
Abstract
Shoulder joint pain due to anterior microinstability is not an unusual complaint of young active individuals. Different etiologies of such shoulder microinstability are encountered, mainly affecting the anterior–inferior labro-ligamentous capsular structures. These injuries include Perthes lesion, ALPSA, GLAD, RIT, SLAP and glenohumeral ligamentous injuries.
The aim of this study
The aim of this study is to enhance the role of MR arthrogram over routine MRI in the diagnosis of such subtle lesions.
Patients and methods
This is a prospective study, involving 30 consecutive patients of shoulder microinstability complaints, evaluated by MR arthrogram of the affected shoulder.
Results
Perthes lesions were diagnosed in 6 patients, ALPSA in 3 patients, GLAD in 2 patients, RIT in 2 patients and SLAP in 11 patients. Ligamentous injuries that include tear of MGHL, were found in 2 patients and IGHL in 4 patients.
Conclusion
MR arthrogram is highly recommended for the management of young patients with shoulder microinstability or unexplained painful movement complaints.
Abbreviations:
- ABER
- abduction external rotation
- AIOS
- Acquired Instability in Overstressed shoulder, surgery
- ALPSA
- anterior labral ligamentous periosteal sleeve avulsion
- AMSI
- Atraumatic Minor Shoulder Instability
- GLAD
- glenolabral articular disruption
- IGLI
- avulsion of inferior glenohumeral ligament
- MGL
- middle glenohumeral ligament
- RI
- rotator interval
- RIT
- rotator interval tear
- SLAP
- superior labrum anterior to posterior tear
- TUBS
- Traumatic, Unidirectional, Bankart lesion, responds to surgery
1 Introduction
Shoulder joint instability has been classified, according to etiology and management response, into two major items: the so-called TUBS (Traumatic, Unidirectional, Bankart lesion, responds to surgery) and on the other AMBRII (Atraumatic, Multidirectional, Bilateral, responds to rehabilitation, inferior capsular shift, interval closure). Between these two extremes there is a wide group of conditions, defined as minor or microinstability, including AIOS (Acquired Instability in Overstressed shoulder, surgery) and AMSI (Atraumatic Minor Shoulder Instability), that are common complaints of young active individuals.Citation1,Citation2
The glenohumeral joint has a loose lax capsule; therefore it is solely at risk of dislocation and in need for additional supporting factors. The strongest stabilizing structures of the glenohumeral joint are the rotator cuff muscles. Additionally, the glenoid labrum is another important structure for maintaining shoulder stability, as it deepens the socket shaped bony glenoid, providing more coverage and stability of the articulating ball shaped humeral head. Also, it provides attachment of the glenohumeral ligaments, long head of biceps and joint capsule to the glenoid rim. The glenohumeral ligaments act to reinforce the joint capsule, and provide more joint support.Citation3,Citation4
Recent advances in arthroscopic shoulder surgery necessitate accurate imaging diagnosis of such stability insults, facilitating successful repair. The most common causes of microinstability are injuries within the anterior and superior additional supporting structures i.e. injuries around rotator interval (RI). Spectrum of these insults includes superior labrum anterior to posterior tear (SLAP), rotator interval (RI) tears, and partial anterior labral tears like Perthes and anterior labral ligamentous periosteal sleeve avulsion (ALPSA) lesions. Also, avulsion of the inferior glenohumeral ligament (IGL) or middle glenohumeral ligament (MGL) is an additional non-stabilizing insult.Citation5,Citation6
2 Patients and methods
This is a prospective study of 30 MR arthrography examinations performed between January 2011 and December 2013, for patients with anterior shoulder pain or impingement like symptoms, with negative X ray findings. Also, the selection did not include patients with positive routine MRI findings of bony or rotator cuff injuries, as they were excluded from the study. Candidate patients were referred for shoulder MR arthrogram after failure of non-steroidal analgesic therapy and rehabilitation programs. The study protocol was approved by the scientific and ethics committee in the Al-Mana General Hospital, Eastern Province, Saudia Arabia. Signed consents were obtained from all study candidates, for acceptance of both arthrographic MRI examination and study participation.
3 Aim of the study
The study aims to enhance the role of MR arthrogram examinations in the diagnosis of some stabilizing factors and defects that may be missed in routine MRI examinations in young active patients with shoulder microinstability.
