Abstract
Hepatocellular carcinoma (HCC) is the third most frequent cause of cancer mortality among men worldwide. Serotonin is biogenic amine, ligand for family of 5-HT receptors reflect the diversity of serotonergic actions.Majority of serotonin in body 90% synthesised by enterochromaffin cells of the gastrointestinal tract and exported to various sites. Serotonin regulate blood flow and vascular tone at portal and sinusoidal levels, serotonin mitogen for hepatocytes and promotes liver regeneration. 5HT emerging as mediator of different pathological conditions (double edged sowrd). It contributes to liver fibrosis, mediates oxidative stress in nonalcoholic steatotic hepatitis and aggravates viral hepatitis, these conditions involved in tumorgenesis of hepatocellular carcinoma (HCC). Impaired metabolic function in liver cirrhosis and slow uptake and storage of serotonin by the platelets is sequelae of kinetic change of serotonin transport mechanisms or abnormal serotonin release from dense granules of activated platelets condition defined “platelet exhaustion”, contributes to elevated plasma serotonin which may facilitate tumor growth of primary liver hepatocellular carcinoma. Aim of this work: was to determine whether serotonin is a marker for the diagnosis of hepatocellular carcinoma in cirrhotic patients. Methods: patients were classified into 2 groups; 45 patients with cirrhosis only and 30 patients with cirrhosis and HCC. 10 healthy subjects was taken as controls. Patients underwent; full history taking,clinical examination,abdominal ultrasonography. Laboratory methods include SGOT, SGPT, GGT, bilirubin, alkaline phosphatase, total proteins, albumin, CBC, prothrombin, INR, APRI score, Child-Pugh score, MELD score, AFP and serum serotonin. Results: plasma serotonin was significantly higher in patients group with cirrhosis with a median level 119.4 ng/ml than in control group showed median value of 51.5 ng/ml p< 0.001.Also a significance difference between cirrhosis &HCC group with median value 478.35 ng/ml than control group and cirrhosis group p<0.001was found. Conclusion: Plasma serotonin level was significantly higher in patients with cirrhosis and HCC than in those with cirrhosis only and it was involved in tumorgenesis of hepatocellular carcinoma.
1 Introduction
Each year, hepatocellular carcinoma (HCC) is diagnosed in more than half a million people worldwide, including approximately 20,000 new cases in the United States.Citation1Liver cancer is the fifth most common cancer in men and the seventh in women. Most of the burden of disease (85%) is borne in developing countries.Citation2Incidence of HCC in Egypt is currently increasing, which may be the result of a shift in the relative importance of HBV and HCV as primary risk factors in addition to exposure to aflatoxin as an additional risk factor.Citation3–Citation5HCC is the second most frequent cause of cancer incidence and mortality among men in Egypt.Citation6Egypt has the highest prevalence of HCV in the world, with estimates ranging from 6 to 28% and a reported average of ∼ 13.8%, also investigations in Egypt have also shown the increasing importance of HCV infection in the etiology of HCC, account for 40-50% of cases.Citation3,Citation5,Citation7,Citation8
HCV mostly plays an indirect role in tumor development and appears to increase the risk of HCC by promoting fibrosis and cirrhosis.Citation5,Citation9On the other hand, HCV may play a direct role in hepatic carcinogenesis through involvement of viral gene products in inducing liver cell proliferation. However, it seems that cirrhosis is the common pathway by which several risk factors exert their carcinogenic effect.Citation9,Citation10
The diagnosis of HCC is made by liver imaging tests such as abdominal ultrasound, helical CT scan or triple phase CT scan in combination with measurement of serum markers such as alpha-fetoprotein (AFP) which has been used as a serum marker for HCC for many years but this test had a sensitivity of 39%-65%, a specificity of 76%-94% in the presence of HCC.Citation11,Citation12
Unfortunately, up to 42% of patients with HCC present with serum AFP levels within normal values and also the fibrolamellar type of HCC not secrete AFP.Citation13,Citation14On the other hand, the AFP could also be elevated in pregnancy, other tumors of gonadal origin even in acute or chronic viral hepatitis and liver cirrhosis.Citation11,Citation15,Citation16
Serotonin is known as 5-hydroxytryptamine (5-HT), a biogenic amine that function as a ligand for a large family of 5-HT receptors.Citation17The majority of serotonin in the body (90%) is synthesized by enterochromaffin cells of the gastrointestinal (GI) tract, where it regulates intestinal motility.Citation18
It plays a major role in neurotransmission within the central nervous system (CNS) and the autonomic nervous system (ANS), In the CNS serotonin is known to control mood, behavior, learning, sleep and anxiety. Peripherally, serotonin is able to mediate vascular contraction and relaxation, cell proliferation, apoptosis and platelet aggregation.Citation19
Serotonin is actively taken up by cells expressing the Na+/Cl− dependent serotonin transporter (SERT) where it is stored in intracellular vesicles and released in response to various stimuli. Once bound to target receptors or taken up by the SERT, internalised serotonin can be metabolised by monoamine oxidase (MAO) leading to the generation of 5-hydroxyindoleacetaldehyde (5-HIAA) which is excreted in urine.Citation19,Citation20
Platelets are responsible for picking up serotonin from the gut and lungs and provide the main peripheral storehouse of serotonin, platelets release serotonin in sites of injury where it contributes to platelet recruitment and thrombus propagation .Citation21,Citation22
