed with the previous results. The results of their study showed that intubation by experienced anesthetist was performed more quickly with the traditional ML than with the AL. However, the difference between the two groups was 5.9 s only; beside they were working on normal airway.
As regards the number of intubation attempts in the present study, there was no statistically significant difference between the two devices as regard the number of intubation trials. In agreement with this study, Maharaj et al. Citation17 have reported nearly the same results in their study; there was no statistically significant difference between the AL group and the ML group as regards the number of intubation trials. In contrast to this study, Chalkeidis et al. Citation19 in their comparative study stated that, three patients were unsuccessfully intubated with the AL. Two of these patients, the laryngoscope visual field were blurred; the other patient was initially successfully intubated but was accidentally extubated during the withdrawal of the Airtraq from the mouth. This may be explained by unfamiliarity of the operator with the new device and how to prepare it before use.
As regards optimization maneuvers required, both devices needed some optimization maneuvers during insertion and placement of the endotracheal tube, AL had a statistically significant less optimization maneuvers than ML and offered easier intubating conditions. Similar results were documented by Laffey and Black Citation20 in a similar study showing that all the patients intubated by the use of AL did not require any optimization maneuvers, in comparison to ML group where 25% of the patients required one, 15% of the patients required two and only 60% of the patients did not require any optimization maneuvers. Although Chalkeidis et al. Citation19 in their comparative study stated that the AL is easier to use yet it does not have any significant advantages compared with the ML for routine airway management.
In the present study, Cormack and Lehane grading at laryngoscopy showed that, 90% of the patients intubated with the AL had a grade I Cormack and Lehane glottic view and 10% had grade 2, compared with 50% of the patients in the ML group had grade 1, 35% with grade 2, and 15% with grade 3, which reflects that the Airtraq can be useful in case of difficult airway. Maharaj et al. Citation17 in their similar study found nearly the same results, where nineteen patients out of the twenty intubated by the AL were grade 1 and one patient was grade 2, while in the ML group only six patients had grade 1, seven patients grade 2 and the other seven had grade 3.
On discussing the results of the present study as regards the ID score, mean ID score was reduced in the AL group with none of the patients showing > score 2, in comparison to the ML group which showed increased ID scores. Although all patients in our study were chosen to be of normal airway, yet applying the MIAS technique have made the intubation procedure a difficult intubation one. Laffey and Black Citation20 in their study found that all patients in the ML group had an IDS score of ⩾ 1, compared to five in the AL group. In the ML group, 19 patients had an IDS score of 4 or greater, indicating at least a moderate degree of intubation difficulty, compared to none in the AL group.
As for the rate of successful placement of the ETT, all patients were successfully intubated by both the AL and the ML, although some required more than one attempt of intubation in both groups. This is attributed to the easiness of use of the Airtraq and its quick learning curve. The same results were conducted by Laffey and Black Citation20 where all patients in AL group were successfully intubated on the first attempt while in ML group, tracheal intubation was unsuccessful in four patients, and those patients were successfully intubated on the first attempt with the Airtraq. Maharaj et al. Citation17 also had nearly the same results as regards the overall success rate of intubation in patients with cervical spine immobilization, with 100% of the patients intubated in the AL group and 95% in the ML group. Turkstra et al. Citation12, compared AL and ML use in intubating patients with cervical spine immobilization using MIAS, C-spine motion was 53%, 95%, and 60% less during laryngoscopy with AL compared to the ML at the occiput-C1, C2–C5, and C5-thoracic motion segments, respectively (all P ⩽ 0.01). Similar to the present study they concluded, use of the Airtraq Laryngoscope may be useful to limit movement without an increase in the duration of intubation Citation12.
As regards the complications related to this study, which were presented in the form of lip bruising, tongue bruising, and teeth clicking, there was no statistical significant difference between the two groups. Yet ML group had 15% of the patients that showed such complications while the AL group showed none of them. The same results were conducted by Laffey and Black Citation20 who reported that the Airtraq significantly reduced the incidence of minor complications as mucosal bleeding or lip bruising.