4 Technique
After conventional MR sequences were performed, patients were shifted to a fluoroscopic X-ray room. Patients were positioned supinely on a fluoroscopy table (Diagnost 96, Philips Medical Systems, St-Laurent, QC, Canada) with the arm in external rotation to avoid the long head of the biceps tendon. If this position is too painful for the patient, neutral position -with palm against the thigh- was used instead. At AP shoulder joint position, the skin was marked over the upper medial quadrant of the humeral head, in close approximation with the articular joint line. Under strict sterile aseptic technique, the skin was anesthetized with Xylocain 1% using a 20 or 22-gauge spinal needle.
With intermittent fluoroscopy, the needle was introduced parallel to the X-ray beam or with a slight medial angulation until it came in contact with the humeral head, then slightly pulled up for 1 or 2 mm. 1 ml of contrast was then injected to ascertain the intraarticular position of the needle. Finally, injection of 20 ml of a contrast mixture, made of 10 ml normal saline, 5 ml Omnipaque 300, 4 ml 1% lidocaine and 0.1 ml gadolinium through a 20 cm syringe was made. Then the patient was shifted to MRI again, for postcontrast imaging. Post contrast axial, sagittal and coronal T1w fat sat sequences, as well as ABER sequences were obtained. All examinations were done through MRI Philips Intera 1.5 T, Closed Magnet, Philips Medical Systems, 5656 AE Eindhoven, Netherlands.
5 Review of MR arthrogram findings
The images were checked by the radiology author who is experienced in MRI shoulder studies, first separately, then in group discussion with the orthopedic author, who got ten years experience in shoulder arthroscopic and surgical procedure. Lastly, reports were made after reaching a conclusion in consensus.
6 Results
The study involved 30 consecutive patients of shoulder microinstability complaints. Age of 11 patients was less than 30 years, 15 patients ages were from 30–40 years, and 4 patients were 40–50 years. ()
Table 1 Different age groups of the study candidates.
Labro-capsular injuries including Perthes lesions were diagnosed in six patients ( and ), ALPSA in three patients (), GLAD in two patients (), RIT in two patients () and SLAP in eleven patients (), in comparison to ligamentous injuries that include tear of MGHL which were found in two patients and IGHL in four patients. () ().
Figure 1 MR arthrogram axial T1w fat sat images of Perthes lesion show non displaced torn segment of the anterior labrum (arrow in A) with still intact glenoid peiosteal link (arrow in B).
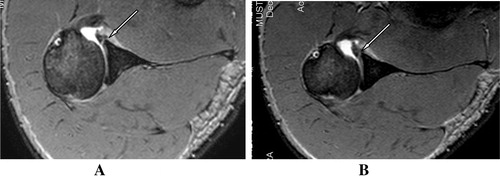
Figure 2 Perthe’s lesion in a 35 year old patient, with minimally displaced inverted torn labral segment(arrow), with still intact periosteum.
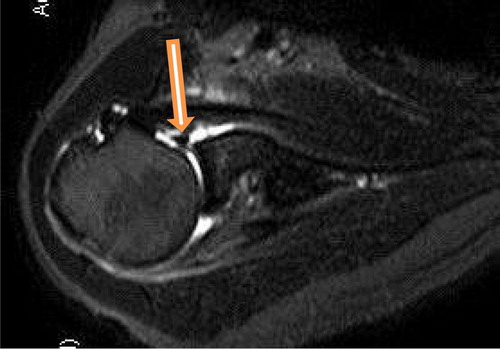
Figure 3 (A, B) Axial T1 fat sat MR arthrogram shows torn and medially displaced anterior glenoid labrum (Arrow in A), with still intact periosteum (Chevron in B), consistent with ALPSA lesion.
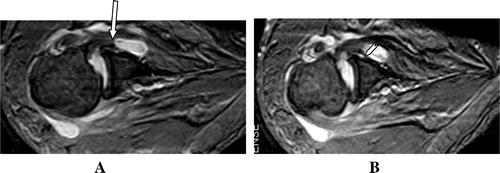
Figure 4 (A, B) Axial MR arthrogram T1 Fat Sat. Images show anterior scapular articular cartilage thin disruption consistent with GLAD injury (arrows).