The family of receptors that bind serotonin is subdivided into seven subgroups and where appropriate these subgroups are again divided reflect the diversity of serotonergic actions. All members of the serotonin receptor family are linked to G-proteins, except the 5-HT3 receptor which is a ligand gated Na+/K+ channel.Citation19,Citation23
With respect to the liver, it was found that serotonin has the ability to regulate hepatic blood flow at both the portal and sinusoidal levels.Citation19
Intraportal injections of serotonin were found to significantly increase portal pressure, events that were antagonized by serotonin antagonist (ketanserin) in portal hypertensive rats,this suggests that serotonergic mechanisms may contribute to maintaining portal hypertension in patients with cirrhosis. Serotonin may play a role in hepatic regeneration following partial hepatectomy in rodents.Citation24–Citation27One resident of the hepatic sinusoid that is postulated to regulate blood flow is the hepatic stellate cell (HSC). The HSC is known to undergo an activation process acquiring a smooth muscle cell-like phenotype with enhanced contractile capabilities in response to liver injury and are instructed by the serotonin to make more scar tissue and switch off the healthy regeneration, also has recently been demonstrated to express functional 5-HT2A and 5-HT2B receptors and therefore it is possible that HSC is able to regulate sinusoidal blood flow. Sinusoidal endothelial cells (SECs) are also known to respond to serotonin inducing contraction of fenestrae.Citation28–Citation30
Patients with advanced liver disease often present with variceal haemorrhage and a more generalised “bleeding tendency”. These additional symptoms linked to hepatic cirrhosis are thought in part to be due to impaired platelet aggregation. Under normal conditions platelets operating as buffers, maintain low levels of free circulating serotonin, are activated in response to a variety of different stimuli, releasing various aggregating factors including serotonin, and following this they become exhausted.
Patients with cirrhosis are known to have Platelet storage pool defects, significantly lower intraplatelet serotonin concentrations when compared to healthy individuals. It is therefore tempting to propose that the reduced platelet serotonin storage ability were in part responsible for the haemorrhagic tendency of cirrhotic patients.Citation19,Citation31,Citation32
The liver and platelets display a very intimate, complex interconnection. The liver plays a critical role even during the synthesis of platelets from megakaryocytes through thrombopoetin(TPO) which was the most important growth factor in the regulation of megakaryocyte development and platelet production, is produced mainly in the liver and kidney.
Hence platelets are not expected to function properly in diseased liver. Platelets harbour important growth factors for liver regeneration, e.g. Hepatocyte growth factor (HGF). Contrariwise, platelets contain Transforming growth factor α (TGF-α), which is required for termination of liver regeneration. Thus, it is plausible that platelets may participate in orchestrating liver regeneration through stimulation and inhibition of growth-related signals. The ability of serotonin to modulate all of these factors renders it crucial in times of hepatic injury and repair .Citation33
Platelet derived serotonin has been shown to be beneficial in terms of stimulating hepatocyte proliferation following hepatic ischaemia in mice.Citation34In addition over proliferation of hepatocytes can lead to HCC and this would raise the possibility that serotonin may play a role in HCC pathogenesis.Citation19
Serotonin is emerging as a mediator of different pathological conditions. It contributes to liver fibrosis, mediates oxidative stress in nonalcoholic steatotic hepatitis, and aggravates viral hepatitis promoting the progression of steatohepatitis by oxidative stress .Citation30,Citation35,Citation36It promotes tumor growth in a mouse model of subcutaneous colon cancer allografts. 5HT deficiency led to decreased vascularity and increased necrosis reflecting cell death of the tumorCitation37
High levels of plasma serotonin in the liver cirrhosis could be due to slow uptake and storage of serotonin by the platelets as could be the sequelae of the kinetic change of serotonin transport mechanisms or abnormal serotonin release from dense granules of activated platelets. Concentration of circulating serotonin in liver cirrhosis can be influenced by other factors, such as altered serotonin catabolism due to an elevated activity of monoamino oxidase and impaired metabolism of tryptophan, as serotonin precursor. Impaired metabolic function in liver cirrhosis contributes to elevated plasma serotoninCitation38
2 Aim
The aim of this work was to evaluate the role of serotonin in the diagnosis of hepatocellular carcinoma in cirrhotic patients.
3 Methods
The studied subjects were recruited from hepatology department in medical research institute, Alexandria university Written confined consent was obtained from all participants before starting the study.
The patients were subdivided into 2 groups:
| 1- | Forty five cirrhotic patients (Group I). | ||||
| 2- | Thirty cirrhotic patients with hepatocellular carcinoma (HCC) (Group II). | ||||
| 3- | Ten healthy persons were considered as control group. | ||||
All subjects were subjected to full history taking, clinical examination with measurement of mean blood pressure and calculation of body mass index (BMI) using the formula: weight in kg /height in metersCitation2,Citation39in addition to an abdominal ultrasonograply and computed tomography .
Patients are matched for age, gender and body mass index. All had clinically evident portal hypertension, none of them had episodes of bacterial peritonitis and free from other neoplastic diseases.
