Abstract
Positron emission tomography computed tomography (PET-CT) is a combined functional and structural multi modality imaging tool that can be utilized to detect vulnerable and atherosclerotic plaques. In this study we observe the prevalence of active and calcified plaques in selected arteries during whole-body 18F-FDG PET-CT and correlate the findings with risk factors in developing coronary artery disease. There was a significant relationship between patients with high body mass index and vulnerable plaques. We concluded that 18F-FDG PET-CT can be utilized in detecting focal high FDG uptake within vascular plaque in early recognition of high risk patients having vascular accidents.
1 Introduction
Ischaemic heart disease and cerebrovascular accidents are the leading cause of death in many countries in the world.Citation1 Despite major advances in the prevention and treatment of vascular diseases, they remain to be the worldwide leading cause of morbidity, mortality and sudden death. Vascular events have been thought to be caused by sudden rupture of a vascular plaque, resulting in either thrombosis at the site of rupture or distal embolization into smaller arteries resulting in reduced blood supply or total occlusion.Citation2 Histologically, cross sectional atheromatous plaque reveals layers of fatty deposits in the intima of an artery. This abnormal accumulation of fats alters the inner lining of arterial lumen leading to constriction and over time, obstruction to blood flow. Atheromatous plaque can be inflamed, detached from its origin and thrombosed smaller arteries thus defined as ‘vulnerable plagues’. There has been a strong association of vulnerable plaques with sedentary and stressful lifestyle, smokers and those with high risks of vascular events.Citation3 Various imaging modalities have been used in the clinical investigation of vascular plaque including ultrasonography, Magnetic Resonance Imaging (MRI) and Multi Detector Computed Tomography (MDCT). However, the ability of these modalities in identifying vulnerable plaques is very limited. On the other hand, Optical Coherence Tomography (OCT) and Intra Vascular Ultra Sound (IVUS) are more invasive. In this study, we investigated the prevalence of inflamed vascular plaque in selected medium and large size arteries and correlate the findings in our patients with risk factors in developing coronary artery disease using 18-fluorine fluorodeoxyglucose as a marker in non invasive integrated dual imaging modality PET-CT.
2 Materials and methods
This study was conducted with the approval of local ethics committee.
2.1 Patient selection
Thirty oncology patients referred for staging at diagnosis were included in this retrospective study. All patients underwent whole body FDG PET-CT study between April 2010 and September 2011 at the centre for Diagnostic Nuclear Imaging of Universiti Putra Malaysia. We include the data from 30 adult patients in our analysis. Past and present clinical history of high risk factors in developing cardiovascular events was obtained from all patients via prospective telephone interview. All PET-CT imaging studies were performed following standard protocol. All patients were required to be fasted for at least 6 h before the study. In the morning of the study, fasting blood glucose level was measured followed by intravenous tracer injection of 8–10 mCi of 18F-FDG. The patients were put to rest in a confinement room with an uptake time of approximately 60 min before imaging. Patients’ characteristics are tabulated ().
Table 1 Descriptive patient characteristics (n = 30).
2.2 Imaging technique
Studies were standardized using a dedicated integrated PET-CT system (Siemens Truepoint Biograph – TrueV®). This device comprises of a dedicated PET scanner with Optimum Performance in 3-D Imaging with Lutetium Oxyorthosilicate (LSO) scintillator crystal technology, which provides fast coincidence timing, efficient rejection of random events, high light output and high count rates. The camera widens the axial field of view by 33%, which increases count rate performance by 70%, better than older scan generation in which shorter acquisition time can be performed. The system is incorporated with a multislice CT scanner with capability for 64 slice CT and high spatial resolution. In view of the higher sensitivity of this system, the acquisition time for PET was 2 min per table position. CT data were re-sized from a 512 × 512 matrix to a 128 × 128 matrix to match the PET data to allow image fusion and generation of CT transmission maps. PET images were reconstructed using ordered-subsets expected maximization (OSEM) with segmented measurement of attenuation correction using CT data with four iterations and 16 subsets. Post reconstruction smoothing of images was performed using a 5 mm FWHM Gaussian filter. PET and CT images were then fused, creating an image of distributed 18F-FDG overlying the corresponding anatomy and physiology generated using a dedicated workstation.
