
Abstract
Background
Obesity has become a major global health challenge due to established health risks and substantial increases in prevalence. Being a complex condition it contributes to burden of chronic diseases by affecting virtually all ages and socioeconomic groups. This study aims to identify the prevalence of obesity and blood lipid profile and their associated factors in Jalalabad city, Afghanistan.
Methods and materials
A cross-sectional study was conducted in Jalalabad within May–June 2013. Multistage random sampling technique was used to enroll 1200 adults of 25–65 years. WHO STEP wise approach used to collect data on demographic and behavioral factors. Physical measurement including height, weight and blood pressure was collected and blood samples were drawn in fast condition for biochemical measurements including blood lipids. Obesity was defined and categorized using body mass index. Descriptive and inferential analyses were performed using SPSS v.20.
Results
The overall prevalence of obesity was 27.4% with significant difference between sexes (35.9% females and 16% males). The mean age was 38.76 ± 11.06 years with 60% female, 71.5% illiterate and 6.3% of smokers. Average total cholesterol, high density lipoprotein, low density lipoprotein, and total glycerides were 198.8 mg/dL, 39.2 mg/dL, 122.9 mg/dL and 186.1 mg/dL respectively. Age, sex, education status, use of mouth snuff, rice as a meal, nature of job, diabetes and high blood pressure were significantly associated with obesity.
Conclusion
Approximately one third of adult population in Jalalabad city is suffering from obesity which is a cause of concern. Blood lipid profile is either borderline or more than average among study participants which could contribute to non-communicable diseases. Measures such as raising awareness and lifestyle modifications may help to reduce the burden of obesity among Jalalabad adults.
1 Introduction
Obesity has become a major global health challenge due to established health risks and substantial increases in prevalence.Citation1 Being a complex condition it contributes to burden of chronic diseases by affecting virtually all ages and socioeconomic groups.Citation2 In 2010, overweight and obesity were estimated to cause 3.4 million deaths, 4% of years of life lost, and 4% of disability-adjusted life-years (DALYs).Citation3 Worldwide, the proportion of adults with a body mass index (BMI) of 25 kg/m2 or greater increased between 1980 and 2013 from 28.8% to 36.9% in men, and from 29.8% to 38.0% in women.Citation1 In developed nations obesity is related inversely to socioeconomic status (SES) affecting disadvantage group.Citation4 In contrast in developing economies, overweight and obesity tend to affect more people from a high socioeconomic background.Citation5–Citation7 With the use of Indo-Asian-specific Basic Mass Index (BMI) cutoff values the prevalence of overweight and obesity was 25% and 10.3% respectively.Citation8 In the Eastern Mediterranean Region obesity and overweight have reached an alarming level. The prevalence of obesity among adolescents ranges from 15% to 45% with more occurrences in women versus men.Citation9 Moreover a systematic review of published papers between 1990 and 2011 showed that overweight and obesity in all age groups of the EMR countries range from 25% to 81.9%.Citation10 In an Iranian study the prevalence of overweight, obesity and pathologic obesity was 40%, 35% and 3% respectively.Citation11 Likewise the prevalence of overweight and obesity was found as high as 46.9% and 28.8% for males and 26% and 27% for females, respectively, in a survey in a relatively affluent country like Cyprus.Citation12 Using anthropometric measurement, the prevalence of obesity in the United States was found to be 30.5% in a survey conducted from 1999 to 2000 while in the United Kingdom, the prevalence is 23% among men and 24% among women.Citation13,Citation14
Many studies have identified different factors that could contribute to the prevalence of overweight and obesity which include greater age, being female, urban residence, being literate, socioeconomic status, intake of meat productsCitation8,Citation11; dietary habits, physical inactivityCitation9; nutrition transition, urbanization, marital status, a shorter duration of breastfeeding, frequent snacking, skipping breakfast, a high intake of sugary beverages, an increase in the incidence of eating outside the home, long periods of time spent viewing television, high fat foodsCitation10; waist circumference, total serum cholesterol, low density lipoprotein, blood glucose, and triglycerides, lower levels of fruits and vegetables, exercised less time/day and smoke more cigarettes/dayCitation12 and more.
