Abstract
Many rheumatologic manifestations have been associated with Hepatitis C virus (HCV) infection including; arthralgia, myalgia, fatigue, fibromyalgia, vasculitis, and sicca syndrome. The relationship between emergence and persistence of intrahepatic or circulating B cell clonotypes and HCV infection is still unknown. However accumulating evidences indicate that certain chemokines play a critical role in providing the appropriate environment for activation and expansion of naïve lymphocytes, one of these chemokines is B cell-attracting chemokine-13 (CXCL13).
CXCL13 is a major regulator of B-cell trafficking. This study evaluates circulating levels of CXCL13 protein in chronically HCV-infected Egyptian patients compared with healthy controls and its association with articular synovial hypertrophy. Rheumatic manifestations were present in 85% of patients; included fatigue (20%), arthralgia (the commonest manifestation) (65%), fibromyalgia (22%), myalgia (37%), Rayunad’s phenomenon (10%), peripheral neuropathy and arthritis (2.5%), and tendenitis (7.5). Cryoglobulins recorded in this study were of type II & III mixed cryoglobulins (MC) positive in 25% all of which showed positive rheumatoid factor (RF). Significant low levels of C3 and C4 were reported in the patient group. CXCL13 serum levels were significantly high in the patient group especially in the MC positive group compared to controls. The highest levels of CXCL13 were significantly associated with rheumatologic manifestations with or without mixed cryoglobulinemia and significantly associated with articular synovial hypertrophy.
1 Introduction
Chronic liver disease is an inflammatory disorder recognized with several etiologies and different pathogenetic mechanisms.Citation1 Within the inflamed liver there is an accumulation of different lymphoid and myeloid cells, including T and B cells, local activation of these cells is thought to be essential in perpetuating chronic inflammatory processes and accelerating liver damage. These cells frequently accumulate in the portal tracts and organize follicle-like structures with germinal centers.Citation2 In these sites, local differentiation of follicular dendritic cells, plasma cells, and antibody production may occur.Citation3
Table 1 Comparison between patients and controls as regards laboratory data.
Table 2 Comparison between patients and controls as regards immunological data.
In hepatitis C virus (HCV) infection, distinct B cell expansions contribute to the formation of intraportal follicle-like structures, which have been found to influence the clinical picture that appears to be related to mixed cryoglobulinemia (MC) and high serum levels of rheumatoid factor (RF). Circulating B-cell clonotypes have also been suggested to be of hepatic origin.Citation4 The relationship between emergence and persistence of intrahepatic or circulating B cell clonotypes and HCV infection is still unknown; however accumulating evidences indicate that certain chemokines play a critical role in providing the appropriate environment for activation and expansion of naïve lymphocytes in response to signals delivered by antigen presenting cells.Citation5
CXC ligand 13 (CXCL13), also known as B cell-attracting chemokine 13 or B-lymphocyte chemoattractant, is a member of CXC subtype of the chemokine superfamily,Citation6 its essential role was seen in the establishment and maintenance of lymphoid tissue microarchitecture,Citation7 and it is critical for secondary lymphoid tissue development and distribution of lymphocytes within the microenvironment.
The primary CXCL13 receptor is CXCR5, which is a 7-transmembrane G-protein expressed by B lymphocytes,Citation8 follicular B helper T cells, osteoblasts, and skin derived dendritic cells.Citation9
CXCL13 is constitutively expressed in B cell follicles of secondary lymphoid organs, pleural and peritoneal cavities, and in ectopic lymphoid follicles within the synovial membrane of patients with rheumatoid arthritis.Citation10
Many rheumatologic manifestations have been associated with HCV infection including; arthralgia, myalgia, fatigue, fibromyalgia, vasculitis, and sicca syndrome. Arthralgia is the most common extrahepatic manifestation and may indicate mixed cryoglobulinemia MC.Citation11
The aim of this study is to determine the level of the serum CXCL13 in Egyptian patients with chronic hepatitis C infection (with or without mixed cryoglobulinemia) and to study its association with rheumatologic manifestations.
1.1 Patients and methods
This study was conducted on 40 Egyptian patients with chronic hepatitis C infection (HCV) attending the Internal Medicine & Rheumatology, Rehabilitation inpatient and outpatients Departments, Ain Shams University Hospitals, and 20 normal volunteers matched in age and sex with the patients, serving as a control group. Consents were taken from all subjects included in the study.
