Abstract
Background
Colonoscopy is a routine procedure in patients who present with bowel symptoms. Polyps can be identified and removed during colonoscopy. A colonoscopy quality-assurance program (CQAP) was instituted in 2003.
Aim
The aim of the study was to determine the effect of instituting a CQAP on the quality of endoscopic polypectomy (EP) in our patients.
Patients and methods
An Initial assessment of EP practice in 2003 showed that four patients had polyps. Cecal intubation had been achieved in only two patients and a complete polyp description (CPD) had not been documented. Polypectomy was performed in two patients but the completeness of removal and retrieval of the polyps had not been assessed and histology had not been recorded. A quality improvement process was therefore instituted. This required full colonoscopy to the cecum, CPD and polypectomy to be performed for every polyp. There should be a 90% retrieval rate of all excised polyps and follow up of all histology reports. Seventy-six patients were assessed prospectively over the period 2004–2011.
Results
Cecal intubation rates increased from 65% in years 2004–2007 to 90% in years 2008–2011 (t-proportion = 2.4 & CI = 4.7, highly significant). CPD rates increased from 35% to 100% (t-proportion = 6.5 & CI = 12.7, highly significant). EP rates increased from 59% to 100% (t-proportion = 3.5 & CI = 6.9, highly significant). Percentage of procedures in which all polyps were judged completely removed increased from 41% to 86% (t-proportion = 3.6 & CI = 7, highly significant). Polyp retrieval rates, with retrieval of ⩾90% of all excised polyps, increased from 80% to 92% (t-proportion = 0.87 & CI = 1.7, significant). Polyp histology documentation rates increased from 41% to 88% (t-proportion = 3.7 & CI = 7.3, highly significant).
Conclusion
The implementation of a quality assurance and improvement program improved the quality of EP in patients with polyp(s) detected during colonoscopy.
1 Introduction
Colonoscopy is a routine procedure in patients of all ages who present with bowel symptoms. Polyps can be identified and removed during colonoscopy. Colonoscopy is technically demanding and has the potential to cause harm if performed badly. It is highly operator-dependent and standards vary.Citation1 Although adverse events are unusual when they do arise they may be life threatening. The majority of adverse events arise during therapeutic colonoscopy.Citation2 An important benefit of colonoscopy is that polyps can be identified and removed during the procedure thereby reducing the risk of colon cancer.Citation3 Endoscopists should be able to perform polypectomy safely and effectively but should remove lesions only within their level of experience.Citation3 Histological examination of the resected specimens is the only reliable way to classify polyps and to exclude malignancy and it is therefore essential to guide further clinical management.Citation3 Adenomas, rather than polyps, are the outcome of interest because of their potential to develop into colorectal cancers.Citation4 The purpose of adenoma removal is to prevent the progression of benign lesions to bowel cancer.Citation2 Data from the national polyp study suggested that colonoscopy and polypectomy prevented 76–90% of incident cancers; however a proportion of incident cancers are probably related to missed lesions.Citation5
Bolak Eldakror Hospital is a secondary-care governmental hospital in Giza, Egypt. The gastrointestinal endoscopy unit was set up in 1999. A colonoscopy quality-assurance program (CQAP) was instituted in 2003.Citation6–Citation12 Accordingly, quality indicators developed by the American Society of Gastrointestinal Endoscopy and the British Society of Gastroenterology were implemented.Citation2,Citation13,Citation14 For easy application, quality indicators were identified for five major groups: patients, procedures, endoscopists, assistant staff and equipment. Process or outcome indicators were used to evaluate and monitor the quality of endoscopic procedures e.g. quality indicators of polypectomy. These include: Complete examination of the colon (cecal intubation), complete polyp description (location, size, number and gross morphology), routine polypectomy for all polyps identified, a retrieval rate of 90% of all excised polyps for histological analysis and full follow up of histology reports. The aim of the study was to determine the effect of instituting a CQAP on the quality of endoscopic polypectomy in patients with polyp(s) detected during colonoscopy.
2 Patients and methods
All patients having polyps detected during colonoscopy were included in the study. Patients were referred from outpatient clinics and the medical department. Children were referred from the pediatric departments in the hospital and from other hospitals. Our endoscopy unit is the only endoscopy unit in the area where colonoscopy for children is performed. Two gastroenterologists performed all cases.