2.3 Image analysis
The images were reviewed systematically. The maximum intensity projection (MIP) was first analysed for adequacy of FDG uptake intensity. The distribution was threshold with the highest activity within the bladder and or renal excretion. Several sites were selected including bilateral carotids, ascending, arch and descending aorta, the abdominal aorta at supra and infra renal locations and the iliac arteries. Reconstructed images were reviewed in trans axial, coronal and sagittal planes. The images were reviewed using CT looking for morphological changes in the wall of the arteries and PET looking for focal increase in 18F-FDG uptake. Focal changes detectable in any of the modalities were analysed in detail. In axial images, two lines in x and y-axis, perpendicular to each other were drawn crossing the central lumen of the artery. On co registered PET-CT slices, 1 cm simple circular regions of interest (ROIs) were placed so as to cover the four sites that had been chosen as control that is divided into four quadrants (2 o’clock, 4 o’clock, 8 o’clock and 10 o’clock) in each carotid, thoracic aorta, abdominal aorta and iliac arterial walls and lumen (). The sites chosen are used to differentiate between ‘lesion’ and ‘control’ areas (). On each slice, the mean and maximum standardized uptake values (SUV) of 18F-FDG derived from the ROI were calculated as the mean and maximum pixel activity that is used to detect inflamed vascular wall (). While CT images were analysed by observing corresponding calcifications and calculating the CT value in Hounsfield unit (HU). The relationship between plaque composition by means of CT value correlating calcium content and raised metabolic activity by means of maximum Standardized Uptake Value (SUVmax) at various sites of arterial walls were obtained and tabulated (). Computer generated SUVmax was obtained using gross body weight. Comparing the mean physiological uptake within the liver and blood pool, the value between second and third quartile is consider as significant activity ranging between 1.7 and 1.9.
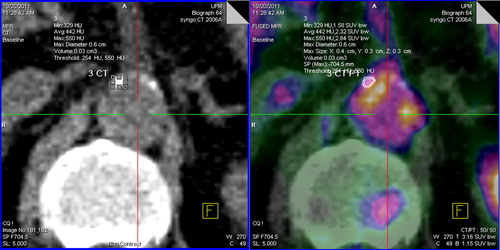
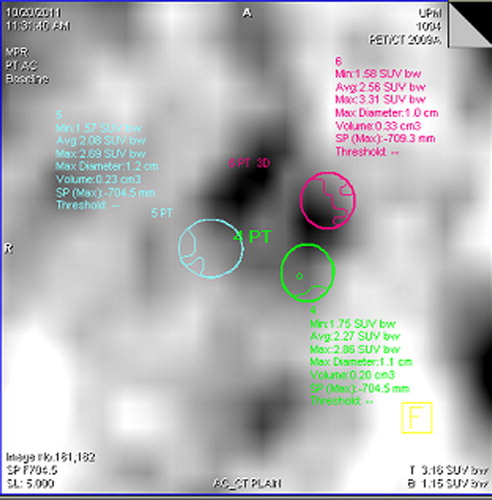
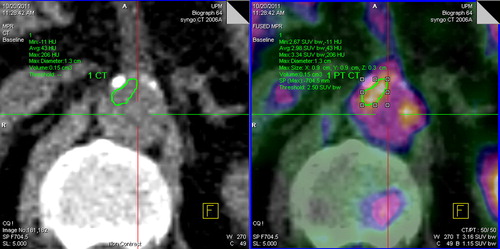
Table 3 The relationship of plaque area (HUmax) and risk factors in developing vulnerable plaque by using independent t test for variable <2 group and ANOVA test for variable >2 group.
2.4 Statistic analysis
Univariate descriptive analysis was carried out to the presence of vascular wall activity (SUV) and calcified artery (HU) in the socio-demographic characteristics (including gender, age group, and body mass index (BMI), ethnic group, smoking status, hypertension, diabetes mellitus and relevant family history. Categorical data described using frequency and percentages. Numerical data described using means and standard deviation depending on distribution of respective variables (). Risk factors (age, BMI, ethnic, gender, smoking status, hypertension, diabetes mellitus, hyperlipidemia and relevant family history) were correlated with SUV using either independent t-test or ANOVA. The variable of HU was not normally distributed (left skewed). Therefore, the logarithmic transformations were performed for HU before data analyses. Pearson’s-r were used to test correlation between calcified artery (in HU) and metabolic activity (expressed in SUVmax) in inflamed vascular wall. All data analyses were performed using statistical Package for Sciences (SPSS) version 19 where p-values below 0.05 are considered as a significant finding.
Table 2 The relationship between SUVmax and HUmax, with patient demographics and risk factors by using an independent t-test for < 2 variables and ANOVA for > 2 variables.