Hepatitis C infection was documented with HCV polymerase chain reaction (HCV-PCR).
2 Exclusion criteria include
Patients with hepatitis B surface antigen (HBsAg) or positive cytomegalovirus. Autoimmune hepatitis, hemochromatosis, and alcoholic hepatitis were excluded. Patients with end stage renal disease, diabetic patients, and patients with a history of interferon therapy were also excluded from the study. None of our patients or controls had known rheumatologic disease prior to this present complain (X-ray is done routinely to exclude any rheumatological problems).
All the patients and controls were subjected to the following:
| • | Full medical history taking and clinical examination with special focus on the rheumatological manifestations; mode of onset and its duration; arthralgia, arthritis, synovial hypertrophy, joint effusion, myalgia, tendinitis, tender points of fibromyalgia (according to the criteria of American College of Rheumatology (ACR) 1990), Raynaud’s phenomenon and cutaneous vasculitis. | ||||
| • | Biochemical and Hematological profiles: total bilirubin, alkaline phosphatase, aspartate aminotransferase (AST), alanine aminotransferase (ALT), albumin, total protein, creatinine, CBC and TSH and T3 & T4. (Taken from recorded data of patients’ medical file). | ||||
| • | Immunological profile rheumatoid factor RF, ANA, C3, C4. | ||||
| • | Cryoglobulins. | ||||
| • | Serum level of CXCL13 (ELISA) .The kit (R&D systems, USA). The assay employed the quantitative sandwich enzyme immunoassay technique that makes use of a mouse monoclonal antibody against human CXCL13 precoated onto a microplate. Human recombinant CXCL13 protein at serial concentrations and 2-fold diluted serum samples were pipetted into the wells to allow any CXCL13 to be bound by immobilized antibody. After washing away unbound substances, a mouse monoclonal antibody conjugated with horseradish peroxidase specifically directed against CXCL13 protein was added to the wells. After further washings, stabilized tetramethylbenzidine was added to the wells and color developed in proportion to the amounts of bound CXCL13. Quantikine kit standards were used for the construction of standard curves. The sensitivity threshold of the test was 2 pg/ml. Intra-Assay: CV < 10% and inter Assay: CV < 12%. | ||||
| • | Abdominal ultrasonography (US) was done for accurate assessment and documentation of hepatomegaly, splenomegaly, ascitis and liver cirrhosis. | ||||
| • | Musculoskeletal US was performed for selected joints (those who presented with arthralgia or arthritis with special attention on knees and metacarpophalangeal joints (MCPs)), which was done by an Internist who is an expert in abdominal and musculoskeletal ultrasonography, who was ignorant to the clinical status of the examined subjects using; Toshiba Medical System (Famio Cube) Model SSA-520A (Fundamentals) (2b730-929 EN) with a multifrequency 3.5–11 MHz transducer. Sector transducer with frequency 3.5 MHz was used in abdomen examination. Linear transducer frequency 11 MHz was used in joint examination. The ultrasound examination was performed in accordance to the European League against Rheumatism (EULAR) Guidelines for musculoskeletal US in Rheumatology.Citation12 Joint effusion appears compressible, probe pressure will squeeze fluid into other parts of the joint and, along with the absence of Doppler signal, distinguishes fluid from hypo or anechoic synovitis. Synovial hypertrophy is defined as a solid, non-compressible, hypoechoic tissue in connection to joint lines or surrounding tendons. In the absence of an effusion, synovitis is diagnosed by the presence of an abnormally thickened hypoechoic region.Citation12 | ||||
Real time US examination of individual subject was done, and fixed photos were saved electronically for further discussion with the responsible rheumatologist.
2.1 Statistical analysis
IBM SPSS statistics (V. 20.0, IBM Corp., USA, 2011) was used for data analysis. Data were expressed as Mean ± SD for quantitative parametric measures in addition to both number and percentage for categorized data.