Colonoscopy in children was performed under supervision of an expert in pediatric colonoscopy. Colonoscopy in adults was performed with conscious sedation (midazolam and pethidine combination) and in children with general anesthesia (propofol or ketamine). Two colonoscopes (Olympus CF-230L/I and CF-EL) were used. Polypectomy was performed with diathermy unit (Olympus PSD-20). Pure coagulation current was used in polypectomy. Removal, retrieval and collection of polyps were performed with hot snare, cold biopsy for diminutive polyps, polyp retriever and polyp trap. Pathological examination was performed by two expert pathologists.
An Initial assessment of our endoscopic polypectomy practice in 2003 showed that four patients with polyps had been detected during the year. Cecal intubation however was achieved in only two patients. A complete polyp description was not documented. Polypectomy was performed in only two patients. The completeness of removal or retrieval of each polyp was not assessed. Histology of the polyps was not recorded. A quality improvement process was therefore instituted.
The quality indicators chosen required full colonoscopy to the cecum, complete polyp description and polypectomy to be performed on every polyp. There should be a 90% retrieval rate of all excised polyps for histological analysis and follow up of histology reports was to be routinely performed in all patients in whom polyps were detected. Between 2004 and 2011 annual quality assurance reports were transmitted to an independent experienced endoscopist with a particular interest in quality assurance for comment and advice.
A total of 312 patients underwent colonoscopy over the period 2004–2011. Polyps were detected in 88 patients (28%). Twelve were excluded: six had polyps that were in close proximity to a colorectal cancer (referred to surgery), five had inflammatory polyps (three pseudopolyps with ulcerative colitis and two Bilharzial polyps) and one had a polypoid lesion (an inverted diverticulum masquerading as a polyp). Seventy-six patients therefore were assessed prospectively for the following: cecal intubation rate, complete polyp description, endoscopic polypectomy rate, complete polyp removal rate, and polyp retrieval of ⩾90% of all excised polyps. These and the histology report follow up were assessed over a period of eight years.
The data from the patients were registered, tabulated and analyzed statistically using a program of SPSS version 13. Descriptive data are presented as percentage and t-proportion test and confidence interval (CI) were performed to detect the differences between two categorical groups.
3 Results
A total of 76 patients were included in the study. Fifty-seven percent were men and 43% were women. Mean age: 22 ± 23 years, age range: 2–86 years. Forty-five patients (59%) were children (less than 12 years). The indications for colonoscopy included rectal bleeding in 52 patients (68%), diarrhea in seven (9%), post polypectomy surveillance in seven (9%), anemia in five (7%), abdominal pain in three (4%) and repeat in two (3%). Polyps were located in the left side of the colon (rectum, sigmoid and descending colon) in 51 (67%), right colon in 14 (18%) and whole colon in 11 (14%). Polyps measured <10 mm in 34 (45%), 10–20 mm in 25 (33%), >20 mm in six (8%) and the size was not documented in 11 (14%). Polyps were single in 42 (55%) and multiple in 34 (45%). Mean number: 3 ± 4, range: 1–20. The polyps were pedunculated in 36 (47%), sessile in 20 (26%), both in 17 (22%) and flat (raised) in three (4%). Cecal intubation was achieved in 64 (84%). Endoscopic polypectomy was performed in 69 (91%). All polyps were removed as a single piece. Polyps were judged completely removed in 58 (76%). Retrieval of ⩾90% of all excised polyps was successful in 62 (90%). Histology was recorded in 59 (78%) and not available in 17 (22%). Juvenile polyps were identified in 37 patients (49%), hyperplastic in 11 (14%) and adenoma in 11 (14%) of whom nine were tubular adenomas, one flat adenoma and one serrated adenoma. Perforation occurred in one patient (1.3%) and was managed surgically. No mortality was reported during the study period.
Polyps were detected in seven patients in 2004, five in 2005, three in 2006, two in 2007, three in 2008, seven in 2009, 31 in 2010 and 18 in 2011. Cecal intubation rates increased significantly from 65% in years 2004–2007 to 90% in years 2008–2011 (t-proportion = 2.4 & CI = 4.7, highly significant) ( and ). Complete polyp description rates increased significantly from 35% in years 2004–2007 to 100% in years 2008–2011 (t-proportion = 6.5 & CI = 12.7, highly significant) ( and ). Endoscopic polypectomy rates increased significantly from 59% in years 2004–2007 to 100% in years 2008–2011 (t-proportion = 3.5 & CI = 6.9, highly significant) ( and ). Percentage of procedures in which polyps were judged completely removed increased significantly from 41% in years 2004–2007 to 86% in years 2008–2011 (t-proportion = 3.6 & CI = 7, highly significant) ( and ). Polyp retrieval rates, with retrieval of ⩾90% of all excised polyps, increased significantly from 80% in years 2004–2007 to 92% in years 2008–2011(t-proportion = 0.87 & CI = 1.7, significant) ( and ). Polyp histology documentation rates increased significantly from 41% in years 2004–2007 to 88% in years 2008–2011 (t-proportion = 3.7 & CI = 7.3, highly significant) ( and ).