In Afghanistan, due to years of war and conflict, few studies have been conducted to estimate the burden of obesity in the country. Overweight and obesity in age group of boys < 20 years, men ⩾ 20 years, girls < 20 years, and women ⩾ 20 years are estimated to be 18.5%, 49.2%, 19.5%, and 42.6%, respectively, while the obesity alone in same age groups is estimated to be 6.8%, 14.8%, 4.4%, and 13.8% respectively.Citation1 A study in Badghis province of Afghanistan in 2002 showed that the prevalence of obesity and overweight in female age group of 15–49 years was 1.8% and 11.5% respectively while the mean BMI was 21.1 kg/meter square.Citation15 In a study in 1997 in children less than 3 years it was showed that the proportion of overweight was 4%,Citation16 however, according to anecdotal reports of clinicians in Kabul the number of people with obesity is increasing day by day. Currently in Afghanistan, there is lack of reliable information on burden of non-communicable diseases including obesity, blood pressure, cancer, and diabetes due to high priority to infectious diseases while the country is suffering from double burden of diseases. The study may assist in estimating the burden of obesity and risk factors for adult population in Jalalabad city. The information provided will support strategic decisions and public health interventions to control and reduce risk factors and decrease the burden of disease. This study aims to determine the prevalence of obesity indicated by BMI and blood lipid profiles and its risk factors in Jalalabad city.
2 Methods and materials
WHO STEP wise approachCitation17 was adopted and conducted to determine the prevalence and associated factors for non-communicable diseases including blood lipids and obesity in Jalalabad city, Afghanistan. Jalalabad city is the capital of Nangarhar province located in eastern border of country. Our target population was adult individuals in age group of 25–65 years of both sexes and gave consent to participate. Temporary residents (less than six months) and those living in institutionalized settings along with insecure areas were excluded from the survey. After statistical calculation, totally 1200 subjects enrolled in the study. Data were collected during May–June 2013. All four clusters (A–D) and 20 sub-clusters of expanded program of immunization (EPI) were used for sample selection. The primary sampling unit (PSU) was sub-clusters, the secondary sampling units (SSU) were streets/areas, tertiary sampling units (TSU) were households and ultimate sampling units (USU) were respondent more than 25 years in the household. In cluster A, B, C and D the percentage of study population was 32%, 23%, 22% and 23% accordingly. Cluster A was more populated and more people are drawn but the actual number of population is not available. The interviewer was instructed to find a famous masjid as a fixed landmark or a very populated street within the boundaries of the selected location and following the bottle rotating rule proceed to series of households. In each household interviewer enumerated all persons who were eligible for our study based on inclusion criteria. The households with only one person meeting the eligibility criteria were the designated respondent. For households’ more than one person we wrote everyone names on a piece of paper before folding to look similar. Like lottery a member was asked to pick up a paper to select the designated respondent for this survey. The methods provide equal chance of being selected for each member of the households which fulfill the requirement of the survey. Structured and coded questionnaires were used to collect demographic, socioeconomic, clinical and behavioral information during interview. Bath scales were used for determining subjects’ body weight. A flexible measurement tape was used to measure height of participants. Height and weight measurements were used to calculate and categorize body mass index (BMI).Citation18 A tension measurement tape was used to measure the waist circumference in order to identify central obesity.Citation19 Cuff type sphygmomanometers were used to determine systolic and diastolic blood pressures and later on it was categorized as normal and high blood pressure.Citation20 We have developed operational definitions to categorize the risk factors in our study. Hypertension was diagnosed if systolic blood pressure was ⩾140 mm of Hg and/or diastolic pressure ⩾90 mm of Hg, or diagnosed cases taking antihypertensive drugs. Pre-hypertension is defined as 120–139 mmHg systolic blood pressure and/or 80–89 mmHg diastolic pressure. Overweight was defined as BMI 25–29.9 kg/m2, and obesity as BMI ⩾ 30 kg/m2. Individuals with a fasting blood sugar (FBS) of ⩾126 mg/dL were considered diabetic. Blood samples were collected following interview, next day for biochemical