A routine biochemical evaluation was performed as follow:
| a) | Liver function tests including serum aspartate and alanine aminotransferase. (AST+ALT), Gamma Glutamyl Transpeptidase (GGT), Alkaline Phosphatase (ALP),Total proteins, Albumin, Bilirubin (Total and direct).Citation40 | ||||
| b) | Complete blood picture, Prothrombin activity and INR.Citation41 | ||||
| c) | Calculation of Aspartate Aminotransferase –to– Platelet ratio index (APRI) score using the formula: (AST/upper limit of normal × 100) /platelet count. The reference value of AST was considered to be 45 IU, which is the upper normal limit in our laboratory.Citation42 | ||||
| d) | Hepatitis virus markers: Hepatitis B surface antigen done by Eliza technique..Citation43 Hepatitis C virus antibodies done by Eliza technique.Citation44 | ||||
| e) | Child – PughCitation45 and Model of end stage liver disease (MELD) scores were evaluated.Citation46 | ||||
| f) | Determination of serum AFPCitation47 and serotoninCitation48 by Eliza technique. | ||||
3.1 Statistical analysis
Data were fed to the computer using the Predictive Analytics Software (PASW Statistics 18).
Qualitative data were described using number and percent. Association between categorical variables was tested using Chi-square test. When more than 20% of the cells have expected count less than 5, correction for chi-square was conducted using Firsher’s Exact test or Monte Carlo correction.
Quantitative data were described using median, minimum and maximum as well as mean and standard deviation.
The distributions of quantitative variables were tested for normality using Kolmogorov-Smirnov test, Shapiro-Wilk test. D’Agstino test was used if there was a conflict between the two previous tests. If it reveals normal data distribution, parametric tests was applied. If the data were abnormally distributed, non-parametric tests were used.
For normally distributed data, comparison between two independent population were done using independent t-test while more than two population were analyzed F-test (ANOVA) to be used and Post Hoc test (LSD). Correlations between two quantitative variables were assessed using Pearson coefficient.
For abnormally distributed data, Mann-Whitney Test (for data distribution that was significantly deviated from normal) were used to analyze two independent population. If more than two population were analyzed Kruskal Wallis test to be used. Correlations between two quantitative variables were assessed using Spearman coefficient.
Agreement of the different predictives with the outcome was used and was expressed in sensitivity, specificity, positive predictive value, negative predictive value and accuracy. Receiver operating characteristic curve (ROC) was plotted to analyse a recommended cutoff, the area under the ROC curve denotes the diagnostic performance of the test. Area more than 50% gives acceptable performance and area about 100% is the best performance for the test.
Significance test results were quoted as two-tailed probabilities. Significance of the obtained results was judged at the 5% level.
4 Results
Patients enrolled in this study were subdivided into 2groups:
Group I included 33(73.3%) cirrhotic male and 12 (26.7%) cirrhotic females their mean age was 53.98±9.07 years.
Group II included 17(56.7%) males and 13(43.3%) females with liver cirrhosis and HCC, their mean age was 55.60±93.95 years.
The healthy control group included 6(60%) males and 4(40%) females with matched age, gender and body mass index (BMI), their mean age was 48.40±9.17 years.
Group I, 25 patients (55.6%) were bleeder; 32 patients (71.1%) had ascites, 16 patients (35.6%) presented with hepatic encephalopathy
Group II,13 patients (43.3%) were bleeder; 25 (83.3%) had ascites and 10 patients (33.3%) presented with hepatic encephalopathy with no significant difference between both groups.
Five patients (11.1%) of group I were hypertensive while 7 patients (23.3%) of group II were hypertensive and 4 patients (8.9%) of group I had IHD while 5 patients (16.7%) of group II had IHD.
In group I, 8 patients (17.8%) were of child class A, 27 patients (60.0%) were of child class B and 10 patients (22.2%) where of child class C. While in group II, 1patient (3.3%) was of child class A, 13 patients (43.3%) were of child class B and 16 patients (53.3%) where of child class C with significant difference between both groups (p=0.011*) ().
Table 1 Clinical data of patients groups
The mean value of child class score in group I was 8.58±1.90 while in group II, it was 9.63±1.83 with significant difference between the two groups (p=0.015*) ().
The mean value of MELD score in group I was 13.60±4.91while in group II it was 14.47±4.19 with no significant difference between both groups (p=0.235) ().
AST, ALT, direct bilirubin and total proteins levels were significantly higher in group II than group I (p=0.001*,0.001*, 0.026*, 0.021* respectively), while serum albumin level showed no significant difference between the two groups. Also GGT and ALP were significantly higher in group II than group I (p=0.043*, 0.041* respectively) ().
Table 2 Laboratory investigations in both patients groups.
No significant difference between both groups as regards HB level, WBC count, prothrombin activity and INR was found ().
Table 3 Haematological investigations in both patients groups
Platelates were significantly lower in group II than group I (P=0.036*).
APRI score was significantly higher in group II than group I with P value <0.001* ().
- AFP serum concentration was significantly higher in group II showing a median value of [462.0(22.7-10271)] ng/ml than in group I which showed median value of [10.30 (1.58- 63.90)] ng/ml with p3< 0.001*().
Table 4 AFP and serotonin concentration in control and patients groups
Also the serum concentration of AFP in both groups was significantly higher than control group which showed a median value of [5.10 (2-10)] ng/ml with [P1 <0.001*, P2<0.001*]().
