
Abstract
Background
Albumin to creatinine ratio (ACR) in random urine samples correlates well with 24-h protein excretion in potential glomerulopathy as in diabetic renal microangiopathy. Using this ratio as an appropriate screening test for proteinuria or for the disease severity in hypertensive disorders with pregnancy needs still to be verified.
Objective
To investigate the role of albumin to creatinine ratio in a random urine sample for assessment of severity of preeclampsia.
Patients & methods
Two separate groups, fifty women each, were enrolled. All were pregnant at their third trimester with confirmed preeclampsia. Based on their blood pressure levels, Group A, included patients with mild form of preeclampsia, whereas group B included cases with severe form. Albumin to creatinine ratio in random urine samples and the 24-h protein content in urine were assessed.
Results
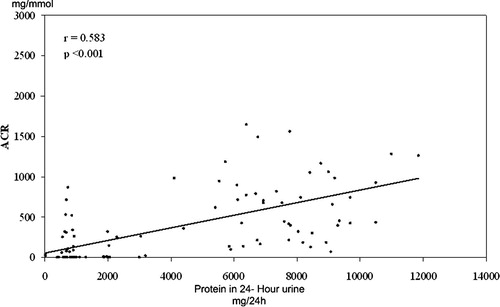
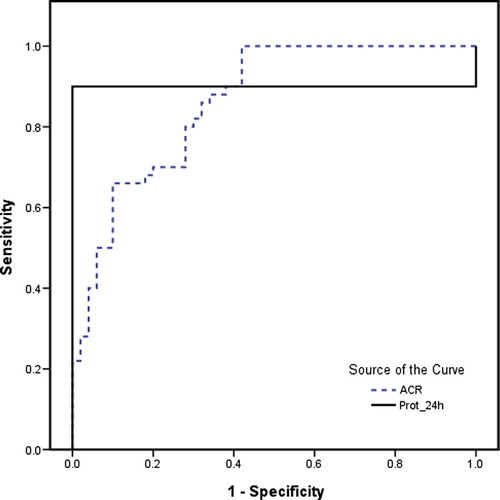
ACR and the 24-h urine protein excretion were significantly correlated, (r = 0.583, p < 0.001). Cut-off value for ACR for this group of patients was calculated to be 14.65 mg/mmol, above which severity of the disease is highly probable. The sensitivity and specificity were 100% and 58.0%, respectively. The positive predictive value was 70.4% and negative predictive value was 100%.
Conclusions
Random urine ACR may be a reliable method for prediction and assessment of severity of preeclampsia. Using the estimated cut-off may add to the predictive value of such a simple quick test.
1 Introduction
Hypertensive disorders complicating pregnancy are common and form one of the deadly triad, along with hemorrhage and infection that contribute greatly to maternal morbidity and mortality.Citation1,Citation2 Preeclampsia is defined as a pregnancy-specific syndrome of reduced organ perfusion secondary to vasospasm and endothelial activation.Citation3–Citation6 Proteinuria is an important sign of preeclampsia, without which, the diagnosis is questionable.Citation7,Citation8 Significant proteinuria is defined by 24-h urinary protein exceeding 300 mg or persistent 30 mg/dl in random urine samples. The degree of proteinuria may fluctuate widely over any 24-h period, even in severe cases. Therefore a single random sample may fail to demonstrate significant proteinuria.Citation9,Citation10
Severe preeclampsia may be diagnosed clinically by persistent diastolic hypertension at or above 110 mm Hg, marked headache, visual symptoms, oliguria or right upper quadrant pain. Persistent proteinuria and abnormal liver or renal function tests are all signs of disease severity as well.Citation11
The measurement of protein excretion in a 24-h urine collection is used as the gold standard for the diagnosis and follow-up of pathologic urinary excretion.Citation12 However, 24-h urine collection is time consuming, inconvenient and often inaccurate especially during pregnancy with less patient’s compliance.
It is of utmost importance to highlight new diagnostic or predictive reliable tests, and hence introduce and apply them in a population with still fairly high maternal mortality rate, such as the Egyptian population. Many suggestions of predictors of severity of preeclampsia in the Egyptian population have been published, such as blood lead level,Citation13 genetic mutation in Endothelial nitric oxide synthase (eNOS) (Glu298Asp) or urotensin II (UTS2 S89N) gene polymorphisms,Citation14 and maternal serum leptin.Citation15
In this study we studied a random urine albumin to creatinine ratio as a simple quick test to predict the presence of significant proteinuria and to assess severity of preeclampsia in Egyptian patients.