3 Theory
Functional imaging modality Positron Emission Tomography (PET) using Fluorodeoxyglucose (FDG) as biotracer is known to improve the accuracy of many oncology diagnoses. Being an analogue of glucose, FDG is phosphorylated by glucose-6-phosphate dehydrogenase during glycolysis process at a rate directly related to tumour aggressiveness. This principle of FDG metabolism in malignant tumour is applicable in imaging inflammatory conditions and infection albeit lower intensity of FDG uptake is expected comparing to malignancy during PET imaging study like in the case of vulnerable plaque imaging. The combination of PET and CT in a single instrument enables the exact anatomical assignment of focally increased 18F-FDG uptake to a specific region which also allows the detection and quantification of vascular calcifications.Citation4 Early localization of vulnerable plaques by means of functional metabolic imaging using FDG can facilitate early interventions preventing possible near future vascular events.Citation5
4 Results
4.1 Patient characteristics
The mean age of patients in our study is 51.67 ± 16.5 year with male predominant (63.3%). Most of our patients are Chinese ethnic followed by Malays and Indian with 3:2:1 ratio. One third of our patients fall under overweight category (BMI 29.99 kg/m2) while the majority are within normal weight range (53.3%). Majority of our patients are within high risk group (73.3%) where more than half have multiple risks in developing cardiovascular disease (53.3%) in comparison to single risk group (20%). One third are smokers while the remaining two thirds are non smokers. Of the 30 patients, none of them had any past history of cardiac events, two died from their oncology disease.
4.2 Relationship between SUVmax and HUmax with cardiovascular risk factors
There is a significant relationship between calcified plaque area (HU > 150) and risk of cardiovascular disease which includes male gender, older age group, high body mass index, hypertension, hyperlipidemia and family history of hypertension and diabetes mellitus. In addition, we also found a direct correlation between high SUVBW and body mass index of patients. We observed majority of Chinese having the highest prevalence of calcified plaque while Indians having the highest uptake of 18F-FDG. Overall, the uptake of FDG in vascular wall is found to be higher in male gender, obese, younger age group, smoker and history of diabetes mellitus and heart disease.
Plaque characterization is tabulated in . Majority of hard plaque formation is evident within the wall of aortic arch (674.5 ± 399.3 HU), right (593.71 ± 381.4 HU) and left (551.1 ± 384.25 HU) iliac arteries with CT value >150 HU.
The highest range of SUVmax found in association with plaque formation of vascular wall falls within the second and third quartile ranging between 1.67 ± 0.30 and 1.99 ± 0.11.
4.3 Relationship between SUVmax and HUmax
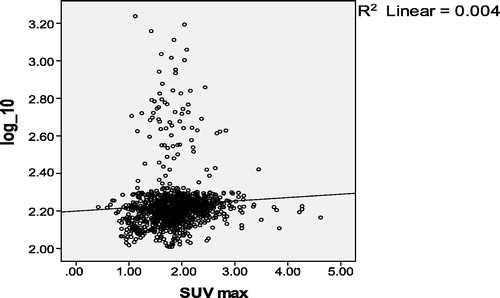
The correlation between calcified plaque and FDG uptake is significant (p < 0.05) with moderate Pearson correlation of 0.6 at 95% confident interval (95% CI). The mean CT value is 2.23 ± 0.15 (log10 HU) and mean SUVmax is 1.87 ± 0.50 in the majority of studied lesions. The correlation between calcified plaque (log10HU) and FDG uptake (SUVmax) is significant (p <0.05) with moderate correlation strength (r = 0.6). The mean CT value is 2.23 ± 0.15 (log10 HU) and mean SUVmax is 1.87 ± 0.50 in the majority of studied lesions. Guildford’s rule of thumb for interpreting degree, size, strength or magnitude of relationship is divided into five strengths which are as follows:
r = 0.0–0.29 Little or negligible relationship.
r = 0.3–0.49 Low relationship.
r = 0.5–0.69 Moderate or marked relationship.
r = 0.7–0.89 Strong relationship.
r = 0.9–1.0 Very strong relationship.
Our patients demonstrate no co-relationship between calcified plaque and metabolic activity where at 95% confident interval, the R square value is 0.004 .
5 Discussion
Our study found that 18F-FDG can be used to detect vulnerable plaques. The maximum SUVBW intensity greater than 1.8 can be utilized as the cut-off value in stratifying patients at our centre having risk of thrombo-emboli complications.