The following tests were done:
| 1. | Comparison between two independent mean groups for parametric data using Student’s t test. | ||||
| 2. | Chi-square test to study the association between each two variables or comparison between two independent groups as regards the categorized data. | ||||
| 3. | Comparison between two proportions as regards in variant categorized data. The probability of error at 0.05 was considered sig., while at 0.01 and 0.001 are highly sig. | ||||
| 4. | Spearman R testing association. | ||||
3 Results
The results of this study revealed that the age of the patients ranged from 17–54 years with a mean value of 40.7 ± 7.33 years, they were; 19 males (47.5%), and 21 (52.5%) females. While the control group was; 10 males (50%) and 10 females (50%), their age ranged from 25 to 50 years with a mean value of 40 ± 7.1 years. No statistically significant differences were detected between the two groups as regards age and sex. Disease duration ranged from few months to several years as the exact onset is not reported and all the cases were accidentally discovered.
3.1 Clinical data of the patients as regards the hepatic manifestations
Jaundice was detected in 18 patients, nine patients had lower limb edema, fever was present in three patients (low grade of no special pattern), two patients had cervical lymphadenopathy, 14 had hepatomegaly confirmed with US, eight patients had ascites and 13 patients had splenomegaly and liver cirrhosis also confirmed with abdominal US. Comparing these findings to controls (who did not show any of these abnormal findings) there was a significant statistical difference between patients and controls as regards; jaundice, hepatomegaly and liver cirrhosis (US findings), lower limb edema, and ascites and a non significant difference as regards; fever and lymphadenopathy.
3.2 Rheumatic manifestations of patients
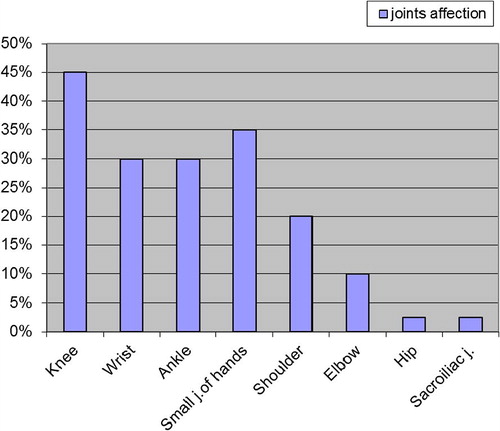
Disease duration of different rheumatic manifestations ranged from 6 months–3 years. The prevalence of rheumatological manifestation was 85% (34 patients), chronic fatigue was recorded in eight patients (20%), arthralgia in 26 patients (65%) with different distributions as shown in (); knee 45%, small joints of the hand 35%, wrist and ankle 30%, shoulder 20%, elbow 10%, hip & sacroiliac 2.5%. The onset was monoarticular in 20/26 (76%), oligoarticular in 4/26 (15.3%), and polyarticular in 2/26 (7.6%). The full picture of arthritis was documented in only one patient 2.5% (in the knee joint). The arthralgia/arthritis they expressed was of no specific pattern and was not associated with morning stiffness. Myalgia of calf muscles and trapezii was reported in 15 patients (37.5%), fibromyalgia was present in nine patients (22%). Tendinitis (bicipital tendinitis) was reported in three patients (7.5%), Achilles tendinitis in one patient (2.5%), Raynaud’s phenomenon in four patients (10%), Sicca syndrome in four patients (10%) (manifested as xerophthalmia). Peripheral neuropathy was detected in one patient (2.5%). None of the patients had purpura or cutaneous vasculitis. Rheumatic manifestations were not recorded in any of the controls. A significant statistical difference was noted between the patient and control groups as regards; arthralgia, myalgia (P < 0.001) and chronic fatigue and fibromyalgia (P < 0.05). Non-significant differences as regards arthritis, tendinitis, Raynaud’s phenomenon, Sicca syndrome and peripheral neuropathy (P < 0.05) were also recorded.
3.3 Laboratory data of the patients and controls are shown in ()
This table shows a comparison between mean and standard deviation of main laboratory data of patients and controls. Highly significant statistical differences were noted for total bilirubin, AST, ALT, albumin and a non-significant difference for; total protein, creatinine, platelets and white blood cells.