2 Patients and methods
One hundred pregnant women attending the Antenatal clinic of our University hospital were enrolled. All women were primigravidae, at or above 28 weeks of gestation and with confirmed diagnosis of preeclampsia. Based on their blood pressure levels, and after a full informed consent was signed, women were recruited into two separate equal groups (50 women each); group A, consisted of patients with mild form of preeclampsia (diastolic blood pressure less than 110 mm Hg3Citation4) and Group B consisted of patients with severe form (diastolic blood pressure at or above 110 mm Hg3Citation4). Patients with chronic hypertension, diabetes mellitus, preexisting renal or vascular disease or urinary tract infection were excluded. The study was formally approved by the Ethical Committee of the Faculty of Medicine, Alexandria University with the following ID:[IRB No. 00006555, FWA No. 00011712,May 2008]. Microalbumin in urine was tested by NycoCard Microalbumin Single Test (Axis-Shield® plc, Oslo, Norway) based upon an immunometric flow-through principle. Quantitative determination of both creatinine and albumin in urine sample was done by Roche/Hitachi 902 analyzer (Roche Diagnostics®, Basel, Switzerland).Citation16,Citation17
The statistical analysis of the data obtained in the present study was carried out using the Statistical Packages for the Social Sciences (SPSS version 15.0, Chicago, IL). Normally distributed data were presented as mean, standard deviation, whereas skewed data were expressed as median and range. Pearson coefficient of correlation was used to find the correlation between two parameters in the same group. ROC curve was plotted to find the diagnostic performance of the variables.
3 Results
The mean values of albumin (mg/L), creatinine (mmol/L), ACR in a random urine sample, and 24-h protein in urine (mg/24-h) in both groups are shown in . Significant statistical differences were found between both studied groups regarding albumin in random urine sample, ACR, and 24-h protein in urine, however, it was not significantly different when it came to creatinine in a random urine sample ().
Table 1 Albumin, creatinine, ACR and protein in urine.
There was a strong positive correlation between ACR and the severity of preeclampsia when Spearman coefficient was applied (r = 0.518, p < 0.001), similarly, the correlation between ACR and the 24-h protein in urine was also found to be significantly positive (r = 0.583, p < 0.001) ().
Using the ROC curve, the cut-off value of ACR for the study subjects was calculated to be 14.65. ACR above this value could be used as a good predictor for the disease severity, with a sensitivity of 100% and a specificity of 58.0%. The positive predictive value was 70.4% and negative predictive value was 100%. The area under the curve (AUC) represented the diagnostic performance of both 24-h urine protein, and ACR. It confirmed a better role for the latter (AUC 0.93) ().
4 Discussion
Preeclampsia is associated with the highest risk of adverse maternal and perinatal complications that affect 2–5% of pregnancies.Citation16 Assessing the presence or absence of significant proteinuria (⩾0.3 g/day) represents a key component in the evaluation of pregnant women with hypertension. Urine collection over 24 h is considered the traditional way for quantification of proteinuria in pregnancy, however, timed collections delay clinical diagnosis and may result in prolonged hospital stay, thereby increasing patient anxiety and healthcare costs. Moreover, it requires more patients’ compliance than could be usually found in pregnancy. Alternatives include: urinary dipsticks, urine collections over a shorter period, the urinary spot protein: creatinine ratio, and the urinary spot albumin: creatinine ratio (ACR). The dipstick is inexpensive, easy to use, and provides a rapid result but has low sensitivity and specificity.Citation18,Citation17 Shorter timed urine collections (2, 4, 8, or 12 h) were also suggested to diagnose proteinuria in pregnancy but still, they have their own limitations.Citation18–Citation20 The spot protein: creatinine ratio and spot ACR have been well studied and used. The National Kidney Foundation now recommends these tests (instead of 24-h urine collection) to diagnose proteinuria in most situations, without specific mention of pregnancy.Citation17 The Australasian Society for the Study of Hypertension in Pregnancy and the International Society for the Study of Hypertension in Pregnancy have proposed the use of the urinary spot protein: creatinine ratio as an alternative to 24 h urine collection.Citation21–Citation25 Up to our knowledge, the spot protein: creatinine ratio is not widely used for the diagnosis of proteinuria in pregnant women with hypertension. In our study, it was shown that ACR is significantly higher in patients with severe preeclampsia than those with a mild form of the disease. Moreover, the correlation between ACR and the 24-h protein in urine was also found to be positive, independent of gestational age, maternal age, blood chemistry or time of disease onset. It was also possible, in the light of this work, to calculate the cut-off value for ACR for the enrolled patients, above which, a severe form of the disease might be predicted. This is to our knowledge the first report in Egypt, to recommend such a test and a cut-off for diagnosis/follow up of albuminuria in pregnancy, which can, thus, be used as a marker of severity of preeclampsia. Finally, a better diagnostic potential for ACR than a 24-h urine protein, was suggested based on our result analysis. In conclusion, ACR measurement is a simple, quick, and reasonably-reliable method for assessment of severity of preeclampsia.