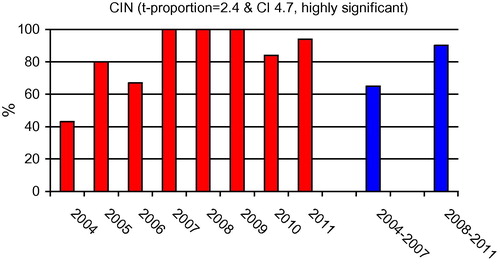
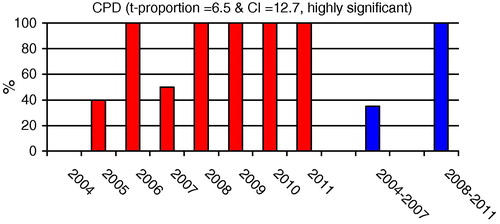
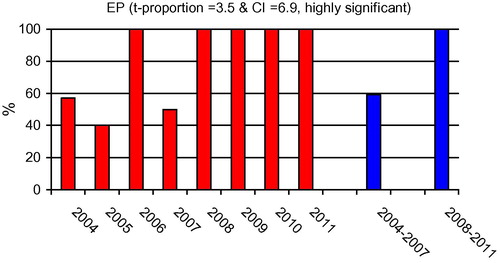
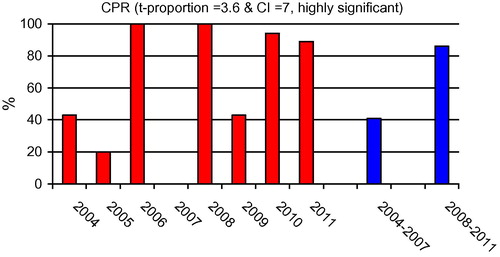
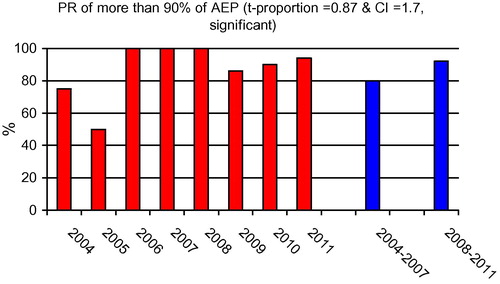
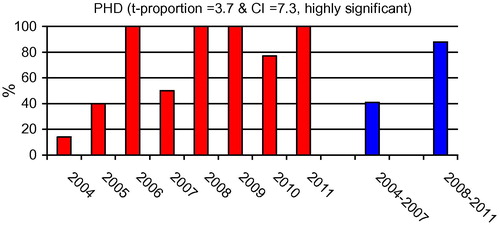
Table 1 Cecal intubation (CIN) rates among studied years.
Table 2 Complete polyp description (CPD) rates among studied years.
Table 3 Endoscopic polypectomy (EP) rates among studied years.
Table 4 Complete polyp removal (CPR) rates among studied years.
Table 5 Polyp retrieval (PR) rates, with retrieval of ⩾90% of all excised polyps among studied years.
Table 6 Polyp histology documentation (PHD) rates among studied years.
