
Abstract
Objective
The aim of this study was to evaluate the role of ultrasound in early diagnosis of intra-abdominal injury following blunt abdominal trauma and follow up in patients with intra-abdominal injury for detecting late complications.
Materials and methods
120 patients who presented to the emergency room were evaluated by Focused abdominal sonography for trauma (FAST) and follow-up sonography was done after 12–24 h.
Results
This study found FAST to be 93% sensitive and 99% specific.
Conclusion
Ultrasonography is considered the best modality in initial evaluation of blunt abdominal trauma patients as it is noninvasive, readily available, and requires minimal preparation time. Ultrasonography is very useful in follow up of patients with intra-abdominal injury and decreases use of CT which has the disadvantages of being expensive, high dose radiation.
1 Introduction
Trauma is one of the most common causes of death in the young population (age group between 1 and 45 years). Blunt abdominal trauma (BAT) is very common, and the prevalence of intra-abdominal injury following it has been reported to be as high as 12–15%. The mechanisms resulting in BAT were motor vehicle collision (73%), motorcycle collision (7%), auto-pedestrian collision (6%), and fall (6%).Citation1
Rapid diagnosis of abdominal injury is an important step in the treatment process to prevent morbidity or mortality in BAT cases. Rapid determination of cases in need of emergency laparotomy is crucial for life saving, especially for those with unstable hemodynamics, the avoidance of unnecessary surgeries with its invasiveness and complications should be considered.Citation2
Ultrasonography (US) is the first imaging method for screening patients with blunt abdominal trauma. It can demonstrate variety of post traumatic abdominal organ pathologies including hematomas, contusions, lacerations, and hemoperitoneum.Citation2
Clinical examination and focused abdominal ultrasonography comprise the standard initial abdominal evaluation in post trauma patients. Clinical observation following BAT is a common procedure in all hospitals; however, the required period for observation remains controversial, some suggested that 24 h is sufficient, while others reported minimum of an 8-h observation as a sufficient time to identify injuries among hemodynamically stable patients.Citation3
This study aims to assess the role of focused sonography in early diagnosis of intra-abdominal injuries following blunt abdominal trauma and follow up in patients with intra-abdominal injury for early diagnosis of complications.
2 Materials and methods
The study was conducted at the Radiodiagnosis Department, Ain Shams University on 120 patients who presented to the emergency room (ER) with blunt abdominal trauma during the period between April 2012 to August 2013.
2.1 Patient preparation
No preparation was done, and the patient was sent directly from the ER to the radiodiagnosis Department.
2.2 Ultrasound scanning
All examinations including the follow up studies were conducted by the same radiologist (first author) who has 15 year experience in ultrasonography using ultrasound machine Esaote My lab 70 XVG with a 3.5 MHz curved array transducer.
2.3 Scanning technique
The patients were placed supine. Focused abdominal sonography for trauma (FAST|) was performed, which takes no more than 5 min, the following four standard views should be obtained:
| (a) | Epigastric region transverse views to assess the left lobe of the liver. | ||||
| (b) | Right hypochondrium longitudinal views to assess the right lobe of the liver, the right kidney, and the Morison pouch. | ||||
| (c) | Left hypochondrial longitudinal views to assess the left kidney, the spleen, and the lienorenal space. | ||||
| (d) | Suprapubic transverse and longitudinal views to assess the urinary bladder and Douglas pouch. | ||||
In addition to these four views, right and left longitudinal views of the lower thoracic cage are acquired to rule out pleural effusion.
2.4 Follow up
Ultrasonography was performed after 12–24 h except 3 cases who had severe intra-abdominal hemorrhage and entered the operation room urgently after FAST examination.
Contrast enhanced computed tomography (CECT) was done in FAST positive cases except those who were hemodynamically unstable or sent directly to the operation room.
Ultrasonography findings were correlated with patient’s clinical and operative data.
3 Results
The study included 120 patients (110 males and 10 females) presented to the ER by blunt abdominal trauma, 105 were due to car accident, 10 due to fight, 5 due to fall from height.
The mean age of the patients was 28 years (range 11–65 years). The most commonly affected group was between 15 and 35 years (69% of patients).
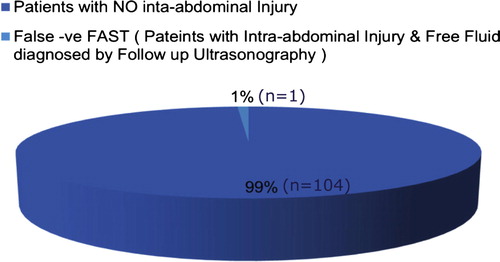
Out of the 120 patients only 15 had +ve FAST at time of presentation. Out of the 105 patients with −ve FAST, only one case had false −ve FAST (), small upper pole splenic hematoma and moderate pelvic free fluid were recognized in the follow up ultrasonography done 12 h later, the patient’s hemodynamic condition was deteriorating progressively, and splenectomy was done.
Figure 1 Patients with false negative FAST.
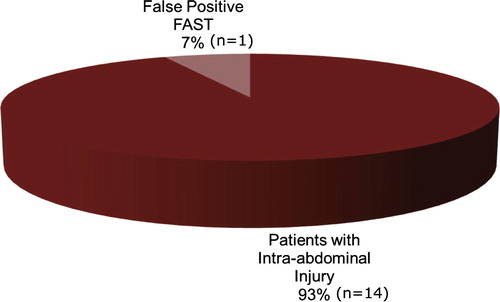
Out of the 15 patients with +ve FAST, only one case was false +ve FAST (), the patient had ascites due to renal impairment, both kidneys showed grade 2 nephropathy and no gross organ injury is detected by ultrasonography or Contrast Enhanced Computed Tomography (CECT).
