
Abstract
Introduction
Multiple surgical approaches have been described to access the infratemporal fossa. One of them is the endoscopic endonasal transpterygoid approach to the infratemporal fossa. The endoscopic endonasal transpterygoid approach is considered the best to access the midline structures such as the nasopharynx, Eustachian tube, sella, and clivus. Through this work, we try to describe the anatomical structures and landmarks of the infratemporal fossa from the endosopic endonasal transpterygoid point of view.
Methods
A cadaveric study was performed on five adult specimens. Endoscopic medial maxillectomy and complete resection of the posterior wall of the maxillary antrum were performed. Extension of the medial maxillectomy anteriorly was done to reach the lateral part of the infratemporal fossa. Endoscopic Denker’s or Sturman–Canfield approach was done. Dissection of the pterygopalatine fossa was done with identification of maxillary artery branches, V2 (maxillary nerve) and masticatory muscles. Resection of the lateral pterygoid muscle and drilling the lateral pterygoid plate improve exposure of the infratemporal fossa, including V3 (mandibular nerve), which lies posterior to the lateral pterygoid plate.
Results
A total of ten infratemporal and pterygopalatine fossae (five cadaveric specimens) were dissected endoscopically using a transpterygoid approach. Dissection of different anatomical structures in the infratemporal fossa was done to describe the anatomical structures and landmarks of the infratemporal fossa.
Conclusions
Endoscopic endonasal transpterygoid approach is considered one of the most useful surgical solutions to manage selected tumors that involve the infratemporal fossa. A good understanding of the endoscopic anatomy of infratemporal fossa allows safe and complete resection of lesions arising or extending to infratemporal fossa.
1 Introduction
The infratemporal fossa is present below the middle cranial fossa floor, posterior to the maxillary sinus, medial to the ramus of the mandible, and lateral to the nasopharynx. The infratemporal surface of the greater wing of the sphenoid bone forms its roof. The lateral pterygoid plate forms its medial wall. The insertion of temporalis muscle into the coronoid process, the mandibular ramus and condylar process of mandible constitute the lateral boundary of the infratemporal fossa.Citation1–Citation3
The infratemporal fossa contains the lateral and medial pterygoid muscles, and important neurovascular structures, such as the mandibular nerve (V3) and the internal maxillary artery. Caudally, the infratemporal fossa is occupied by the medial pterygoid muscle, that inserts into the angle of mandible. Posteromedially, the infratemporal fossa contains the carotid sheath (internal carotid artery [ICA], internal jugular vein, and cranial nerves IX–XII) in the poststyloid part of parapharyngeal space.Citation1–Citation3 Other contents of the infratemporal fossa include the pterygoid venous plexus, maxillary vein, and the branches of mandibular nerve and chorda tympani nerves. Medially, the infratemporal fossa communicates with the pterygopalatine fossa via the pterygomaxillary fissure.Citation2,Citation3
Multiple surgical approaches to the infratemporal fossa have been described including lateral preauricular and postauricular approaches, anterior trans-maxillary, and inferior transmandibular approaches.Citation3 Anterior surgical approaches to the infratemporal fossa include the sublabial transmaxillary approach, Le Fort osteotomies, maxillary swing, and facial translocation.Citation4 Endoscopic endonasal transpterygoid approaches have been described to manage multiple pathologies in the paramedian and lateral skull base.Citation5
Endoscopic endonasal transpterygoid approaches were first described to access the lateral recess of the sphenoid sinus and was then expanded to manage lesions of the middle cranial fossa and infratemporal fossa.Citation5–Citation7 Understanding the anatomic landmarks of the infratemporal fossa from the endoscopic view is important before doing the endoscopic endonasal transpterygoid approaches.Citation8–Citation10
In this work, we studied the anatomy of the infratemporal fossa from the endoscopic view through applying the endoscopic endonasal transpterygoid approach.
2 Materials and methods
We studied five human anatomic specimens, dissecting the infratemporal fossa and pterygopalatine fossa bilaterally, in accordance with institutional protocols. Using a standardized method, all specimens were injected with red and blue silicone, through the internal carotid artery and internal jugular vein, respectively.
Visualization was facilitated by the use 0°, 30°, and 45° rod lens endoscopes coupled to a high definition camera and monitor (Storz Endoscopy, Tuttlingen, Germany). The surgical dissection was performed using paranasal sinus and skull base/neurosurgical endoscopic instruments (Storz), and a high-speed drill with angled hand-piece, and diamond and cutting burrs (Total Performance System, Stryker, Kalamazoo, MI, USA).
Photographs were taken with 0°, 30°, and 45° rod lens endoscopes coupled to an HD camera and monitor (Storz Endoscopy, Tuttlingen, Germany).