In recent years, atherosclerotic disease has become a recognized contributor towards worldwide causes of death from cardiovascular and stroke diseases.Citation6–Citation13
The mean SUVmax of FDG uptake within vascular plaque in our study within the majority of studied lesions is 1.87 ± 0.50. This value falls between the second and third quartile ranging between 1.67 ± 0.30 and 1.99 ± 0.11. In our set-up this value is above the average value of physiological FDG uptake within the liver, spleen and background activity. Considering the standardized protocol in performing whole body PET-CT study at our centre including the PET-CT system, uptake time and imaging protocol, we suggest this value as our reference point for future vulnerable plaque imaging studies, thus patients who demonstrate high 18F-FDG uptake at imaging may benefit further investigation screening for risk of cardiovascular disease.
In the study conducted by Vallabojosula et al.Citation14 they found that the site of aortic FDG uptake correlated well with the site of calcification. Based on the pathology of calcified and non calcified atheromas, it is not surprising that there was little overlap between the inflammatory and calcification: Correlation between sites of aortic calcification and foci of FDG uptake was observed in 7% of patients in one series and in less than 2% of patients in other series. While Rudd et al.Citation15 recently demonstrated that 18F-FDG uptake was higher in symptomatic lesion. These observations strongly suggest that 18F-FDG-PET is capable of imaging quantifying plaque inflammation.Citation16–Citation18 Our study found a linear relationship between calcified atheromatous plaque and high FDG uptake. In addition, we found high FDG uptake within atheromatous plaques in high risk group of patients including male gender, obese, smoker and those with history of diabetes mellitus and past coronary artery disease. This group of patients also demonstrate a significant high incidence of calcified plaque formation (p = 0.001).
In this study, we highlight the potential of PET-CT, a non invasive modality in imaging vulnerable and thrombotic plaques using 18F-FDG as marker in high risk groups. 18F FDG PET-CT was serially performed to investigate whether there is correlation between vascular 18F-FDG uptake and risk factor to develop atherosclerosis. The increased 18F-FDG uptake and calcified vascular wall were most strongly correlated with obese patients with BMI (30.00–34.99). Tahara et al. found significant correlations between BMI and male genderCitation16,Citation17which is in agreement with our study. A few potential limitations may impair the data analysis of this study. Moreover, most of the FDG uptake sites were not accompanied by calcification, each FDG sites were separated from the nearest calcification site which may have been caused by inaccurate integration of PET and CT images due to movement or respiratory motion from the patient Citation19–Citation21. Besides that, the subject of the study is limited. Current technology hampers PET camera ability to detect metabolic activity smaller than the camera’s resolution.Citation22–Citation25 In our setting the limitation is 4 mm dimension. In this observatory study, there are no methods to validate the FDG uptake of vascular plaques. Other factors which may induce 18F-FDG uptake should also be considered. Validation is required to established the relationship between high 18F-FDG vascular plague activity and vulnerability for vascular accidents. Its co-relationship with plasma concentration of established inflammatory parameters and endarterectomy findings require further investigations. The hypothesis that some foci of increased vascular-wall 18F-FDG uptake may correspond to early atherosclerosis and may indicate the presence of a ‘vulnerable’ plaque needs to be further tested by prospective studies and also continue following-up patients to find the outcome events and survival analysis, so that 18F-FDG PET-CT may be the tool for early detection of patients at increased risk of future cardiovascular events and for assessment of early therapies for vascular-wall lesions.
6 Conclusion
There is a role for 18F-FDG PET-CT as a non invasive tool in detecting vulnerable plaques. This combined imaging modality can stratify high risk patient in developing thrombo-embolic vascular diseases. Thus early clinical intervention can be instituted to prevent cardiovascular or cerebro-vascular events.
Acknowledgment
This work was supported by Research University Grant Scheme of Universiti Putra Malaysia.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 22 July 2013
References
- K.Geok LinPhdCardiovascular epidemiology in the Asia-Pacific region Asia PacificJ Clin Nutr1020017680
- B.PaulmierM.DuetR.KhayatN.Pierquet-GhazzarJ.P.LaissyC.MaunouryArterial wall uptake of fluorodeoxyglucose on PET imaging in stable cancer disease patients indicates higher risk for cardiovascular eventsJ Nucl Cardiol152008209217
- P.MorenoK.R.PurushothamanV.FusterD.EchverriH.TruszcynskaS.K.SharmaPlaque neovascularization is increased in ruptured atherosclerotic lesions of human aorta: Implication for plaque vulnerabilityJ Circ110200420322038
- S.Ben-HaimE.KupzovA.TamirO.IsraelEvaluation of 18F-FDG uptake and arterial wall calcifications using 18F-FDG PET/CTJ Nucl Med4511200418161821
- R.AxelS.TobiasW.SarahC.C.ClemensS.MichaelF.Stefan18F-FDG PET/CT identifies patients at risk for future vascular events in an otherwise asymptomatic cohort with neoplastic diseaseJ Nucl Med50200916111620
- World Health Organization. Cardiovascular diseases fact sheet. <http://www.who.int/mediacentre/factsheets/fs317/en/print.html [accessed 17.08.09].