4 Discussion
Colonoscopy is a routine procedure in patients of all ages who present with bowel symptoms. Polyps can be identified and removed during colonoscopy thereby reducing the risk of colon cancer.Citation3 The effectiveness of colonoscopy depends on the technical quality of the procedure.Citation15 Brenner et al. reported that when colonoscopy reveals a polyp, the risk of cancer may depend more on colonoscopy-related factors than on the polyp itself.Citation16 Lack of complete removal of all polyps and lack of surveillance colonoscopy within five years were strongly independently associated with later development of colorectal cancer. The presence of at least one colonoscopy-related characteristic (incompleteness, poor bowel preparation, incomplete removal of all polyps, or no surveillance colonoscopy within five years) accounted for 41.1% of the cancer risk, compared with only 21.7% for the presence of at least one of the following polyp characteristics: 1 cm or larger, villous components or high-grade dysplasia, at least three polyps, or at least one proximal polyp.Citation16
Endoscopists should be able to perform polypectomy safely and effectively.Citation3 Because a significant proportion of adenomas were found in the proximal colon (40%), the importance of a complete colonoscopy to the cecum is emphasized.Citation17 Ensuring complete examination of the colon helps reduce the possibility of missing lesions.Citation18 US Multi-Society Task Force on Colorectal Cancer has recommended that clinicians should achieve a cecal intubation rate of at least 90% overall.Citation13 Polyp characteristics are important factors in assessing the risk of malignancy and the likelihood of recurrence in advanced lesions.Citation18 The malignant potential of individual polyps is never known and even small/diminutive polyps can occasionally harbor cancer.Citation3 It is therefore advisable that all polyps (even diminutive rectal polyps) should be removed unless they are obviously non-neoplastic.Citation3 An ineffective polypectomy may be associated with the risk of interval colorectal cancer (cancer diagnosed between screening and post-screening surveillance examinations).Citation19 Population studies have demonstrated greater protection from colon cancer when the endoscopist’s colonoscopy completion and adenoma removal rates are high.Citation19,Citation20 Histological examination of the resected specimens is the only reliable way to classify polyps and exclude malignancy and is therefore an essential determinant of the need for further treatment and endoscopic surveillance.Citation3 An attempt should therefore always be made to retrieve all resected specimens.Citation3 NHS Bowel Cancer Screening Program’s endoscopy quality assurance group recommends retrieval of 90% of all excised polyps for histological evaluation.Citation2
Variation in the quality of colonoscopy is likely to have an important impact on effectiveness and patient outcome, and this has led to a call for the routine assessment of quality, particularly for screening.Citation20 A CQAP was instituted in 2003 in our institution. We previously reported improved cecal intubation rates, patient comfort, detection rate of microscopic colitis and the yield of histological sampling in patients with suspected colorectal cancer by introducing a CQAP.Citation8–Citation10 In this study we report improving the quality of endoscopic polypectomy by introducing a CQAP. Cecal intubation, complete polyp description, polyp removal, recovery and histology documentation rates all markedly improved across the studied years.
Our study, mainly included children and young adults, in these, juvenile polyps were most common. Eleven patients (14%) had adenomatous polyps. They were scheduled for surveillance colonoscopy. Seven patients (9%) attended surveillance colonoscopy during the study period. None of the patients had evidence of malignancy during follow up. Repeat colonoscopy was performed in two patients (3%). Both patients presented with bleeding per rectum. Following colonoscopy and polypectomy rectal bleeding continued. Repeat colonoscopy revealed missed polyps which were removed and bleeding stopped. A systematic review to obtain summary estimates of the polyp miss rate revealed that the pooled miss rate for polyps of any size was 22% (370/1650 polyps).Citation21 Careful examinations are necessary in order not to miss lesions. It is reported that longer withdrawal times plus enhanced inspection techniques have been associated with higher adenoma or polyp detection rates.Citation4 In 2007 we started measuring colonoscopic withdrawal times in negative colonoscopies. The mean colonoscopy withdrawal time was 3 ± 1 min in the year 2007 and increased to 7 ± 3 min in years 2008–2011 (unpublished). Three children had difficult polyps, one involving the base of the appendix, another close to the anal verge and a large one crossing two haustral folds. These polyps were safely removed by the expert endoscopist. There was one complication (1.3%). Perforation occurred from thermal injury by snare polypectomy. The perforation was recognized at the time of endoscopy and was managed surgically. In a prospective study of snare polypectomies among 3976 patients from 13 German institutions, it was reported that perforation occurred in 1.2% of patients.Citation22 The introduction of a continuous quality improvement program did not significantly change the overall incidence of procedure-related complications.Citation23
This study was performed in a setting of self-evaluation and it assessed quality using an approach based on measurement and comparison. It allowed us to detect shortcomings and deviations from the selected standards and enabled a quality improvement process. The quality assurance program is a part of an overall program designed to improve the quality of endoscopy practice in our unit.
5 Conclusion
The implementation of a quality assurance and improvement program does improve the quality of endoscopic polypectomy in patients with polyps detected at colonoscopy.
Conflicts of interest
None declared.
Notes
Available online 6 April 2013
Peer review under responsibility of Alexandria University Faculty of Medicine.
References
- T.W.BalfourTraining for colonoscopyJ R Soc Med941999160161
- NHS bowel cancer screening program publications: quality assurance guidelines for colonoscopy. [Internet]. 2010. Available from:http://www.cancerscreening.nhs.uk/bowel/publications/index.html.
