
Abstract
Background
Thyroid nodule evaluation is usually done using a fine needle aspiration cytology/biopsy. The aim of this study was to evaluate the role of diffusion weighted imaging to differentiate benign from malignant thyroid nodules.
Methods
Sixty-one patients, 15 males and 46 females (30–70 years, mean age 49.08 years) with thyroid nodules were included in the study. Routine MRI of neck and diffusion-weighted MR imaging was performed using multiple b-values. Apparent diffusion coefficient (ADC) values were done for the different b-values. Histopathological results of the thyroidectomy samples were obtained. Comparison of apparent diffusion coefficient values of thyroid nodules with the histopathology was done.
Results
The pathology results showed that there were 38 and 23 benign and malignant thyroid nodules respectively. ADC value for b-values of 0–300 s/mm2 was used to evaluate the ADC values for benign and malignant thyroid nodules which were significant (p < 0.001). Higher ADC values were seen in benign nodules (ADC: 2.32 ± 0.44 × 10–3 mm2/s) than malignant ones (1.40 ± 0.40 × 10–3 mm2/s).
Conclusion
Differentiation of thyroid nodules whether benign or malignant can be done using the diffusion-weighted MR technique.
1 Introduction
There is a great increase in the incidence of thyroid cancer.Citation1,Citation2 Thyroid cancer is the most common endocrine tumor. Incidence of thyroid cancer is increasing by 6%.Citation3
Fine needle aspiration cytology guided by ultrasonography can prevent unnecessary thyroidectomy and precise the extent of surgical resection.Citation4,Citation5
Thyroid ultrasonography can provide information with regard to nodule diameter, structure of the nodule whether cystic or solid, presence of classification, regular margin and absence of halo sign but still no reliable criteria for distinguishing benign from malignant lesions. In addition, it is difficult to diagnose the malignancy of the nodule when it is large or multinodular.Citation6,Citation7
Despite great improvement in diagnostic techniques such as thyroid scan and CT scan of neck, there is still a large problem to use a non-invasive and reliable technique to differentiate benign from malignant thyroid nodules. Recent developments in MRI techniques may be of diagnostic value.Citation8
Diffusion-weighted MR imaging (DWI) is an emerging technique for brain tumors. DWI is sensitive to changes in the microstructural organization of tissue that may affect water diffusion. It has been used to evaluate head and neck tumors.Citation9–Citation11 The Apparent Diffusion Coefficient (ADC) value is a quantitative parameter for distinguishing malignant tumors from benign thyroid nodules.
We compare ADC value of thyroid nodules with their histopathology and then evaluate its role in differentiating malignant from benign thyroid nodules.
2 Patient selection
Between February 2012 and February 2014, 61 patients (15 males; 46 females) with determined thyroid nodules either by clinical examination or by ultrasonography were prospectively enrolled and patient consent was obtained. Mean age of those patients was 49.08 years (range 30–70 years). Routine neck MR imaging and diffusion-weighted MR imaging were performed for each patient. All patients will be subjected to thyroidectomy within 2 weeks and then followed by histopathology result. Histopathology revealed that 38 patients had benign lesions, including thyroid adenoma (N = 30) and nodular goiter (N = 8),) while 23 patients were found to have malignant lesions, including thyroid papillary carcinoma (N = 13), follicular thyroid cancer (N = 7) and atypical hyperplasia (N = 3).
3 MRI technique
MR scanning was performed on a GE Sigma HD 1.5 T MR scanner. The patients lay spine and asked to avoid movement and swallowing as possible. Routine MRI examinations were done with the following parameters: fast spin echo (FSE) scanning for neck, axial T1WI (TR = 520 ms, TE = 14 ms), T2WI (TR = 3500 ms, TE = 95 ms) and coronal T2WI (TR = 3000 ms, TE = 85 ms). Thickness = 4 mm, spacing = 1 mm. FOV = 14 cm × 14 cm, matrix = 320 × 256, NEX = 4.
Diffusion Weighted MR Imaging (DWI) in axial plane was acquired using four different b factors (0, 300, 500, and 800 s/mm2). All DWI scans were acquired with the same parameters: TR = 3000 ms, TE = 60 ms, matrix = 96 × 128, thickness −4 mm and 6 averages. Total scanning time was about 10 min for the DWI scan.