3 Results
A total of ten infratemporal and pterygopalatine fossae (five cadaveric specimens) were dissected endoscopically using a transpterygoid approach. Access was obtained after performing an endoscopic medial maxillectomy and the complete resection of the posterior wall of the antrum. The latter was accomplished using Kerrison rongeurs, starting its removal at the anterior aspect of the sphenopalatine foramen, and proceeding in a medial to lateral direction.
The lateral exposure provided by a medial maxillectomy, performing posterior septectomy may enhance this angle of approach. To dissect the most lateral aspect of the infratemporal fossa, however, it is best to extend the medial maxillectomy anteriorly with or without displacing the nasolacrimal duct. To reach the most lateral part of the infratemporal fossa, we remove the pyriform aperture and ascending process of the maxilla (endoscopic Denker’s or Sturman–Canfield approach). This is done by making a vertical incision just anterior to the head of the inferior turbinate, directly over the edge of the aperture. Extension of the dissection laterally, following a subperiosteal plane, exposes the entire anterior maxilla till the infraorbital foramen and its corresponding nerve and vessel.
After dissecting the periosteum and the fat of the pterygopalatine fossa, the main branches of the third part of the internal maxillary artery were identified including the infraorbital, descending palatine, vidian, sphenopalatine, and posterior nasal arteries (). All branches were transected to expose the underlying neural structures including the infraorbital, descending palatine, vidian, and pharyngeal nerves.
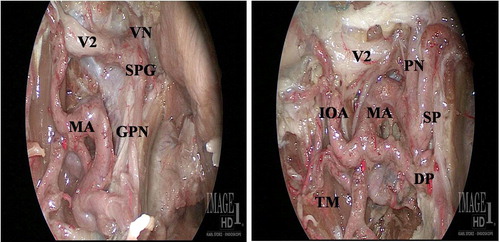
The infraorbital nerve traversing the infraorbital fissure is dissected, just after arising from the maxillary nerve near the foramen rotundum, and before entering the infraorbital canal. This portion of the infraorbital nerve accurately defines the border between the infratemporal fossa and pterygopalatine fossa.
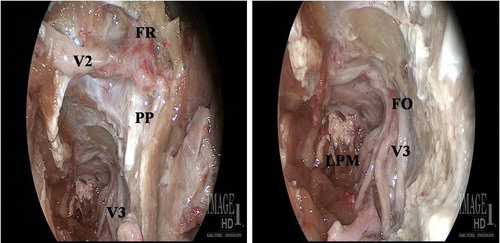
Wide exposure of the infratemporal fossa requires complete removal of the posterior wall from floor to roof of the maxillary sinus. Removal of bone from the floor and lateral wall of the sphenoid sinus exposes the bone comprising the floor of the middle cranial fossa, which is the superior boundary of the infratemporal fossa. The lateral limit is reached when the vertically-oriented temporalis muscle is visualized, while the lateral pterygoid muscle is readily identified by the horizontal orientation of the muscle fibers. The second part of the internal maxillary artery has a variable course, which may run lateral or medial to the lateral pterygoid muscle. This segment of the internal maxillary artery gives off several branches near the anterior border of the lateral pterygoid muscle, including the lingual and buccal arteries, which course anteriorly. The middle meningeal artery may be seen medial to the lateral pterygoid muscle, coursing superiorly toward the foramen spinosum. Resection of the lateral pterygoid muscle and drilling the lateral pterygoid plate improve exposure of the infratemporal fossa, including V3, which lies posterior to the lateral pterygoid plate ().
4 Discussion
Multiple surgical approaches have been described to access the infratemporal fossa. Anterior and lateral approaches were very famous to manage lesions extending in the infratemporal fossa (ITF).Citation11,Citation12 Compared to lateral approaches to the infratemporal fossa, the endoscopic endonasal transpterygoid approach allows better exposure of midline structures such as the nasopharynx, sella, and the clivus.
Moreover, it provides excellent exposure of foramen rotundum, V2, nerve of pterygoid canal, foramen ovale and V3 by drilling of lateral pterygoid plate and dissection of lateral pterygoid muscle. However, some bleeding from the pterygoid venous plexus is expected, that can be controlled with cautry, hemostatic agents and warm saline irrigation.Citation13
In this approach, some of the branches of V2 like descending palatine and alveolar branches are sacrificed. This leads to loss of sensation of hard palate and ipsilateral upper dentition.