The serum concentration of serotonin in group II was [478.35(266.60-1577.40)] ng/ml which was significantly higher than group I which showed a median value of [119.40(44.90 -337.40] ng/ml with P3< 0.001*, also serotonin serum concentration in both groups was significantly higher than control group which slowed a median value of [51.50(42.50-75) ng/ml]
[P1< 0.001*,P2<0.001*] ().
Serotonin serum concentration was significantly higher in child class C than child class B and A (P=0.023*) ().
Table 5 Relation between child class and serotonin in total patients
There was a significant positive correlation between serum serotonin concentration and AFP in group I and group II (r=0.298, p=0.047*, r=0.468, 0.009* respectively) ().
Table 6 Correlation between AFP and serotonin
Serotonin showed negative significant correlation with APRI score in group II (r=-0.363, p=0.049*), while in group I the negative correlation between serotonin and APRI score was not significant (r=-0.064, P=0.675) ().
Table 7 Correlation between serotonin and APRI
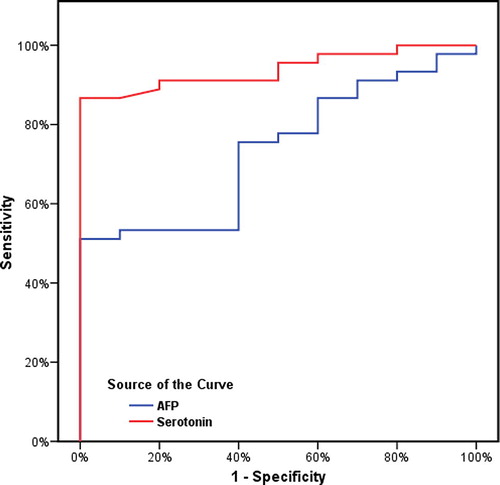
4.1 ROC curve
4.1.1 A; Group I: ()
* AFP area under ROC curve (AUROC) at cut off (10 ng/ml) was 0.733
P = 0.074 showing 51.11% sensitivity 100% PPV, 100% specificity, 31.25% NPV and 60% accuracy .
* Serotonin AUROC at cut off value of 75ng/ml was (0.939 P = 0.031) showed 86.67% sensitivity with‘ 100% specificity with‘ 62.50% NPV and 89.09% accuracy.
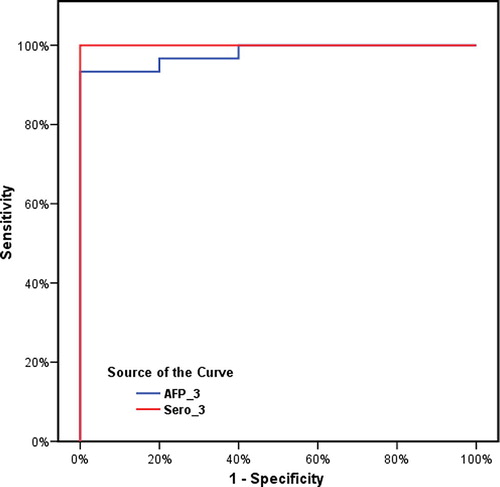
4.1.2 B; Group II: ()
AFP at cut off 10ng/ml the area under ROC curve was 0.980 P= 0.018 showing 93.33% sensitivity with 100% PPV and 100% specificity with 83.3% NPV and 95% accuracy .
Serotonin at cut off 75 ng/ml was 1.000 p< 0.001 showing 100% diagnostic performance.
5 Discussion
Hepatocellular carcinoma is the fifth leading cause of cancer and the third leading cause of cancer death.Citation49 This cancer varies widely in incidence throughout the world, with rising incidence in Egypt.Citation5,Citation8In general, almost all HCC cases are preceded by chronic hepatitis or liver cirrhosis which is mainly caused by hepatitis B and hepatitis C.Citation50 Despite the surveillance programs for high-risk patients, it is still a medical issue that many patients have an unresectable HCC at the time of diagnosis.Citation51
Ultrasound (US) screening is superior to AFP assay for detection of HCC but combined use of AFP monitoring and US is recommended in patients with chronic HCV.Citation52,Citation53
Serotonin (5HT), a well-known neurotransmitter within the central nervous system, also regulates a wide range of physiological actions in the gastrointestinal tract.Citation545HT is a potent mitogen for many different cell types, including hepatocytes.Citation55 Within the liver, 5HT has the ability to regulate hepatic blood flow at both the portal and sinusoidal levels and it may play a role in hepatic regeneration.Citation19 Serotonin has been shown to mediate the pathology of many liver diseases, such as steatohepatitis, chronic cholestasis, viral hepatitis and liver cirrhosis.Citation30,Citation35All these conditions are involved in the tumorgenesis of HCC.Citation56
After application of serotonin inhibitors, portal pressure is decreased in patients with liver cirrhosis, confirming the importance of serotonin in the pathogenesis of portal hypertension.Citation57 On the other hand, higher serotonin levels are associated with improved antiviral treatment outcomes in patients with HCV.Citation58 These findings make serotonin both friend and foe for the liverCitation59
AFP seems to be of prognostic value at the time of tumor diagnosis. A high concentration in HCC is associated with greater tumour size, bilobar involvement, portal vein invasion, and a lower median survival rate .Citation60
Farinati et alCitation61 concluded that AFP was not a sensitive marker to detect the presence of HCC. Also, the prognostic value of AFP is limited, but it is correlated with the overall survival in untreated patients.