4 Image post processing
Using the post processing software Functool from GE, ADC maps were automatically generated for each of the b factors. ADC values were extracted from ADC maps. Circular ROIs (regions of interests) with an area of 1 cm2 were carefully placed on the lesions (areas of necrosis, hemorrhage, calcium and cyst formation were excluded).
ROIs were placed on one ADC map and then evaluated the other 2 by two experienced radiologists. To minimize noise, each radiologist made three measurements for each lesion and the mean ADC value was recorded. Final ADC value was determined by the mean values from two rates.
5 Analysis
ADC was done at the following b values of 300, 500, and 800 s/mm2. Statistical analysis was performed. All ADC data were recorded in mean ± SD (×10−3 mm2/s) form. The Mann–Whitney U-test was performed to compare the quantitative ADC value of benign and malignant thyroid nodules. A value of p < .05 was considered significant.
6 Results
MRI results revealed that among those 61 patients of nodules in the thyroid, ADC measurements were measured at different b values. The patients were 38 and 23 benign and malignant nodules respectively. In both types of thyroid nodules benign and malignant ones females were more common than females ().
Table 1 Characteristics of 61 patients with thyroid nodules.
For ADC values at b value of 300 s/mm2, we found that benign lesions were significantly higher than malignant nodules (p < 0.001) ( and ). Mean ADC value for the benign group (2.33 ± 0.47 × 10–3 mm2/s) () is much higher than that for malignant nodule (1.13 ± 0.60 × 10–3 mm) (). We found no statistical difference in b value at 5000 and 800 s/mm2. Also at b value of 300 s/mm2 the ADC value showed the highest sensitivity and specificity ( and ).
Figure 1 37 year old female presented with papillary thyroid cancer: Coronal T1: shows large heterogeneous nodule mainly involving the right lobe, nodule shows multiple hyper intense foci that denote …hemorrhagic foci, encroached upon the air column. Axial T1 shows ill heterogeneous nodule mainly involving the right lobe. It shows restricted diffusion.
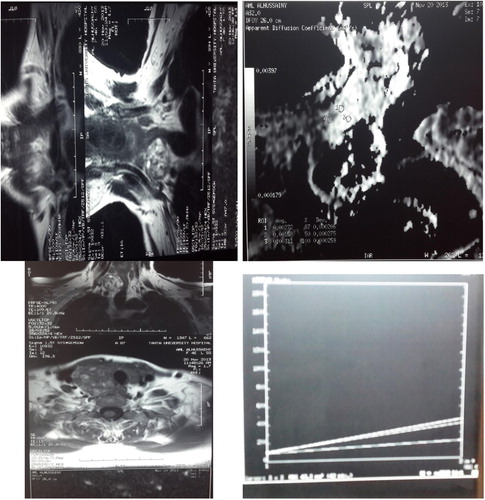
Figure 2 A female patient aged 46 years presented with follicular adenoma. (A) and (B), axial T1- and T2-weighted MR images, respectively, showing a well-defined solitary nodule affecting the right thyroid lobe. (C) An ADC map image with marked hyperintensity of the anterior cystic portion of the nodule (arrow), denotes increased diffusion with a measured ADC value of 2.25 ± 0.18 × 10–3 mm2/s and a relatively hypointense posterior solid portion, denotes relatively restricted diffusion with a measured ADC value of 1.2 ± 0.08 × 10–3 mm2/s.
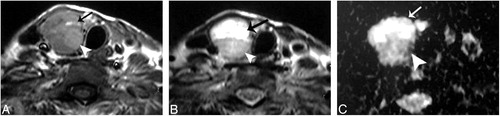
Table 2 Association between different patients’ characteristics and pathology.
Table 3 Sensitivity and specificity and AUC of the use of mean ADC value as calculated based on 3 different b-values for differentiating benign from malignant thyroid lesions.
7 Discussion
Diffusion weighted imaging is one of the functioning MRI modalities which was used to evaluate thyroid nodules.Citation12
Diffusion weighted signal is produced from the movement of water in the intra, and extra cellular spaces and also from intravascular spaces. According to degree of cellularity the MRI image appeared. The malignant tumors had reduced extracellular spaces with resultant reduction in apparent diffusion coefficient.Citation13
The b-value in the DWI was an important factor for image quality. We obtained diffusion-weighted MR images with different b values. Higher b-values produce higher contrast between thyroid lesions and normal tissue. Our results showed that a b-factor of 300 s/mm2 was sufficient to obtain high quality ADC values and it was also the one which had a high sensitivity and accuracy for differentiating benign and malignant nodules. These results are consistent with Bozgeyik’sCitation10 results.