3.4 Immunological data of the patients and controls are shown in ()
Neither the patients nor the controls showed positive ANA. Cryoglobulins were detected in 10 patients (25%), Rheumatoid factor was positive in 22 patients (55%), and in one of the controls (5%). None of the controls showed positive cryoglobulins. Comparison between patients and controls, showed a highly significant difference as regards Rheumatoid factor, complement 3, and level of CXCL 13 proteins, and a significant difference as regards cryoglobulins and complement 4, with low levels of C3 & C4 in the patient group. All the recorded cryoglobulins were of type II & III (mixed cryoglobulins), the cryocrit percent ranged from 0.5% to 2%.
The patients’ group was further divided into two subgroups according to the presence of cryoglobulins into group A which included 10 patients and, group B without cryoglobulins, which included 30 patients. Rheumatic manifestations were present in 8/10 patients (80%). On comparing the prevalence of rheumatic manifestations in group A & group B, there was no statistically significant difference ().
Table 3 Comparison between cryoglobulin positive and negative patients as regards prevalence of rheumatic manifestations.
On comparing the laboratory data of groups A and B, there was a highly significant difference as regards the mean values of AST, ALT and albumin levels. On comparing the immunological data of groups A and B there was a significant difference as regards the presence of positive RF which was present in 10/10 cryoglobulin positive patients (100%) versus 12 cryoglobulin negative patients (40%). CXCL 13 levels ranged from 200–371 & 90–150 pg/L with a mean value of 260.45 ± 46.05 and 148.8 ± 60.74 for groups A and B, respectively. This showed a highly significant difference (P < 0.001). Non-significant difference was recorded for the other laboratory and immunological data.
3.5 Abdominal ultrasonography
Abdominal US confirmed the clinical data, which showed that 14 patients had hepatomegaly (35%). Ascitis was present in eight patients (20%), and liver cirrhosis was present in 13 patients (32%). On comparing the prevalence of hepatomegaly, ascitis and liver cirrhosis between groups A and B, hepatomegaly and ascitis for group A were significantly higher ().
Table 4 Comparison between US findings of cryoglobulin positive and negative patients.
3.6 Musculoskeletal US
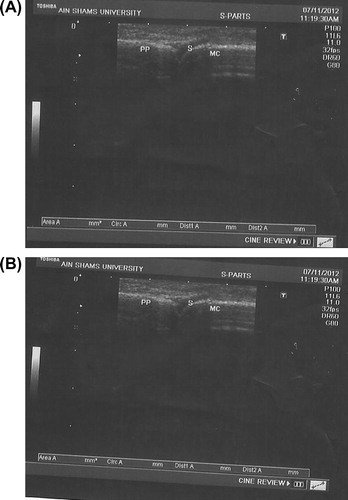
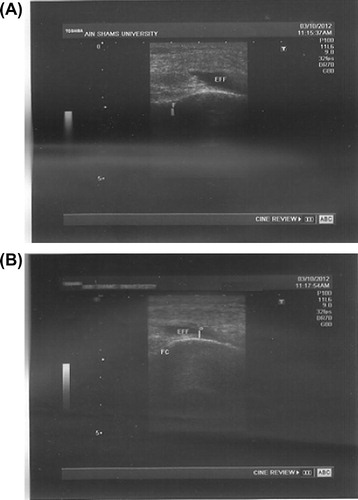
High frequency linear transducer 11 MHZ, was used in evaluation of 26 of our patients for the presence of clinically detectable abnormalities (tenderness, and/or swelling of the joints). Joints were assessed for the presence of bone erosion, synovial effusion, and joint effusions. Hypertrophy of the synovial membrane of the knee was detected in five patients (12.5%). However it was also detected in the MCP joints of nine patients (22.5%) (). Knee joint effusion was detected in 5 patients (12.5%) (), and sporadic tendenitis was detected in 10 (25%) patients.
On studying the level of CXCL 13 among the patients with synovial hypertrophy (knees and MCPs) and those without, there was a significant difference as seen below (P < 0.03). Testing the association of level of CXCL 13 and synovial membrane hypertrophy (R 0.27), (P < 0.003) a significant association was found ().
Table 5 Comparison of the levels of CXCl3 between patients with and without synovial hypertrophy.