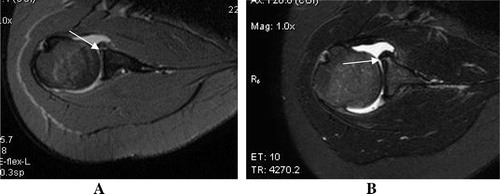
Figure 5 (A, B) Sagittal T1w Fat Sat. MR arthrogram images showing rotator interval tear, seen as extrasynovial leakage of contrast through the defect (arrows) into anterior extra-articular tissues.
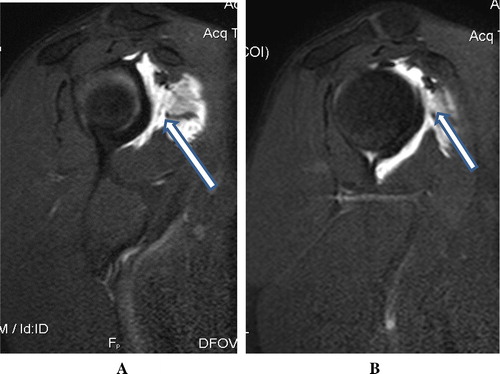
Figure 6 (A) Diagram of type II and III normal variants of labral attachment, as shown in coronal MRI sequence (arrows).Citation20 (B, C) Coronal MR arthrogram T1 fat sat. Images showing SLAP II injury of superior labrum with non-detached labrum (notice the wide gab >3 mm.) (arrows) and intact biceps tendon (Chevron in B).
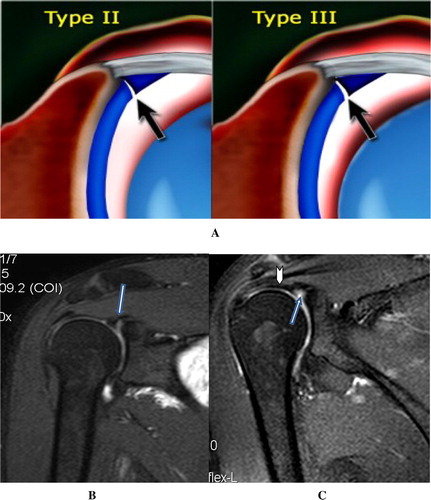
Figure 7 (A, B) Axial MR arthrogram T1 fat sat. Images showing interrupted glenoid attachment of the middle glenohumeral ligament with frayed distorted fibers (arrows).
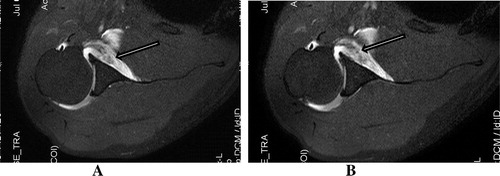
Table 2 Different types of lesions diagnosed by the MR arthrogram.
7 Discussion
The cumulative microtraumatic stresses on the shoulder joint represent challenges for the physiologic limits of the stabilizing structures and often compromise the static status of the joint. This finally makes shoulder micro-instability not an uncommon occurrence in young active individuals. Many of the causative factors can be surgically corrected, regaining the painless stable status, if early managed. This is because it helps to avoid the uncorrected muscular atrophy which is the end-stage of long standing missed insults. These subtle lesions can be easily missed on routine plain MRI examinations, especially if MRI power is less than 3 tesla, hence the importance of MR arthrogram examinations.Citation7,Citation8
The glenoid labrum is a wedge-shaped fibrous ring, which is attached to the glenoid articular surface through a fibrocartilaginous transition zone. The inferior labrum is firmly continuous with the articular cartilage; while its upper half is more mobile i.e. meniscus like configuration. Anterior labral insults include three types. Type I, in which the labrum is completely separated from the glenoid bone, is termed the Bankart lesion. In type II, which is termed Perthes lesion, the labrum is incompletely separated from the glenoid bone, due to the periosteum which is still intact, while in type III, the torn labral segment is retracted medially with the intact periosteum (ALPSA).Citation9,Citation10
Bankart lesion has been reported to result in a 50% decrease in the glenoid depth. Lippit et al.Citation11 demonstrated that the translational force required to dislocate the humeral head was 20% smaller after removal of the glenoid labrum. Bankart lesions are usually easily demonstrated by routine MRI workup, however, the other clinically significant labral injury types are less clear and may be missed, namely Perthes and ALPSA lesions.Citation11,Citation12
In Perthes lesion – which was diagnosed in 6 patients – there is only minimal displacement of the torn anterior labrum due to still intact periosteal glenoid connection, hence the lesions may be missed on routine MRI examination. MR arthrogram is more accurate and clearly delineates the torn segment. However, it sometimes had some limitation in demonstrating the non-displaced tears, hence the requirement of additional abduction external rotation (ABER) technique in arthrographic MRI study. ABER stretches the anteroinferior joint capsule and IGHL and helps in better delineation of the lesion. So, it is widely agreed that the ABER MR arthrogram is the most diagnostic sequence for these insults.Citation13