Recent data suggest that the use of AFP as a diagnostic test is less specific than was once thought. Since it can be elevated in liver cirrhosis and other malignancies, it is recommended that it is no longer be used for diagnosis of HCC.Citation62In our work, serum AFP was significantly higher in patients than healthy subjects (P1=0.022*, P2<0.001*) also it was significantly higher in group II than group I (P3<0.001*), although it was higher than normal in some patients with liver cirrhosis without HCC ().
Baig et al.Citation63 concluded that AFP was a significant marker for HCC and also an indicator of HCC risks mostly in patients with cirrhosis and HCV/HBV infections .In study conducted in chinese patients with chronic hepatitis B, 44 patients were found to have an elevated AFP. Of these, only six had HCC.Citation64
In our work, plasma serotonin level was significantly higher in patients than healthy subjects (P1<0.001*,P2<0.001*) also it was significantly higher in group II than group I (P3<0.000*) ().
Serum serotonin concentration was significantly higher in child class C than child class A and B (P=0.023*) ().
Culafic et alCitation38 found a statistical significant difference between serotonin plasma values in patients with liver cirrhosis and healthy subjects, moreover they found that its level was significantly higher in Child-Pugh grade A/B than in grade C patients but platelets serotonin content was not significantly different between Child –Pugh grade C and grade A/B and concluded that plasma serotonin is a better marker of liver insufficiency than platelet serotonin content .
In this work, platelets serotonin was not measured and platelets count was low in both groups but was significantly lower in group II than group I (P=0.036*) ().
Marasini et alCitation65 described a significant reduction of serotonin in platelets of patients with liver cirrhosis, although level of plasma serotonin was within the normal range In the study of Beaudry et alCitation66, the whole blood serotonin level was significantly lower in patients with cirrhosis than in age matched controls, and no correlation was found between these levels and the severity of cirrhosis but the unconjugated plasma serotonin level, an indication of the active form of serotonin, was significantly higher in patients with cirrhosis than in the controls
Platelets are able to attract serotonin from the gut and lung. Serotonin is present in high concentration in platelets, where it accumulates from the plasma via the active transport system SERT. Thus, serotonin participates in
aggregation of platelets and coagulation of blood.Citation67 Operating as buffers, platelets maintain low levels of free circulating serotonin. As the carrier and reservoir, platelets store serotonin in dense electron granules.Citation68
Lesurtel et alCitation69identified platelets as the major source of serotonin that drives liver regeneration in partial hepatectomy (PHx) mice. They found that liver regeneration in thrombocytopenic mice following PHx was restored by supplementing the mice with platelet-rich plasma containing near weight levels of serotonin.
Laffi et alCitation32 gave evidence for significant reduction of substances that are deposited in thick and in alpha granules in patients with liver cirrhosis, a condition defined as “platelet exhaustion” .
Culafic et alCitation38 concluded that plasma serotonin was significantly higher in patients with cirrhosis than in the controls and represent the degree of liver insufficiency .It was noticed that liver regeneration and repair were significantly impaired in platelet-depleted animals. Mice lacking peripheral serotonin showed a failure of hepatocyte proliferation after ischaemia, but otherwise display
normal tissue remodeling. The results suggest that platelets may not cause postischaemic liver injury, but mediate tissue repair through modulation
of inflammation and release of serotonin.Citation31
APRI score was significantly higher in group II than group I (P<0.001*) also a significant negative correlation was found between serotonin level and APRI score in group II patients who had both higher serotonin and APRI score (r=-0.363, p=0.049*). Similar results obtained by Loftis JM et alCitation58 who demonstrated association between higher serotonin level and lower APRI score suggesting that higher serotonin levels might be a surrogate marker of less advanced liver disease.
The involvement of serotonin in the induction of hepatocyte DNA synthesis was first investigated in primary cultures of adult rat hepatocytes by Balasubramanian et alCitation70, which showed that 5-HT could significantly induce hepatocyte proliferation in the presence of insulin and EGF (epidermal growth factor) .
Among serotonin receptors 5-HT2B receptor has been strongly associated with increased hepatic stellate cells (HSCs) proliferation and liver fibrosis. HSCs have been reported to secrete numerous factors that influence hepatocyte proliferation. The role of serotonin as a mitogen for HSCs during liver regeneration remains hugely unknown.Citation30,Citation71
Serotonin signalling seems to play a pivotal role in determining the balance between regeneration and fibrogenesis in chronic liver disease and it has been reported that activation of 5-HT2B receptor on fibrogenic HSCs suppresses hepatocyte proliferation through augmented production of TGFβ1.Citation72 At the severe end of the spectrum, 5-HT has been involved in the pathogenesis of human HCC through increased 5-HT2B expression, which seems to facilitate the survival of carcinoma cells and to inhibit autophagy.Citation48It has also been reported to exert a proliferative effect on cholangiocytes and to promote cholangiocarcinoma growth.Citation73 There are also some interesting reports suggesting that serotonin can potentially contribute to liver tissue hypoperfusion following hepatic ischemia and reperfusion in canines raising new dilemmas about its effects on hepatic regenerationCitation19,Citation74
Serotonin can be potentially associated with either beneficial or detrimental effects on liver regeneration and these actions are mediated through many different receptor subtypes located either centrally or peripherally.Citation71
A significant positive correlation was found between serum serotonin and AFP in group I and group II (r=0.298, p=0.047*, r=0.468, 0.009* respectively) (), so higher AFP is associated with higher serotonin This signify the association between AFP and serotonin and so the importance of serum serotonin as marker of HCC and together with the results of ROC curve in both groups can consider serotonin as good marker for diagnosis of HCC.()
Table 8 Agreement (sensitivity, specificity and accuracy) for AFP and serotonin in liver Cirrhosis and HCC group.