testing, keeping eight hours fast and transported in cold boxes regularly to laboratory section. Samples were processed by laboratory technicians and supervised by laboratory coordinator and serum separation followed the SOP developed by provincial and central laboratory technical team. After shipment of samples to the Central Public Health Laboratory (CPHL) in Kabul, they were stored at −80 °C until biochemical measurements were completed. Fasting blood sugar, triglycerides, cholesterols, and blood lipoproteins were measured and categorized. Diabetes Mellitus (DM) and hypertension were defined having a diagnosis of disease or receiving treatment. During fieldwork the people who were newly diagnosed as having hypertension or diabetes were informed by giving the results timely and in addition to health educations they were refereed to regional hospital in province for further management. Research protocol was approved by institutional review board (IRB) at Ministry of Public Health and informed consent was taken prior to interview. Data management and analysis were done using SPSS version 20.Citation21
3 Results
shows the socioeconomic and demographic characteristics of the study participants. The mean age (mean ± SD) of study subjects was 38.76 ± 11.06 years. Sixty percent were female and 71.5% were illiterate. Illiteracy was common in female (75%) as compared to male (25%). The study subjects were not eager to give information regarding their income, however just 11% had monthly income of more than 200 USD. Prevalence of cigarette smoking was 6.3% while using tobacco via mouth snuff (NASWAR) was 11%. The average number of fruits and vegetables servings per week was 2.93 ± 2 and 5.39 ± 2 respectively. After categorization of fruits and vegetables (serving per week) it was found that 29.4% of study subjects took three or more serving of fruits per week and 78.8 were taking three or more serving of vegetables per week. Around 51.9% of study participants were using solid fats in their kitchen for cooking which is almost double of liquid oil of 21.2%. Strong and moderate physical activity was 35.8% and 59.8% among study subjects. Approximately 35% spent three or more than three hours as sedentary daily. The prevalence of underweight, normal weight, overweight and obesity was 6.1%, 34.4%, 32.1% and 27.4% respectively. Furthermore 58.5% were centrally obese using waist circumference. The average BMI was 27.16 ± 6.87 kg per meter square (mean ± SD). The average height and weight were 159.51 cm ± 13.87 cm and 68.70 cm ± 15.12 cm respectively. shows the distribution of BMI values along with six categories by sex differentiation such as underweight, normal, overweight and obesity. The male group had significantly higher weights, heights and waist circumference while the mean BMI was significantly higher in female as compared to male. The level of LDL cholesterol and triglycerides was significantly different in male as compared to female. However the difference in the level of total cholesterol, HDL cholesterol and fasting blood sugar was not statistically significant by available data. The association of blood lipid with obesity is reflected in in which there is a significant association between total glycerides and obesity while the other types of lipids did not show significant association. The average serving of fruits consumptions daily, meat and chicken weekly, height and weight, systolic and diastolic blood pressures, BMI, triglycerides, total cholesterol, HDL cholesterol, and LDL cholesterol were significantly different among obese and non-obese subjects.
Figure 1 Graphic distribution of obesity categories by sex.
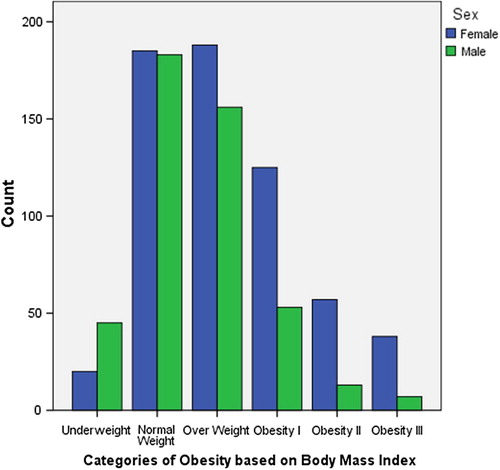
Table 1 Demographic and behavioral characteristics of study participants.
Table 2 Anthropometric measurements and lipid profile of study participants by obesity status.
The relationship between factors such as diet, anthropometric measurement, blood pressure, and lipid profile with obesity is reflected in . It shows odds of being obese were consistently higher as the age groups were increased. Females were 2.94 times more likely to be obese as compared to males (95% CI: 2.18–3.97) which shows sex variation in obesity. Illiterates were more likely to be obese as compared to literate (OR = 1.94, 95% CI: 1.41–2.68). We could not found significant association between cigarette smokers versus obesity while snuffers were less obese as compared to non-snuffers by a significant statistical association. Those who were taking more than three times rice per week were more likely to be obese (OR = 2.06, 95% CI: 1.41–3.01. Those who were obese had 1.9 (95% CI: 1.29–2.81) times more odds of being diabetic. In addition our study found significant relationship between obesity and physical activity in terms of job nature, blood pressure and triglycerides.