4 Discussion
Egypt has a high prevalence of antibodies to hepatitis C virus (HCV), estimated nationally at 14.7%. Numerous HCV prevalence studies in Egypt have published various estimates from different Egyptian communities. Incidence from the previous community studies was 6.9/1000 per person per year. More than 500,000 new HCV infections per year were estimated. Iatrogenic transmission is the most likely way of transmission.Citation13 Clinical sequels of HCV account for a significant proportion of patients presenting to the hepatologist with well described manifestations of hepatitis C including; hepatomegaly, cirrhosis, lower limb edema, ascites and even hepatocellular carcinoma. The extrahepatic manifestations of hepatitis C infection, though common, are less well appreciated as recorded by Sterling and Bralow in 2006 where they stated that 36% of their studied group had extrahepatic manifestations. The most prevalent extrahepatic manifestations are the rheumatologic manifestations; fatigue, arthralgia and essential mixed cryoglobulinemia.Citation14 These various rheumatological symptoms have no specific pattern fulfilling the diagnostic criteria of the American college of Rheumatology (ACR).
Although HCV is a hepatotropic virus, in some patients the primary manifestations of infection occur outside the liver, as autoimmune manifestations, which can be dominant, whereas the hepatic disease can be quiescent or mild.Citation15
This work was designed to study the rheumatologic manifestations of HCV. Our results showed that the overall prevalence of any rheumatic manifestations was 85%, which is similar to the results of Stefanova–Petrova et al.Citation16 who found 76% of the studied Bulgarian patients who had at least one extrahepatic manifestation. However their clinical manifestations were not in accordance with our results except for Raynaud’s phenomenon; (11.8% vs. 10%). Our results were also similar to the results of Sadek et al. in 2003Citation17, where they stated that the overall prevalence of rheumatologic manifestations was 89.3% in a study of 75 Egyptian patients with chronic HCV in El-Minia region. Our results were higher than those of Mohammed et al.Citation18 where they reported that the overall estimated prevalence of rheumatologic manifestations was 16.39% in their study of 306 Egyptian patients with HCV attending the National Hepatology and Tropical Medicine Research Institute. Our higher prevalence of the overall rheumatologic manifestations could be explained; as most of the selected cases in this study were chosen from those attending or referred to the Rheumatology clinic, and also the long standing disease process as 32% of our studied patients had liver cirrhosis. Arthralgia was the commonest extrahepatic manifestation, followed by myalgia, fibromyalgia, and chronic fatigue. These results are in accord with other studies.Citation11,Citation16–Citation18 Buskila et al. also reported that rheumatologic manifestations of HCV infection are common and include, myalgia, arthritis, and fibromyalgia and sicca symptoms, and the most commonly involved joints were; metacarpophalangeal, proximal, interphalangeal, wrist, shoulder, and knees, which are similar to our results.Citation19,Citation20
As regards HCV-related arthropathy; it commonly presents as symmetrical inflammatory arthritis involving small joints. The joints involved are similar to rheumatoid arthritis (RA). This sometimes makes it difficult to differentiate true RA from HCV patients with a positive rheumatoid factor but without RA.
In our study, 35% of our patients had symmetrical small joint affection of the hands, this result was in agreement with Zuckerman et al.Citation21 and Nyigni et al. in 2010.Citation22 Differentiating HCV-related arthropathies from classic RA is essential. In contrast to patients who have RA, our patients experienced minimal morning stiffness, did not exhibit rheumatoid nodules and there was no evidence of erosive arthritis. Anti ccp antibodies were not done, however it is a definite lab test to distinguish RA from HCV associated arthropathies and we should recommend it to be done in further similar studies.