6 Conclusion
Plasma serotonin levels are significantly higher in patients with cirrhosis& HCC than in cirrhosis than in the control groups and & involved in the tumorgenesis of hepatocellular carcinoma the third cause of cancer-related death worldwide.
Notes
Available online 19 April 2013
Peer review under responsibility of Alexandria University Faculty of Medicine.
References
- Surveillance, Epidemiology, and End Results (SEER) Program. SEER*Stat database: incidence — SEER 9 Regs research data, Nov 2009 Sub (1973–2007). Bethesda, MD: NATL CANCER I MONOGR, April 2010.
- El- Serag HB. Hepatocellular carcinoma. New Engl, J Med. 2011; 365:1118–27.
- G.T.StricklandH.ElhefniT.SalmanI.WakedM.Abdel-HamidN.N.MikhailRole of hepatitis C infection in chronic liver disease in EgyptAm J Trop Med Hyg.672002436442
- E.SzabóC.PáskaKaposi Novák P, Schaff Z, Kiss A. Similarities and differences in Hepatitis B and C Virus induced HepatocarcinogenesisPathol Oncol Res.12004511
- El-Zayadi AR, Badran HM, Barakat EM, Attia Mel-D, Shawky S, Mohamed MK, Selim O, Saeid A. Hepatocellular carcinoma in Egypt:a single center study over a decade. World J Gastroentero. 2005; 11: 5193–8.
- L.S.FreedmanB.K.EdwardsL.A.G.RiesJ.L.YoungCancer incidence in four member countries (Cyprus, Egypt, Israel, and Jordan) of the middle east cancer consortium (MECC) compared with US SEERNatl Cancer I Monogr. Bethesda MD: NIH Pub.2006 No. 06- 5873
- M.M.El GaafaryC.RekacewiczA.G.Abdel-RahmanM.F.AllamM.El HosseinyM.A.HamidSurveillance of acute hepatitis C in CairoEgypt. J Med Virol.762005520525
- E.M.LehmanM.L.WilsonEpidemiology of hepatitis virusesamong hepatocellular carcinoma cases and healthy people in Egypt: A systematic review and meta-analysisInt J Cancer.1242009690697
- G.M.El-NadyR.LingT.J.HarrisonGene expression in HCV asssociated hepatocellular carcinoma-upregulation of a gene encoding a protein related to the ubiquitin-conjugating enzymeLiver Int.232003329337
- G.FattovichProgression of hepatitis B and C to hepatocellular carcinoma in Western countriesHepato-gastroenterol.453199812061213
- A.I.GomaaS.A.KhanE.L.S.LeenI.WakedS.D.T.RobinsonDiagnosis of hepatocellular carcinomaWorld J Gastroentero.1511200913011314
- B.DanieleA.BencivengaA.S.MegnaV.TinessaAlpha-fetoprotein and ultrasonography screening for hepatocellular carcinomaGastroenterology.1272004S108S112
- A.V.FrancaJ.Elias JuniorB.L.LimaA.L.MartinelliF.J.CarrilhoDiagnosis, staging and treatment of hepatocellular carcinomaBraz J Med Biol Res.37200416891705
- Mehboob M, Butt K, Ahmed E, Wadood A, Khan JA, Pervez S. Fibrolamellar Hepatocellular Carcinoma - A rare clinical variant. Journal of Surgery Pakistan (International); January - March 2012 17 (1).
- F.FarinatiD.MarinoM.De GiorgioA.BaldanM.CantariniC.CursaroDiagnostic and prognostic role of alpha-fetoprotein in hepatocellular carcinoma: both or neither?Am J Gastroenterol.1012006524532
- Lamerz R, Hayes P, Hoffmann R-T, Lohe F, Shiratori Y, Taketa K. National academy of clinical biochemistry guidelines for the use of tumor markers in primary liver cancer. Practice Guidelines and Recommendations For Use Of Tumor Markers In The Clinic Liver Cancer (Section 3D).