- Riley S. Colonoscopic polypectomy and. endoscopic mucosal resection: a practical guide 2008. [Internet]. Available from: http://www.bsg.org.uk/pdf_word_docs/polypectomy_08.pdf.
- D.A.CorleyC.D.JensenA.R.MarksCan we improve adenoma detection rates? a systematic review of intervention studiesGastrointest Endosc742011656665
- S.J.WinawerA.G.ZauberM.J.O’BrienM.N.HoL.GottliebS.S.SternbergRandomized comparison of surveillance intervals after colonoscopic removal of newly diagnosed adenomatous polyps. The National Polyp Study WorkgroupN Engl J Med3281993901906
- Gado A. Quality assurance in Egypt. World J Gastroenterol News 2007. [Internet]. Available from: http://www.worldgastroenterology.org/assets/downloads/pdf/pub/wgn/wgn2007_1.pdf.
- Gado A. Quality in endoscopy – is it applicable in developing countries? an Egyptian experience. http://GastroHep.com 2009. [Internet]. Available from:http://www.gastrohep.com/freespeech/comments.asp?id=127.
- A.GadoB.EbeidA.AxonHigh quality colonoscopy in a low volume unit; is it achievable?Arab J gastroenterol112010161164
- A.GadoB.EbeidA.MetwaliA.AxonImproving the detection rate of microscopic colitis by introducing a colonoscopy quality assurance programArab J Gastroenterol112010223226
- A.GadoB.EbeidA.AbdelmohsenA.AxonImproving the yield of histological sampling in patients with suspected colorectal cancer during colonoscopy by introducing a colonoscopy quality assurance programGastroenterol Res42011157161
- Gado A, Ebeid B. Impact of a continuous quality improvement program on infection control of endoscopes. Int J Infect Control 2009. [Internet]. Available from: http://www.ijic.info/article/download/3143/2813.
- Gado A, Ebeid B. Are you looking at your channel cleaning brush?. Int J Infect Control 2011. [Internet]. Available from: http://www.ijic.info/article/download/6225/6147.
- D.J.BjorkmanJ.W.PoppMeasuring the quality of endoscopyGastrointest Endosc632006S1S2
- Valori R. BSG Quality and safety indicators for endoscopy 2007. [Internet]. Available from: http://www.grs.scot.nhs.uk.
- J.RaymondB.TissotJ.DartiguesE.Saint-MartinJ.VergierP.MichelQuality assessment of colonoscopy in usual practice in a French area: AquitaineAbstr Int Soc Technol Assess Health Care Meet91993142
- H.BrennerJ.Chang-ClaudeL.JansenC.SeilerM.HoffmeisterRole of colonoscopy and polyp characteristics in colorectal cancer after colonoscopic polyp detection: a population-based case–control studyAnn Intern Med1572012225232
- V.De JongeJ.Sint NicolaasD.L.CahenW.MoolenaarR.J.OuwendijkT.J.TangQuality evaluation of colonoscopy reporting and colonoscopy performance in daily clinical practiceGastrointest Endosc75201298106
- Li J, Nadel M, Poppell C, Dwyer D, Lieberman D, Steinberger E. Quality assessment of colonoscopy reporting: results from a statewide cancer screening program. Diagn Ther Endosc 2010. [Internet]. Available from: http://www.hindawi.com/journals/dte/2010/419796/.
- M.KaminskiJ.RegulaE.KraszewskaM.PolkowskiU.WojciechowskaJ.DidkowskaQuality indicators for colonoscopy and the risk of interval cancerN Engl J Med362201017951803
- N.BaxterR.SutradharS.ForbesL.PaszatR.SaskinL.RabeneckAnalysis of administrative data finds endoscopist quality measures associated with postcolonoscopy colorectal cancerGastroenterology14020116572
- J.C.Van RijnJ.B.ReitsmaJ.StokerP.M.BossuytS.J.van DeventerE.DekkerPolyp miss rate determined by tandem colonoscopy: a systematic reviewAm J Gastroenterol1012006343350
- G.RajuY.SaitoT.MatsudaT.KaltenbachR.SoetiknoEndoscopic management of colonoscopic perforationsGastrointest Endosc74201113801388
- G.ImperialiG.MinoliG.MeucciG.SpinziE.StrocchiV.TerruzziEffectiveness of a continuous quality improvement program on colonoscopy practiceEndoscopy392007314318