Conflicts of interest
None.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 31 January 2014
References
- C.J.BergJ.ChangW.M.CallaghanS.J.WhiteheadPregnancy-related mortality in the United States 1991–1997Obstet Gynecol10122003 Feb289296
- B.SibaiG.DekkerM.KupfermincPre-eclampsiaLancet36594612005785799
- G.A.DekkerB.M.SibaiEtiology and pathogenesis of preeclampsia: Current conceptsAm J Obstet Gynecol1795199813591375
- J.M.RobertsPregnancy-related hypertensionR.K.CreasyR.ResnikMaternal-Fetal Medicine2nd ed.1998WB Saunders CompanyPhiladelphia, PA (1), 833: 72
- S.CampbellM.Pearce JG.HackettT.Cohen – OverbeekC.HernandezQualitative assessment of uteroplacental blood flow: early screening test for high risk pregnancies Obestet Gynecol681996649658
- H.J.KlimanUteroplacental blood flow the story of decidualization, menstruation and trophoblast invasionAm J Pathol157200017591768
- ACOG practice bulletin. Diagnosis and management of preeclampsia and eclampsia. Number 33, January 2002. Obstet Gynecol 2002; 99(1):159-67.
- Beaulieu MD. Prevention of pre-eclampsia. Canadian Guide to clinical preventive Health care. Ottawa: Health Canada 1994; 136–43.
- N.L.MeyerB.M.MercerS.A.FriedmanB.M.SibaiUrinary dipstick protein: a poor predictor of absent or severe proteinuriaAm J Obstet Gynecol1701 Pt 11994137141
- S.FerrazzaniA.CarusoS.De CarolisI.V.MartinoS.MancusoProteinuria and outcome of 444 pregnancies complicated by hypertensionAm J Obstet Gynecol16221990366371
- National High Blood Pressure Education Program Working group report on high blood pressure in pregnancyAm J Obstet Gynecol18312000S1S22
- A.M.AdelbergJ.MillerM.DoerzbacherD.S.LambersCorrelation of quantitative protein measurements in 8-, 12-, and 24-h urine samples for the diagnosis of preeclampsiaAm J Obstet Gynecol18542001804807
- S.M.MotaweiS.M.AttallaH.E.GoudaLead level in pregnant women suffering from pre-eclampsia in DakahliaEgypt. Int J Occup Environ Med420133644
- W.S.El-SherbinyA.S.NasrA.SolimanEndothelial nitric oxide synthase (eNOS) (Glu298Asp) and urotensin II (UTS2 S89N) gene polymorphisms in preeclampsia: prediction and correlation with severity in Egyptian femalesHypertens Pregnancy3232013 Aug292303
- A.M.El ShahatA.B.AhmedM.R.AhmedH.S.MohamedMaternal serum leptin as a marker of preeclampsiaArch Gynecol Obstet28862013 Dec13171322
- A.WheltonNitrogen metabolites and renal functionC.A.BurtisE.R.AshwoodTietz Textbook of Clinical Chemistry2nd ed.1994WB Saunders CompanyPhiladelphia, PA
- N.W.TietzClinical Guide to Laboratory Teststhird ed.1995WB SaundersPhiladelphia, Pa pp. 22–24
- G.L.MyersW.G.MillerJ.CoreshJ.FlemingN.GreenbergT.GreeneRecommendations for improving serum creatinine measurement: a report from the Laboratory Working Group of the National Kidney Disease Education ProgramClin Chem522006518
- L.K.PhelanM.A.BrownG.K.DavisG.MangosA prospective study of the impact of automated dipstick urinalysis on the diagnosis of preeclampsiaHypertens Pregnancy232004135142
- J.WaughM.KilbyP.LambertS.C.BellC.N.BlackwellA.ShennanValidation of the DCA 2000 microalbumin:creatinine ratio urinanalyzer for its use in pregnancy and preeclampsiaHypertens Pregnancy2220037792
- A.M.AdelbergJ.MillerM.DoerzbacherD.S.LambersCorrelation of quantitative protein measurements in 8-, 12-, and 24-h urine samples for the diagnosis of preeclampsiaAm J Obstet Gynecol1852001804807
- W.EvansJ.P.LensmeyerR.S.KirbyM.E.MalnoryF.F.BroekhuizenTwo-hour urine collection for evaluating renal function correlates with 24-h urine collection in pregnant patientsJ Matern Fetal Med92000233
- N.SomanathanT.FarrellA.GalimbertiA comparison between 24-h and 2-h urine collection for the determination of proteinuriaJ Obstet Gynaecol232003378380
- J.A.VassalottiL.A.StevensA.S.LeveyTesting for chronic kidney disease: a position statement from the National Kidney FoundationAm J Kidney Dis502007169180
- M.A.BrownM.D.LindheimerM.De SwietA.Van AsscheJ.M.MoutquinThe classification and diagnosis of hypertensive disorders of pregnancy: Statement from the International Society for the Study of Hypertension in Pregnancy (ISSHP)202001321322