- D.HoyerD.E.ClarkeJ.R.FozardP.R.HartigG.R.MartinE.J.MylecharaneInternational Union of Pharmacology classification of receptors for 5-hydroxytryptamine (Serotonin)Pharmacol Rev.461994157203
- M.D.GershonJ.TackThe serotonin signalling system: from basic understanding to drug development for functional GI disordersGastroenterology.1322007397414
- R.G.RuddelD.A.MannG.A.RammThe function of serotonin within the liverJ Hepatol.482008666675
- M.LesurtelC.SollR.GrafP.A.ClavienRole of serotonin in the hepato-gastrointestinal tract: an old molecule for new perspectivesCell Mol Life Sci.6562008940952
- C.P.MercadoF.KilicMolecular mechanisms of SERT in platelets: regulation of plasma serotonin levelsMol Interv.1042010231241
- D.J.AngiolilloM.UenoS.GotoBasic principles of platelet biology and clinical implicationsCirc J.742010597607
- J.R.RaymondY.V.MukhinA.GelascoJ.TurnerG.CollinsworthT.W.GettysMultiplicity of mechanisms of serotonin receptor signal transductionPharmacol Therapeut.922001179212
- S.A.CummingsR.J.GroszmannA.J.KaumannHypersensitivity of mesenteric veins to 5-hydroxytryptamine- and ketanserin-induced reduction of portal pressure in portal hypertensive ratsBrit J Clin Pharmaco891986501513
- R.MastaiB.RocheleauP.M.HuetSerotonin blockade in conscious, unrestrained cirrhotic dogs with portal hypertensionHepatology.91989265268
- M.ĐorđeS.DuškoD.MiodragS.JelenaPlasma and platelet serotonin levels in patients with liver cirrhosisWorld J Gastroentero.1343200757505753
- A.MabuchiI.MullaneyP.W.SheardP.A.HessianB.L.MallardM.N.TawadrousRole of hepatic stellate cell/hepatocyte interaction and activation of hepatic stellate cells in the early phase of liver regeneration in the ratJ Hepatol.402004910916
- Brauneis U, Gatmaitan Z, Arias IM. Serotonin stimulates a Ca2+ permeant nonspecific cation channel in hepatic endothelial cells. Biochem Bioph Res Co.1992; 186:1560–6.
- Z.GatmaitanL.VarticovskiL.LingR.MikkelsenA.M.SteffanI.M.AriasStudies on fenestral contraction in rat liver endothelial cells in cultureAm J Clin Pathol.148199620272041
- R.G.RuddellF.OakleyZ.HussainI.YeungL.J.Bryan-LlukaG.A.RammA role for serotonin (5-HT) in hepatic stellate cell function and liver fibrosisAm J Clin Pathol.1692006861876
- A.NocitoP.GeorgievF.DahmW.JochumM.BaderR.GrafPlatelets and platelet-derived serotonin promote tissue repair after normothermic hepatic ischemia in miceHepatology.452007369376
- G.LaffiF.MarraP.GreseleP.RomagnoliA.PalermoO.BartoliniEvidence for a storage pool defect in platelets from cirrhotic patients with defective aggregationGastroenterology.1031992641646
- H.ItohC.CicalaG.J.DouglasC.P.PagePlatelet accumulation induced by bacterial endotoxin in ratsThromb Res.831996405419
- L.AmitranoM.A.GuardascioneV.BrancaccioA.BalzanoCoagulation disorders in liver diseaseSemin Liver Dis.2220028396
- A.NocitoF.DahmW.JochumJ.H.JangP.GeorgievM.BaderSerotonin mediates oxidative stress and mitochondrial toxicity in a murine model of nonalcoholic steatohepatitisGastroenterology.1332007608618
- P.A.LangC.ContaldoP.GeorgievA.M.El-BadryM.RecherM.KurrerAggravation of viral hepatitis by platelet-derived serotoninNat Med.142008756761
- A.NocitoF.DahmW.JochumJ.H.JangP.GeorgievM.BaderSerotonin regulates macrophage-mediated angiogenesis in a mouse model of colon cancer allograftsCancer Res.68200851525158
- D.M.CulaficD.S.MirkovicM.D.VukcevicJ.S.RudicPlasma and platelet serotonin levels in patients with liver cirrhosisWorld J Gastroentero.1343200757505753
- G.BedogniL.MiglioliF.MasuttiC.TiribelliG.MarchesiniS.BellentaniPrevalence of and risk factors for nonalcoholic fatty liver disease: The Dionysos nutrition and liver studyHepatology.42120054452
- Burtis CA, Ashwood ER, BrunsDE. Tietz Textbook of Clinical Chemistry and Molecular Diagnostics. Elsevier Saunders Company St Louis.2008, 604-14.
- Lewis SM, Brain BJ, Bates I. Dacie and Lewis practical Hematology. 10 th ed.Churchil livingstone Elsevier, Philadelphia. 2006, 40–57, 465–79.