The exposure done utilizing the endoscopic endonasal transpterygoid approach to the infratemporal fossa equals or exceeds the exposure provided by traditional anterior approaches and more extensive than the sublabial transmaxillary approach. Moreover, the endoscopic endonasal transpterygoid approach avoids multiple morbidities that are resulting from other lateral and non-endoscopic anterior approaches like cosmetic issues related to skin incision, need for orbitozygomatic osteotomies, or temporalis muscle manipulation, TMJ dysfunction, facial nerve paralysis, craniotomy, and brain retraction, but trismus can also result from resection of lateral pterygoid muscle.Citation14
Also the transpterygoid approach to the infratemporal fossa allows dissection of foramen ovale and V3, that is important for the management of most of tumors that extend to the infratemporal fossa like nasopharyngeal angiofibroma, trigerminal schwanomma and low grade adenocarcinoma. Other extensive malignant tumors of maxilla and/or nasopharynx that extend to the infratemporal fossa can be safely and completely resected using the traditional anterior or lateral approaches or combinations. Sizeable defects are expected and the issue of reconstruction should be taken in consideration.Citation14
Moreover, one of the most important landmarks for the endonasal endoscopic location of the post-styloid space, hence the ICA was the third division of the trigeminal nerve at the level of foramen ovale. Other anatomical landmarks include the Eustachian tube and the Vidian nerve. As a result of the variability of the position of parapharyngeal ICA in close relation to the lateral or even the posterior pharyngeal wall, surgeons should rely on certain landmarks in endoscopic endonasal transpterygoid approach. These anatomical landmarks allow safe and complete resection of lesions that arise or extend to the infratemporal fossa (ITF).Citation15,Citation16
5 Conclusions
Endoscopic endonasal transpterygoid approach is considered one of the most effective surgical solutions for most of benign and some malignant tumors that involve the infratemporal fossa and middle cranial fossa. A good understanding of the endoscopic anatomy of the infratemporal fossa allows safe and complete resection of lesions arising or extending to infratemporal fossa.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 18 February 2014
References
- R.CarrauA.KassamM.ArriagaAnterior and subtemporal approaches to the infratemporal fossa Otologic surgeryBrackmannSheltonArriaga2010Saunders ElsevierPhiladelphia 3rd ed.
- T.HitotsumatsuA.L.RhotonJr.Unilateral upper and lower subtotal maxillectomy approaches to the cranial base: microsurgical anatomyNeurosurgery46200014161452
- G.R.IsolanR.RoweO.Al-MeftyMicroanatomy and surgical approaches to the infratemporal fossa: an anaglyphic three dimensional stereoscopic printing studySkull Base172007285302
- R.TiwariJ.QuakS.EgelerTumors of the infratemporal fossaSkull Base Surg10200019
- W.E.BolgerEndoscopic transpterygoid approach to the lateral sphenoid recess: surgical approach and clinical experienceOtolaryngol Head Neck Surg13320052026
- J.M.DelgadoEndoscopic transnasal approach to the pterygopalatine fossaArch Otolaryngol Head Neck Surg1292003441446
- F.S.FortesL.U.SennesR.L.CarrauEndoscopic anatomy of the pterygopalatine fossa and the transpterygoid approach: development of a surgical instruction modelLaryngoscope11820084449
- A.B.KassamP.GardnerC.SnydermanA.MintzR.L.CarrauExpanded endonasal approach: fully endoscopic, completely transnasal approach to the middle third of the clivus, petrous bone, middle cranial fossa, and infratemporal fossaNeurosurg Focus192005E6
- I.R.HerzallahR.GermaniR.R.CasianoEndoscopic transnasal study of the infratemporal fossa: a new orientationOtolaryngol Head Neck Surg1402009861865
- P.V.TheodosopoulosB.GuthikondaA.BresciaJ.T.KellerL.A.ZimmerEndoscopic approach to the infratemporal fossa: anatomic studyNeurosurgery662010196202 [discussion 202–3]
- M.D.VilelaR.C.RostomilyTemporomandibular joint-preserving preauricular subtemporal-infratemporal fossa approach: surgical technique and clinical applicationNeurosurgery552004143153 [discussion 153–4]
- J.P.LeonettiD.E.AndersonS.J.MarzoT.C.OrigitanoR.SchumanThe preauricular subtemporal approach for transcranial petrous apex tumorsOtolneurotol292008380383
- A.KassamC.H.SnydermanR.L.CarrauP.GardnerA.MintzEndoneurosurgical hemostasis techniques: lessons learned from 400 casesNeurosurg Focus192005E7
- S.Mousa Sadr HosseiniA.RazfarR.L.CarrauD.M.PrevedelloJ.Fernandez-MirandaA.ZanationA.B.KassamEndonasal transpterygoid approach to the infratemporal fossa: Correlation of endoscopic and multiplanar CT anatomyHead Neck2011
- A.D.VescanC.H.SnydermanR.L.CarrauVidian canal: analysis and relationship to the internal carotid arteryLaryngoscope117200713381342
- A.B.KassamA.D.VescanR.L.CarrauExpanded endonasal approach: Vidian canal as a landmark to the petrous internal carotid arteryJ Neurosurg1082008177183