Ultrasound is a promising tool for musculoskeletal assessment of patients with rheumatologic manifestations. Ultrasound has a particular advantage that an experienced observer can rapidly screen several joints in a relatively short time.Citation23 Positive findings were detected in 26 (85%) of our HCV patients. None of our patients had erosion arthritis, this was in agreement with Nyingi et al. in 2010Citation22 who concluded that no radiological features distinguish HCV-related arthritis from arthritis caused by other disorders. However, an important clinical characteristic of HCV-related arthropathy is the lack of bone erosions on imaging; therefore, imaging is essential in the diagnostic workup to evaluate for other causes of arthritis. Neither synovial fluid analysis nor synovial tissue biopsy has been useful in the diagnosis of HCV-related arthropathy; ultimately, this is a diagnosis of exclusion.Citation22,Citation23
As regards our laboratory and immunological results, they were similar to the results of Saadoun et al. in 2007Citation24 who stated that circulating mixed cryoglobulins (MC) are present in 40–60% of HCV-infected patients, this is also augmented by old studies which showed that mixed cryoglobulinemia has a clinically significant association with chronic HCV infection, particularly in those with long duration of liver disease and cirrhosis.Citation25,Citation26 MCs reflect the expansion of B cells producing a pathogenic IgM with rheumatoid factor (RF) activity. Its expression can be variable including palpable purpura, cutaneous vasculitis, arthralgias, neuropathy or Raynaud’s phenomenon. This was shown in our study, where we found 80% of patients with +ve cryoglobulins expressed rheumatologic findings, although it did not show a significant difference from the control group, yet it could be due to the low cryocrit percent as stated by Leone et al.Citation27 where they found 51/114 (44.7%) patients with HCV infection with MC complained from rheumatological symptoms and the mean cryocrit value in these patients was 2.6%, while in patients with HCV infection with MC without rheumatological symptoms the cryocrit value was lower than 0.5% in 50% of cases.Citation27
The third component of human complement (C3) plays a central role in innate immune function as its activation is required to trigger classical as well as alternative complement pathways. This complement system has been shown to contribute to the protection of the host from virus infection.Citation28,Citation29
In this study, we observed that sera from patients chronically infected with HCV displayed significantly lower C3 and C4 levels than sera from controls, which agrees with another study which demonstrated that sera from patients chronically infected HCV displayed significantly lower C3 levels than sera from healthy individuals and also liver biopsy specimens from the same patients also exhibited lower C3 mRNA expression than liver tissues from healthy donors.Citation29,Citation30
HCV plays a critical role in a wide variety of inflammatory processes by regulating the expression of transcriptional factors and proinflammatory genes, including tumor necrosis factor and members of its superfamily, interleukins, and chemokines.Citation31 Chemokines have been shown to orchestrate migration and preferential sequestration of B and T cells in HCV-infected compartments. Indeed, an increased number of circulating B cells has been demonstrated in these patients, probably reflecting deregulation of B-cell traffic. The homeostatic trafficking of B cells is mainly regulated by the chemokine CXCL13 through interaction with CXCR5, its only known receptor, expressed on all mature circulating B cells and on a subset of memory CD4 T cells.Citation32
MC is a systemic small-vessel vasculitis; B-cell expansion is the biological substrate of the disease. It can be regarded as a benign lymphoproliferative condition that may evolve into frank lymphoma. HCV infection is the main causative factor of MC,Citation33 HCV lymphotropism is responsible for poly-oligoclonal B-lymphocyte expansion with a consequent production of different autoantibodies and immune-complexes, including cryoglobulins, which are characterized by the coexistence of autoimmune and lymphoproliferative alterations. Therefore, it represents the prototype of HCV-associated disorders.Citation34 Moreover the most frequent and clinically important endocrine HCV related extrahepatic diseases (HCV-EHDs) are thyroid disorders. However none of our patients showed thyroid disorders. A possible common immunological Th1 pattern could be the pathophysiological base of the association of HCV-EHDs, with thyroid autoimmunity. In fact, HCV infection of thyrocytes may act by upregulating CXCL10 secretion in these cells that is responsible for Th1 lymphocyte recruitment. Th1 response leads to increased IFNγ and TNFα production that in turn stimulates CXCL10 secretion by the target cells, thus perpetuating the immune cascade. This process may lead to the appearance of thyroid autoimmune disorders in genetically predisposed subjects.Citation35