- F.C.KrugerC.R.DanielsM.KiddG.SwartK.BrundynC.Van RensburgAPRI: A simple bedside marker for advanced fibrosis that can avoid liver biopsy in patients with NAFLD/NASHS Afr Med J.1012011477480
- H.L.ChanWongVW, Tes AM l. serum hepatitis B surface antigen quantitation can reflect hepatitis B virus in the liver and predict treatment responseClin Gastroenterol.512200714621468
- K.MasayukiT.YasuhitoN.NaoS.NaoyaPre-treatment prediction of response to pegylated-interferon plus ribavirin for chronic hepatitis C using genetic polymorphism in IL28B and viral factorsHepatology.542011439448
- I.LevyM.ShermanStaging of hepatocellular carcinoma: assessment of the CLIP, Okuda and Child-Pugh staging systems in a cohort of 257 patients in TorontoGut.502002881950
- L.GheorgheS.IacobR.IacobC.GheorgheI.PopescuVariation of the MELD Score as a Predictor of Death on the Waiting List for Liver TransplantationJ Gastrointest Liver.1632007267272
- T.C.PoonT.S.MokA.T.ChanQuantification and utility of monosialylated alpha-fetoprotein in the diagnosis of hepatocellular carcinoma with nondiagnostic serum total alpha-fetoproteinClin Chem Lab Med.48200210211027
- C.SollJ.H.JangM.RienerW.MoritzP.J.WildR.GrafSerotonin promotes tumor growth in human hepatocellular cancerHepatology.514201012441254
- F.X.BoschJ.RibesR.CleriesM.DiazEpidemiology of hepatocellular carcinomaClin Liver Dis.92005191211
- H.El-SeragK.RudolphHepatocellular carcinoma: epidemiology and molecular carcinogenesisGastroenterology.132200725572576
- S.K.YoonRecent advances in tumor markers of human hepatocellular carcinomaINT VER.51suppl 120083441
- G.LarcosH.SorokopudG.BerryG.C.FarrellSonographic screening for hepatocellular carcinoma in patients with chronic hepatitis or cirrhosis: an evaluationAm J Roentgenol.17121998433435
- K.A.GeboG.ChanderM.W.JenckesK.G.GhanemH.F.HerlongM.S.TorbensonScreening tests for hepatocellular carcinoma in patients with chronic hepatitis C: a systematic reviewHepatology.362002S84S92 (5 Suppl1)
- W.NiS.W.Watts5-Hydroxytryptamine in the cardiovascular system: Focus on the serotonin transporter (SERT)Clinical and Experimental Pharmacology and Physiology.332006575583
- B.L.FanburgS.L.LeeA new role for an old molecule: serotonin as a mitogenAm J Physiol.2721997795806
- D.SchuppanN.H.AfdhalLiver cirrhosisLancet.3712008838851
- J.VorobioffG.Garcia-TsaoR.GroszmannG.AcevesE.PicabeaR.VillavicencioLong term hemodynamic effects of ketanserin, a 5-hydroxytryptamine blocker, in portal hypertensive patientsHepatology.919898891
- J.M.LoftisB.J.MorascoD.MenascoD.FuchsM.StraterP.HauserSerum serotonin levels are associated with antiviral therapy outcomes in patients with chronic hepatitis CThe Open Infectous J.42010132141
- M.LesurtelC.SollB.HumarP.A.ClavienSerotonin: A double edged sword for the liverSurgeon.1022012107113
- A.S.LokLai CL. alpha-Fetoprotein monitoring in Chinese patients with chronic hepatitis B virus infection: role in the early detection of hepatocellular carcinomaHepatology.91989110115
- F.FarinatiD.MarinoM.De GiorgioA.BaldanM.CantariniC.CursaroDiagnostic and prognostic role of alpha-fetoprotein in hepatocellular carcinoma: both or neither?Am J Gastroenterol.1012006524532
- F.GrizziB.FranceschiniC.HamrickE.E.FrezzaE.CobosM.Chiriva-InternatiUsefulness of cancer-testis antigens as biomarkers for the diagnosis and treatment of hepatocellular carcinomaJ Transl Med.520073
- J.A.BaigJ.M.AlamS.R.MahmoodM.BaigR.ShaheenI.SultanaHepatocellular carcinoma (HCC) and diagnostic significance of α – fetoprotein (AFP)J Ayub Med Coll Abbottabad.21120097275
- J.BruixM.ShermanAASLD practice guidline. Management of hepatocellular carcinoma: an updateHepatology.5332011135
- B.MarasiniM.L.BiondiA.AgostoniPlatelet and plasma serotonin in patients with liver cirrhosisJ Clin Chem Lab Med.271989419421
- P.BeaudryA.HadengueJ.CallebertC.GaudinH.SolimanR.MoreauBlood and plasma 5-hydroxytryptamine levels in patients with cirrhosisHepatology.201994800803
- P.A.ClavinLiver regeneration: a spotlight on the novel role of platelets and serotoninSwiss Med Wkly.13825–262008361370
- A.E.LinderW.NiJ.L.DiazT.SzaszR.BurnettS.W.WattsSerotonin(5-HT) in veins: not all in vainJ Pharmacol Therapeut.3232007415421
- M.LesurtelR.GrafB.AleilD.J.WaltherY.TianW.JochumPlatelet-derived serotonin mediates liver regenerationScience.3122006104107
- S.BalasubramanianC.S.PauloseInduction of DNA synthesis in primary cultures of rat hepatocytes by serotonin: possible involvement of serotonin S2 receptorHepatology.2719986266
- G.K.PapadimasK.N.TzirogiannisM.G.MykoniatisA.D.GrypiotiG.A.MantaG.I.PanoutsopoulosThe emerging role of serotonin in liver regenerationSwiss Med Wkly.1422012135148
- M.R.EbrahimkhaniF.OakleyL.B.MurphyJ.MannA.MolesM.J.PerugorriaStimulating healthy tissue regeneration by targeting the 5-HT2B receptor in chronic liver diseaseNatl Med J India.17201116681673
- G.A.FramptonH.LiJ.RamirezA.MohamadS.De MorrowBiogenic amines serotonin and dopamine regulate cholangiocyte hyperplastic and neoplastic growthWorld J Gastrointest Pathophysiol.15220106368
- R.MurataN.HamadaN.NakamuraA.KobayashiM.FukuedaA.TairaSerotonin activity and liver dysfunction following hepatic ischemia and reperfusionIn Vivo.172003567572