Table 3 Statistical analysis of risk/protective factors and obesity of study participants.
4 Discussion
High prevalence of overweight (32.1%) and obesity (27.4%) among the Jalalabad citizens was an important finding of our study. This prevalence of obesity among adult population is consistent with similar studies in other regions of the world which is clustered around 30%.Citation8 In addition blood lipid profile including total cholesterol and triglycerides is high among the sample study. It hypothesizes a question for further research to find the main reasons. Increasing age is affecting positively the association (level) of obesity at bivariate level. It seems the older are at greater risk of many non-communicable diseases including obesity and overweight. Likewise gender as non-modifying factors has relationship with obesity. It seems that women are at more risk of obesity as compared to men possibly due to low level of physical activity in the country. Similar results regarding age and gender are reported by the studies conducted in a number of Middle East countries such as Bahrain, Saudi Arabia, Lebanon and Pakistan.Citation22–Citation25 Due to low economic situation approximately two third of study participants are illiterate which is necessary to be taken into account while formulating health promotion messages. Education level is affecting obesity which means literate group are more health oriented and less likely to be obese as compared to illiterate. The relationship of tobacco use via mouth snuff with obesity is required to be studied more in future because using snuff was negatively affected level of obesity. Diabetes and blood pressure both were associated with obesity which shows the adult populations are suffering from different risk factors at the same time. It means that the country is already entered in epidemic of non-communicable diseases which requires strengthening efforts for its control and prevention. The significant association of obesity and blood pressure is well reported by other studies as well.Citation8 The more level of triglycerides was significantly associated with high level of obesity which make the person vulnerable to cardiovascular diseases. Screening for blood lipids as a measure could help in prevention of dyslipidemia and potential health diseases. Nature of job being more oriented to physical activity was a protective factor against obesity. This finding is consistent finding of other countriesCitation26–Citation28 as well as focus of World Health Organization (WHO) along with tobacco use, healthy diet and harmful use of alcohol. This study could not show significant association of diet, except using rice as a meal, and obesity but it has been proved by other studies elsewhere.Citation29
In nutshell it can be concluded that that obesity is a major public health problem that requires concerted interventions to be prevented and controlled. Unfortunately the country has not been able to defeat communicable diseases, however non-communicable diseases are another burden over the weak and donor driven health system. Particularly the coexistence of obesity, blood pressure and diabetes provides a persuasive basis to explain the specific factors that contribute to obesity and relationship between blood pressure, diabetes and obesity as well as other factors.Citation30 The findings obtained from this study can contribute in formulation of more advanced and national studies to have a generalized picture of non-communicable disease and their risk factors in the country. It is recommended that WHO should design a nationwide survey using STEP wise approach to provide representative data for making informed decisions by the government.
Conflict of interest
The authors have no conflict of interest to declare.
Acknowledgment
This study was supported financially by Ministry of Public Health and World Health Organization. WHO and Afghan National Public Health Institute are thanked for their financial and technical guidance. In addition we would like to thank all our technical supervisors, data collectors, and study participants for their guidance and support to this study.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 16 January 2015
References
- Marie Ng et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. <http://www.thelancet.com> [published online 29.05.14] http://dx.doi.org/ 10.1016/S0140-6736(14)60460-8.
- WHO. Global strategy on diet, physical activity and health. Geneva: World Health Organization; 2004. <http://www.who.int/dietphysicalactivity/en/> [accessed 18.08.13].