In this study, serum CXCL13 levels were found to be elevated in chronic HCV infection compared with healthy controls with the highest levels found in HCV-infected cryoglobulinemic patients, and in patients with articular synovial hypertrophy with a significant association with synovial hypertrophy. Both of these results confirm the coexistence of both autoimmune and lymphoproliferative alterations of chronic HCV (indicated in group A by the presence of liver cirrohsis and ascitis) associated disorders as described in previous studies.Citation33,Citation36 A similar study found levels of CXCL13 were significantly higher in RA compared to healthy controls and correlated with measures of synovitis, which emerged as a new biological marker in early RA, accurate in assessing the severity of synovitis.Citation37 These high serum levels of CXCL13 may be a consequence of high local production, which is a perpetuation of the augmented autoimmune (manifested as MC) and lymphoproliferative state (manifested as synovial hypertrophy and musculoskeletal manifestations) induced by the ongoing chronic hepatic inflammation, which maintains the pathologic process in tissues by attracting additional lymphocytes and more B cell proliferation and over production of CXCL 13 leading to chronic damage.Citation38
5 Conclusion
In this study, serum CXCL13 levels were found to be elevated in chronic HCV infection compared with healthy controls. High levels correlated with HCV extrahepatic musculoskeletal manifestations with mixed cryoglobulinemia and were significantly associated with articular synovial hypertrophy.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 17 April 2013
References
- M.JacynaG.Millward-SadlerH.ThomasChronic hepatitisG.H.Millward-SadlerR.WrightM.J.P.ArthurWright’s liver and biliary disease1992SaundersLondon787820
- J.MosnierC.DegottP.MarcellinD.HeninS.ErlingerJ.P.BenhamouThe intraportal lymphoid nodule and its environment in chronic hepatitis C: an immunohistochemical studyHepatology171993366371
- J.MuakamiY.ShimizuY.KashiiFunctional B cell response in intrahepatic lymphoid follicles in chronic hepatitis CHepatology301999143150
- B.RehermannInteraction between hepatitis C virus and the immune systemSemin Liver Dis202000127141
- A.RotU.H.Von AndrianChemokines in innate and adaptive host defense: basic chemokinese grammar for immune cellsAnnu Rev Immunol222004891928
- D.LeglerM.LoetscherR.S.RoosI.Clark-LewisM.BaggioliniB.MoserB cell-attracting chemokine-1, a human CXC chemokine expressed in lymphoid tissuesJ Exp Med1871998655660
- J.CysterK.AnselK.ReifE.EklandP.HymanH.TangFollicular stromal cells and lymphocyte homing to folliclesImmunol Rev1762000181193
- K.AnselV.NgoP.HymanS.LutherR.ForsterJ.SedgwickA chemokine-driven positive feedback loop organizes lymphoid folliclesNature4062000309314
- H.SaekiM.WuE.OlaszS.HwangA migratory population of skin–derived dendritic cells expresses CXCR5, responds to B lymphocyte chemoattractant in vitro, and co-localizes to B cell zones in lymph nodes in vivoEur J Immunol30200028082814
- K.ShiK.HayashidaM.KanekoLymphoid chemokine B cell-attracting chemokine-1 (CXCL13) is expressed in germinal center of ectopic lymphoid follicles within the synovium of chronic arthritis patientsJ Immunol1662001650655
- C.LormeauG.FalgaroneD.RoulotBoissier MC Rheumatologic manifestations of chronic hepatitis C infectionJoint Bone Spine7362006633638
- M.BackhausG.R.BurmesterT.GerberW.GrassiK.P.MacholdW.A.SwenWorking group for musculoskeletal ultrasound in the EULAR standing committee on international clinical studies including therapeutic trials: guidelines for musculoskeletal ultrasound in rheumatologyAnn Rheum Dis602001641649
- F.DeWolfeA.MillerJ.Abu-RaddadEvidence of intense ongoing endemic transmission of hepatitis C virus in EgyptPNAS1073320101475714762
- R.SterlingS.BralowExtrahepatic manifestations of hepatitis C virusCurr Gastroenterol Rep8120065359
- M.KhattabM.EslamS.AlavianHepatitis C virus as a multifaceted disease: a simple and updated approach for extrahepatic manifestations of hepatitis C virus infectionHepat Mon1042010258269
- D.Stefanava-PetrovaA.TzvetanskaE.NaumovaA.MihailovaE.HadjievR.DikovaChronic hepatitis C virus infection: prevalence of extrahepatic manifestations and association with cryoglobulinemia in Bulgarian patientsWorld J Gastroenterol4813200765186528 [28]
- Sadek H, Abd El wahab J, El sharkawi E, El Labban A. Rheumatic manifestations of Hepatitis C infection, Thesis submitted for partial fulfilment of MD degree in Rheumatology and Rehabilitation, Faculty of Medicine El-Minia University, Egypt, 2003.