6 Conclusion
The Airtraq Laryngoscope offers a new approach for the management of the normal and difficult airway like patients with potential cervical spine injury, it is fast, easy to use, gets an easy view of the larynx without moving the cervical spines or causing hemodynamic stimulation.
Notes
Available online 4 April 2012
Peer review under responsibility of Alexandria University Faculty of Medicine.
References
- G.N.PetersonK.B.DominoR.A.CaplanManagement of the difficult airway: a closed claim analysisAnesthesiology10320053339
- N.R.ConnellyK.GhandourS.DunnManagement of unexpected difficult airway at a teaching institution over a 7-year periodJ Clin Anaesth182006198204
- S.KiharaS.WatanabeJ.BrimacombeSegmental cervical spine movement with the intubating laryngeal mask during manual in-line stabilization in patients with cervical pathology undergoing cervical spine surgeryAnaesth Analg912000195200
- T.V.MurthyP.BhatiaR.L.GognaAirway management: uncleared cervical spine InjuryIJNT2200599101
- W.T.HuangY.T.ChungClinical comparisons between GlideScope video laryngoscope and Trachlight in simulated cervical spine instabilityJ Clin Anaesth192007110114
- J.J.HendersonM.T.PopatI.P.LattoA.C.PearceDifficult airway society guidelines for management of the unanticipated difficult intubationAnaesthesia592004675694
- C.H.MaharajJ.F.CostelloB.D.HigginsB.H.HarteJ.G.LaffeyRetention of tracheal intubation skills by novice personnel: a comparison of the Airtraq and Macintosh laryngoscopesAnaesthesia632007272278
- G.DhonneurS.NokoR.AmathieuL.El HousseiniC.PonceletL.TualTracheal intubation using the Airtraq in morbid obese patient undergoing emergency cesarean deliveryAnesthesiology1062007629630
- R.R.MarksR.HancockP.ChartersAn analysis of laryngoscope blade shape and design: new criteria for laryngoscope evaluationCan J Anaesth401993262270
- T.M.CookJ.P.TuckeyA comparison between the Macintosh and the McCoy laryngoscope bladesAnaesthesia511996977980
- J.PaulD.O.AllegrettiLarygoscope blade reviewAm J Emerg Med26200889
- T.P.TurkstraM.EngDavid M.PelzPhilip M.JonesCervical spine motion: a fluoroscopic comparison of the Airtraq laryngoscope versus the Macintosh laryngoscopeAnesthesiology1111200997101
- C.H.MaharajM.Ni ChonghaileB.HigginsTracheal intubation by inexperienced medical residents using the Airtraq and Macintosh laryngoscopesAm J Emerg Med62008241247
- R.S.CormackJ.LehaneDifficult tracheal intubation in obstetricsAnaesthesia39198411051111
- F.AdnetS.W.BorronS.X.RacineJ.L.ClemessyJ.L.FournierP.PlaisanceThe intubation difficulty score (IDS): proposal and evaluation of a new score characterizing the complexity of endotracheal intubationAnesthesiology87199712901297
- H.ChrisenB.MaharajB.ElmaH.BrianM.B.HarteG.JohnEndotracheal intubation in patients with cervical spine immobilizationAnesthesiology10720075359
- C.H.MaharajB.HigginsB.H.HarteJ.G.LaffeyEvaluation of ease of intubation with the Airtraq or Macintosh laryngoscope by anaesthetists in easy and simulated difficult laryngoscopy: a manikin studyAnaesthesia612006469477
- J.F.CostelloC.H.MaharajB.H.HarteEvaluation of the Airtraq and Macintosh laryngoscopes in patients at increased risk for difficult tracheal intubationAnaesthesia632008182188
- ChalkeidisK.GeorgiosK.ApostolosA comparison between the Airtraq and Macintosh laryngoscopes for routine airway management by experienced anesthesiologists: a randomized clinical trialActa Anaesthesiol Taiwan48120101520
- J.G.LaffeyJ.J.BlackEmergency use of the Airtaq laryngoscope in traumatic asphyxia: case reportEmerg Med J242007509511