ALPSA lesion – which was diagnosed in 3 patients – was first defined by Neviaser et al.Citation14, as avulsion and gross medial displacement of the inferior labroligamentous complex, with a still intact periosteum. MR arthrogram is sensitive for diagnosis and clear demonstration of this insult. This is one of the most beneficial tools of MR arthrogram, as this lesion can be easily missed on arthroscopy, if there is no previous notification about such insult.Citation14,Citation15
Glenolabral articular disruption (GLAD) -which was diagnosed in 2 patients – consists of an anterior labral tear associated with an anterior articular cartilage injury. The use of intra-articular contrast in the MR arthrogram helps to visualize small tears at the level of the anterior–inferior glenoid rim. GLAD lesions are usually presented clinically with clicking during shoulder joint movement. It is one of the important causes of anterior shoulder pain, regardless it alone is not responsible for shoulder instability as described by Neviaser Citation16
Rotator interval tear – diagnosed in 2 patients – is a subtype of rotator cuff tear which represents torn joint capsule between the supraspinatus and subscapularis tendons. This injury limits flexion and external rotation. MR arthrogram is essential for diagnosis of such injury, through demonstrating the extracapsular subscapularis contrast leak through the rotator interval defect. Routine MRI could not clearly diagnose this capsular defect.Citation16,Citation17
The superior labrum is originally more loosely attached and more mobile than the inferior labrum. This normal laxity leads to some diagnostic difficulty in identifying SLAP lesions. There are some variants of the superior labrum that may simulate SLAP tears for unspecialized radiologists. For example, in of Buford complex variant, there is absence of anterosuperior portion of the labrum, associated with a cordlike middle glenohumeral ligament. Also, anatomic variations commonly occur in the superior labrum glenoid attachments that include sublabral recess (sulcus) and sublabral foramen (hole).Citation18,Citation19 There are 3 types of attachment of the superior labrum at the 12 O’clock position where the biceps tendon is inserted. In type I there is no recess between the glenoid cartilage and the labrum. In type II there is a small recess. In type III there is a large sublabral recess (A). This sublabral recess can be difficult to distinguish from a SLAP tear. It is widely agreed that a defect more than 3 mm should be considered SLAP tear.Citation20
Snyder et al.Citation21 classified SLAP lesions – that were diagnosed in 11 patients – into four types on the basis of arthroscopic evaluation. Type I lesion represents fraying, without frank tear. Type II lesion consists in stripping of the superior labrum and biceps tendon from the underlying glenoid cartilage. Type III lesion is a bucket-handle displaced tear, if it involves the biceps tendon, it will be classified as type IV. Additional classes were added by Maffet et al.Citation22 in 1995, reporting ten classes of SLAP injuries according to associated other joint part injuries to the initial four classes of the SLAP lesion. MR arthrogram can confidently demonstrate the complete extent of the labral tear, which can be easily missed on routine MRI. So, MR arthrogram clearly determines the different classes of injury, which is essential for management decisions.Citation18
Tear or avulsions of the middle or inferior glenohumeral ligaments – that were diagnosed in 6 patients – from either humeral or glenoid sides (HAGL or GAGLE) are also considered important factors for anterior glenohumeral instability. Unless there is considerable effusion, diagnosis of these lesions will be difficult in plain MRI, however in the MR arthrogram there will be clear demonstration of the torn fibers and the gab formed by their retraction. This is also considered a crucial informative guide for the plan of management.Citation22
8 Conclusion