- S.S.LimT.VosA.D.FlaxmanA comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010Lancet380201222242260
- B.A.SwinburnG.SacksK.D.HallK.McPhersonD.T.FinegoodM.L.MoodieThe global obesity pandemic: shaped by global drivers and local environmentsLancet3782011804814
- M.J.FriedrichEpidemic of obesity expands its spread to developing countriesJAMA287200213821386
- K.S.ReddyS.YusufEmerging epidemic of cardiovascular disease in developing countriesCirculation971998596601
- L.FezeuE.MinkoulouB.BalkauA.P.KengneP.AwahN.UnwinAssociation between socioeconomic status and adiposity in urban CameroonInt J Epidemiol352005105111
- T.H.JafarN.ChaturvediG.PappasPrevalence of overweight and obesity and their association with hypertension and diabetes mellitus in an Indo-Asian populationCMAJ1759200610711077
- A.O.MusaigerOverweight and obesity in the Eastern Mediterranean Region: can we control it?Eastern Mediterr Health J1062004
- A.O.MusaigerOverweight and obesity in eastern mediterranean region: prevalence and possible causesJ Obesity201111710.1155/2011/407237
- G.R.VeghariM.SedaghatH.R.JoshaghaniA.HoseiniF.NiknezhadA.H.AngizehThe prevalence of obesity and its related risk factor in the North of Iran in 2006JRHS1022010116121
- E.AndreouP.G.HajigeorgiouK.KyriakouT.h.AvraamG.ChappaP.KallisRisk factors of obesity in a cohort of 1001 Cypriot adults: an epidemiological studyHIPPOKRATIA1632012256260
- K.M.FlegalM.D.CarrollC.L.OgdenC.L.JohnsonPrevalence and trends in obesity among US adults, 1999–2000JAMA288200217231727
- British Heart Foundation: Diet, Physical Activity and Obesity Statistics.; 2006 <http://www.heartstats.org/datapage.asp?id=5749> [accessed 22.02.13].
- Nutrition and Health Survey, Badghis Province, Afghanistan, February–March; 2002 (IB Ref: 101440a1).
- M.de OnisM.BlossnerPrevalence and trends of overweight among preschool children in developing countriesAm J Clin Nutr724200010321039
- R.BonitaM.de CourtenT.DwyerK.JamrozikR.WinkelmannSurveillance of risk factors for non-communicable disease: the WHO STEP wise approach2002World Health OrganizationGeneva WHO document WHO/NMH/CCS/01.2002.
- World Health Organization. Obesity: preventing and managing the global epidemic. Geneva: World Health Organization; 2000 (WHO Technical Report Series No.894).
- International Diabetes Federation: The IDF consensus worldwide definitions of the metabolic syndrome. <http://www.idf.org/webdata/docs/IDF_Meta_def_final.pdf>; 2006.
- J.A.WhitworthWorld Health Organization (WHO)/International society of Hypertension (ISH) statement on management of hypertensionJ Hypertens21200319821992
- IBM SPSS Statistics for Windows [computer program]. Version 20.0. Armonk, NY: IBM Corporation; 2011.
- B.M.YalcinE.M.SahinE.YalcinPrevalence and epidemiological risk factors of obesity in TurkeyMiddle East J Family Med662004
- A.O.MusaigerM.A.Al-MannaiWeight, height, body mass index and prevalence of obesity among the adult population in BahrainAnn Hum Biol.282001346350
- A.A.Al-NuaimE.A.BamgboyeK.A.al-RubeaanY.al-MazrouOverweight and obesity in Saudi Arabian adult population, role of sociodemographic variablesJ Community Health2231997211223
- A.M.SibaiN.HwallaN.AdraB.RahalPrevalence of and covariates of obesity in Lebanon: finding from the first epidemiological studyObes Res11200313531361
- L.AzadbakhtP.MirmiranN.ShivaF.AziziGeneral obesity and central adiposity in a representative sample of Tehranian adults: prevalence and determinantsInt J VitamNutr Res7542005297304
- J.L.Gutierrez-FisacP.Guallar-CastillonL.Diez- GananE.Lopez GarciaJ.R.BanegasF.Rodriguez ArtalejoWork- related physical activity is not associated with body mass index and obesityObes Res102002270276
- M.Lahti-KoskiP.PietinenM.HeliovaaraE.VartiainenAssociation of body mass index and obesity with physical activity, food choices, alcohol intake and smoking in the 1982–1997Am J Clin Nutr752002809817
- Khwaja Mir IslamSaeedPrevalence of risk factors for non-communicable diseases in the adult population of urban areas in Kabul City, AfghanistanCent Asian J Glob Health22201310.5195/cajgh.2013.69 http://cajgh.pitt.edu
- C.D.BrownM.HigginsK.A.DonatoF.C.RohdeR.GarrisonE.ObarzanekBody mass Index and prevalence of hypertension and dyslipidemiaObes. Res.82000605619