- R.MohammedH.El MakhzangyA.GamalF.MekkyM.El KassasN.MohammedPrevalence of rheumatologic manifestations of chronic hepatitis C virus infection among EgyptiansClin Rheumatol2912201013731380
- D.BuskilaHepatitis C-associated arthritisCurr Opin Rheumatol1242000295299
- D.BuskilaHepatitis C-associated rheumatic disordersRheum Dis Clin North Am3512009111123
- E.ZuckermanD.YeshurunI.RosnerManagement of hepatitis C virus-related arthritisBio Drugs1592001573584
- N.M.KemmerK.E.ShermanHepatitis C-related arthropathy: Diagnostic and treatment considerationsJ Musculoskelet Med2792010351354
- N.BoutryM.MorelR.FlipoX.DemondionA.CottonAJR: early rheumatoid arthritis: a review of MRI and sonographic findingsAJR189200715021509
- D.SaadounD.LanauL.CalabreseP.CacoubHepatitis C-associated mixed cryoglobulinemia: a crossroad between autoimmunity and lymphoproliferationRheumatology46200712341242
- K.TanakaT.AiyamaJ.ImaiSerum cryoglobulin and chronic hepatitis C virus disease among Japanese patientsAm J Gastroenterol9010199518471852
- W.SchmidtJ.StapletonD.LabnrecqueHepatitis C virus (HCV) infection and cryoglobulinemia: Analysis of whole blood and plasma HCV-RNA concentrations and correlation with liver histologyHepatology312000737744
- N.LeoneR.PellicanoI.Ariata MaioccoV.ModenaG.MariettiM.RizzettoMixed cryoglobulinaemia and chronic hepatitis C virus infection: the rheumatic manifestationsJ Med Virol6622002200203
- B.MazumdarH.KimK.MeyerS.K.BoseA.M.Di BisceglieR.B.RayHepatitis C virus proteins inhibit C3 complement productionJ Virol864201222212228
- E.MehlhopM.S.DiamondProtective immune responses against West Nile virus are primed by distinct complement activation pathwaysJ Exp Med203200613711381
- A.BanerjeeB.MazumdarK.MeyerA.M.Di BisceglieR.B.RayR.RayTranscriptional repression of C4 complement by hepatitis C virus proteinsJ Virol859201141574166
- I.RiojaF.HughesC.SharpPotential novel biomarkers of disease activity in rheumatoid arthritis patients: CXCL13, CCL23, transforming growth factor alpha, tumor necrosis factor receptor superfamily member 9, and macrophage colony-stimulating factorArthritis Rheum58200822572267
- D.SansonnoF.DammaccoHepatitis C virus, cryoglobulinemia, and vasculitis: immune complex relationsLancet Infect Dis52005227236
- C.FerriA.AntonelliM.MasciaM.SebastianiP.FallahiD.FerrariB cell and mixed cryoglobulinemiaAutoimmun Rev722007114120
- C.FerriA.AntonelliM.MasciaM.SebastianiP.FallahiD.FerrariHCV-related autoimmune and neoplastic disorders: the HCV syndromeDig Liver Dis392007 S1
- A.AntonelliC.FerriS.FerrariM.ColaciP.FallahiImmunopathogenesis of HCV-related endocrine manifestations in chronic hepatitis and mixed cryoglobulinemiaAutoimmun Rev8120081823
- D.SansonnoL.SansonnoFAnna TucciLDammaccoGLaulettaMMontroneIncreased serum levels of the chemokine CXCL13 and up-regulation of its gene expression are distinctive features of HCV-related cryoglobulinemia and correlate with active cutaneous vasculitisBlood112200816201676
- S.BugattiA.ManzoF.BenaglioC.KlersyB.VitoloM.TodoertiSerum levels of CXCL13 are associated with ultrasonographic synovitis and predict power Doppler persistence in early rheumatoid arthritis treated with non-biological disease-modifying anti-rheumatic drugsArthritis Res Ther1412012R34
- D.SansonnoG.LaulettaM.MontroneF.A.TucciL.NisiF.DammaccoVirologic analysis and phenotypic characterization of peripheral blood lymphocytes of hepatitis C virus-infected patients with and without mixed cryoglobulinemiaClin Exp Immunol1432006288296