In this study we used the gold reference for malignancy which was based on the histopathology after thyroidectomy. Our results showed a significant difference in the ADC value between benign and malignant thyroid lesions, with ADC values in benign lesions being higher than malignant lesions (ADC: 2.33 ± 0.47 × 10–3 mm2/s vs. malignant: 1.13 ± 0.60 × 10–3 mm2/s) at the b factor of 300 s/mm2. These results are consistent with other similar studies.Citation10,Citation11,Citation14–Citation16
However, in Weidekamm’sCitation17,Citation18 study, the opposite result was reported. ADC values were higher in malignant thyroid nodules than that in benign nodules with values equal to or more than 2.25 × 10–3 mm2/s.
8 Conclusion
In conclusion, differentiation of thyroid nodules could be done using ADC values depending on MRI diffusion weighted imaging.
Competing interests
The authors declare that they have no competing interests.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
accepted 10 September 2014
References
- T.S.DesserA.KamayaUltrasound of thyroid nodulesNeuroimaging Clin N Am1832008 Aug463478
- G.P.YuJ.C.LiD.BranovanThyroid cancer incidence and survival in the national cancer institute surveillance, epidemiology, and end results race/ethnicity groupsThyroid2052010465473
- R.SiegelD.NaishadhamA.JemalCancer statisticsCA Cancer J Clin62120121029
- B.WojtczakK.SutkowskiM.BolanowskiThe prognostic value of fine-needle aspiration biopsy of the thyroid gland – analysis of results of 1078 patientsNeuro Endocrinol Lett3352012511516
- K.L.McCoyN.JabbourJ.B.OgilvieThe incidence of cancer and rate of false-negative cytology in thyroid nodules greater than or equal to 4 cm in sizeSurgery1422007837844
- M.C.FratesC.B.BensonJ.W.CharboneauManagement of thyroid nodules detected at US: Society of Radiologists in Ultrasound consensus conference statementRadiology23732005794800
- J.Y.KwakE.K.KimM.J.KimThe role of ultrasound in thyroid nodules with a cytology reading of “suspicious for papillary thyroid carcinoma”Thyroid1852008517522
- M.GotwayC.HigginsMR imaging of the thyroid and parathyroid glandsMagn Reson Imaging Clin N Am82008163182
- Y.WuX.YueW.ShenDiagnostic value of diffusion-weighted MR imaging in thyroid disease: application in differentiating benign from malignant diseaseBMC Med Imaging131201323
- Z.BozgeyikS.CoskunA.F.DagliDiffusion-weighted MR imaging of thyroid nodulesNeuroradiology5132009193198
- A.A.RazekA.G.SadekO.R.KombarRole of apparent diffusion coefficient values in differentiation between malignant and benign solitary thyroid nodulesAJNR Am J Neuroradiol2932008563568
- M.TezukaY.MurataR.IshidaMR imaging of the thyroid: correlation between apparent diffusion coefficient and thyroid gland scintigraphyJ Magn Reson Imaging JMRI172003163169
- K.HolzapfelS.DuetschC.FauserValue of diffusion-weighted MR imaging in the differentiation between benign and malignant cervical lymph nodesEur J Radiol7232009381387
- G.ErdemT.ErdemH.MuammerDiffusion-weighted images differentiate benign from malignant thyroid nodulesJ Magn Reson Imaging JMRI31201094100
- A.R.PadhaniA.Dzik-JuraszPerfusion MR imaging of extracranial tumor angiogenesisTop Magn Reson Imaging15120044167
- J.R.AndersonMuir’s textbook of pathology13th ed.1992Edward ArnoldLondon
- C.Schueller-WeidekammK.KasererCan quantitative diffusion-weighted MR imaging differentiate benign and malignant cold thyroid nodules? Initial results in 25 patientsAJNR Am J Neuroradiol302009417422
- C.Schueller-WeidekammG.SchuellerDiagnostic value of sonography, ultrasound-guided fine-needle aspiration cytology, and diffusion-weighted MRI in the characterization of cold thyroid nodulesEur J Radiol732010538544