| • | Shoulder microinstability is not an uncommon complaint of young active people. | ||||
| • | Superior and anterior labroligamentous-capsular lesions are responsible for the etiology of such instability. | ||||
| • | Routine shoulder MRI and even sometimes arthroscopy may not confidently diagnose such injuries. | ||||
| • | MR arthrogram is the most accurate helpful tool of imaging in diagnosis, classification and treatment planning of these injuries. | ||||
Conflict of interest
The authors declare that they have no conflict of interest.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 1 May 2014
References
- A.CastagnaU.NordensonR.GarofaloJ.KarlssonMinor shoulder instabilityJ Arthroscop Relat Surg2322007211215
- S.B.LippittD.T.HarrymanIIJ.S.SidlesF.A.MatsenIIIDiagnosis and management of AMBRI syndrome techniquesTech Orthop619916173
- A.HafizuddinDislocation of shoulder joint. Review ArticleKYAMC22011140145
- A.TateG.N.TurnerS.E.KnabC.JorgensenA.StrittmatterL.A.MichenerRisk factors associated with shoulder pain and disability across the lifespan of competitive swimmersAthl Train4722012149158
- Asgar M.Saleem1Joong K.LeeLeon M.NovakUsefulness of the abduction and external rotation views in shoulder MR arthrographyAJR191200810241030
- J.L.HalbrechtP.TirmanD.AtkinInternal impingement of the shoulder: comparison of findings between the throwing and nonthrowing shoulders of college baseball playersArthroscopy151999253258
- S.H.LiuM.H.HenryAnterior shoulder instability: current reviewClin Orthop Relat Res3231996327337
- Matsen FA, Thomas SC, Rockwood CA, Wirth MA. Glenohumeral instability, in the Shoulder. 2nd ed. Philadelphia (PA), USA: W.B. Saunders; 1998, vol. 2: p. 611–89.
- Mutlu S, Mahir M, Lullari J, Güler O, Uçar BY, et al. Clinical study: anterior glenohumeral instability: classification of pathologies of anteroinferior labroligamentous structures using MR arthrography. Adv Orthoped 20113: http://dx.doi.org/10.1155/2013/473194.
- L.U.BiglianiP.M.NewtonP.ScottM.PatrickLesions associated with recurrent anterior dislocation of the shoulderAm J Sports Med2619984145
- S.B.LippitJ.E.VandorhooftS.L.HarrisGlenohumeral stability from concavity compression: a quantitative analysisJ Shoulder Elbow Surg219932735
- Erkoçak ÖF, Yel M. The functional results of arthroscopic bankart repair with knotless anchors for anterior glenohumeral instability. Eur J General Med 2010; 7(No. 2):179–86.
- A.M.SaleemJ.K.LeeL.M.NovakUsefulness of the abduction and external rotation views in shoulder MR arthrographyAJR191200810241030
- T.J.NeviaserThe anterior labroligamentous periosteal sleeve avulsion lesion: a cause of anterior instability of the shoulderArthroscopy9Issue 119931721
- S.AcidT.L.CorrollerR.AswadV.PaulyP.ChampsaurPreoperative imaging of anterior shoulder instability: diagnostic effectiveness of MDCT arthrography and comparison with MR arthrography and arthroscopyAJR1982012661667
- T.J.NeviaserThe GLAD lesion: another cause of anterior shoulder painArthroscopy919932223
- O.P.KrieMRI of the rotator interval capsuleAJR184200514901494
- A.V.Mohana-BorgesC.B.ChungD.ResnickSuperior labral anteroposterior tear: classification and diagnosis on MRI and MR arthrographyAJR181200314491462
- M.D.MaeseneerF.Van RoyL.LenchikM.ShahabpourCT and MR arthrography of the normal and pathologic anterosuperior labrum and labral–bicipital complexRadiographics202000S67S81
- Smithuis R, van der Woude HJ. Shoulder MR – anatomy: normal anatomy, variants and checklist .http://www.radiologyassistant.nl/en/p4f49ef79818c2/shoulder-mr-anatomy.html.
- S.J.SnyderR.P.KarzelW.Del PizzoSLAP lesions of the shoulderArthroscopy61990274279
- E.M.WolfJ.C.ChengK.DicksonHumeral avulsion of glenohumeral ligaments as a cause of anterior shoulder instabilityArthroscopy111995600607