- American Heart Association. Heart disease and stroke statistics. <http://www.americanheart.org/presenter.jhtml [accessed 17.08.09].
- S.WilliamD.MarkT.NaokiM.CarinaPET and PET-CT imaging in the diagnosis and characterization of atheromaJ Nucl Med1264200495104
- A.H.KaimB.WeberM.O.KurrerJ.GottschalkG.K.Von SchulthessA.BuckAutoradiographic quantification of 18F-FDG uptake in experimental soft-tissue abscesses in ratsJ Radiol22322002446451
- G.G.BuralD.A.TorigianW.ChamroonratM.HouseniW.ChenS.BasuFDG-PET is an effective imaging modality to detect and quantify age-related atherosclerosis in large arteriesEur J Nucl Med Mol Imaging352008562569
- S.VallabhajosulaV.FusterAtherosclerosis: imaging techniques and the evolving role of nuclear medicineJ Nucl Med38199717881796
- A.MasanoriS.SeigoC.H.ChristopherJ.V.SamiR.ElenaF.YoshihiroLipid lowering reduces oxidative stress and endothelial cell activation in rabbit atheromaJ Circ106200213901396
- R.J.LedermanR.R.RaylmanS.J.FisherP.V.KisonH.SanE.G.NabelDetection of atherosclerosis using a novel positron-sensitive probe and 18-fluorodeoxyglucose (FDG)J Nucl Med Commun222001747753
- S.VallabhajosulaJ.MachacK.KnesaurekImaging atherosclerotic macrophage density by positron emission tomography using F-18 fluorodeoxyglucose (FDG)J Nucl Med37199638
- J.H.RuddE.A.WarburtonT.D.FryerH.A.JonesJ.C.ClarkN.AntounImaging atherosclerotic plaque inflammation with 18F-fluorodeoxyglucose positron emission tomographyJ Circ105200227082711
- M.P.DunphyA.FreimanS.M.LarsonH.W.StraussAssociation of vascular 18F-FDG uptake with vascular calcificationJ Nucl Med468200512781284
- M.TatsumiC.CohadeY.NakamotoR.L.WahlFluorodeoxyglucose uptake in the aortic wall at PET/CT: possible finding for active atherosclerosisJ Radiol2292003831837
- S.Ben-HaimMD, DScElaKupzovPhDElaTamirDScOraIsraelMDEvaluation of 18F-FDG uptake and arterial wall calcifications using 18F-FDG PET/CTJ Nucl Med4511200418161821
- N.TaharaH.KaiS.YamagishiM.MizoguchiH.NakauraM.IshibashiVascular inflammation evaluated by [18F]-fluorodeoxyglucose positron emission tomography is associated with the metabolic syndromeJ Am Coll Cardiol4914200715331590
- N.TaharaH.KaiM.IshibashiH.NakauraH.KaidaK.BabaSimvastatin attenuates plaque inflammation: evaluation by fluorodeoxyglucose positron emission tomographyJ Am Coll Cardiol489200618251831
- W.TongH.LaiC.YangS.RenS.DaiS.LaiAge, gender and metabolic syndrome-related coronary heart disease in U.S. adultsInt J Cardiol1042005288291
- M.YunS.JangA.CucchiaraA.B.NewbergA.Alavi18F-FDG uptake in large arteries:a correlation study with the atherogenic risk factorsSemin Nucl Med32120027076
- M.YunD.YehL.I.ArauchoS.JangA.NewbergAlaviF-18 FDG uptake in the large arteries, a new observationClin Nucl Med2642001314319
- J.H.RuddK.S.MyersS.BansilalJ.MachacC.A.PintoC.TongAtherosclerosis inflammation imaging with 18F-FDG PET: carotid, iliac and femoral uptake reproducibility, quantification methods, and recommendationsJ Nucl Med4962008871878
- Andreas K.BuckMDSven N.ReskeMDCellular origin and molecular mechanisms of 18F-FDG uptake: is there a contribution of the endothelium?J Nucl Med4532004461463