Figure 2 Patients with false positive FAST.
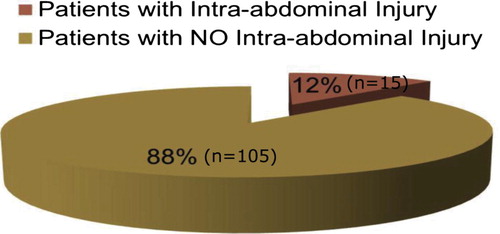
Out of the 120 patients presented by Blunt Abdominal trauma, 15 patients had Intra-abdominal Injury ().
Figure 3 Patients with blunt abdominal trauma.
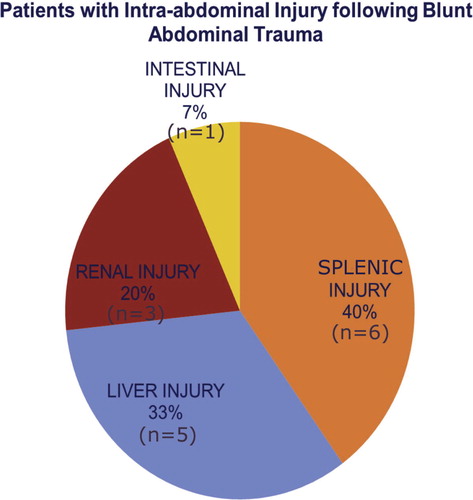
Out of the 15 patients with intra-abdominal injury, 5 patients had liver injury, 6 patients had splenic injury, 3 patients had renal injury and one patient had intestinal injury ().
Figure 4 Types of intraabdominal injuries.
4 Discussion
Trauma is one of the common causes of death, and is a major economic and health problem. The abdomen is the third most common injured region, in 25% of cases who require surgical interference. Abdominal trauma is classified as either blunt or penetrating. Penetrating abdominal trauma is easily diagnosed, while blunt trauma complications can be missed if the clinical signs are not evident.Citation4
Hemodynamic instability, disturbed level of consciousness and presence of other injuries in the skull, chest, pelvic bones or extremities, all explain the need of an accurate and rapid imaging tool to diagnose associated abdominal visceral injuries.Citation5
Contrast enhanced computed tomography (CT) is the radiological golden standard for abdominal visceral injuries. However, renal failure or a previous anaphylactic reaction to contrast material hinders the use of CT in evaluation of some trauma patients. A noncontrast study diminishes the sensitivity of CT in diagnosis of solid organ injuries.Citation6
CT disadvantages include the need for patient transfer to the CT unit, hazards of ionizing radiation or if contrast media is used, patients may not be co-operative or assume the best position if in pain or with disturbed conscious level. Thus, non-elevated arms, or medical devices (catheters, tubes and lines) will cause artifacts decreasing imaging quality.Citation7
Organ injury can be easily diagnosed by abdominal ultrasound as well as the presence of free intra-abdominal fluid, which could be blood or intestinal secretions, that provides indirect evidence of these injuries. Ultrasound is non-invasive, portable using no ionizing radiation, repeatable, and easily performed in the emergency unit, at the same time with resuscitation methods. Focused abdominal sonography for trauma (FAST) is a fast examination method that could demonstrate intraperitoneal fluid. Several studies found this technique to be sensitive (79–100%) and specific (95.6–100%), particularly in hemodynamically unstable patients.Citation8
Our study found FAST to be 93% sensitive and 99% specific, only one case was false −ve FAST, moderate pelvic fluid collection and very small subcapsular splenic hypoechoic area less than 1 cm were seen in the follow up ultrasonography done after 12 h. However, the patient was hemodynamically deteriorating with progressive decrease in vital data, and exploration and splenectomy were done. Only one case had false +ve FAST, the patient had ascites due to renal impairment, repeated ultrasonography after 12 h showed no increase in the amount of intra-peritoneal fluid or organ injury and the patient was hemodynamically stable.
Our study showed that 40% of cases with intra-abdominal injury had splenic injury (), 33% had hepatic injury (), 20% had renal injury () and 7% had intestinal injury ().
Figure 5 Male patient 26 years old presented to the ER with blunt abdominal trauma following fight. FAST examination performed at the time of presentation showed; (a) Upper pole of the spleen iso to hypoechoic area measuring 1 cm in its maximum diameter (hematoma) and minimal free fluid at the splenorenal angle. (b) Minimal pelvic fluid collection. FAST examination performed after 12 h showed. (c) Upper pole of the spleen shows hypoechoic area 1 cm in its maximum diameter and minimal free fluid at the splenorenal angle. (d) No pelvic fluid collection. Findings of Splenic injury and disappearance of pelvic free fluid suggest stop of bleeding. Management was conservative.
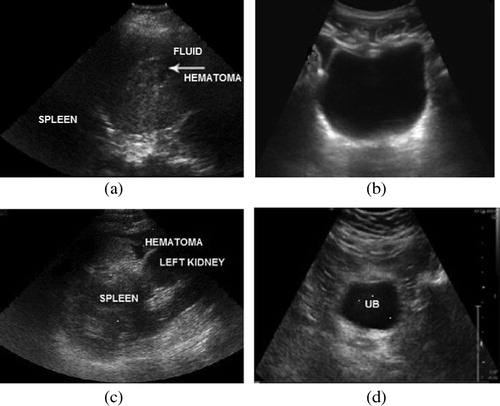
Figure 6 Male patient 25 years old presented to the ER with blunt abdominal trauma following car accident. FAST examination performed at the time of examination. (a) Right lobe of the liver subcapsular area of heterogenous echogenicity measuring 3 × 1 cm in maximum diameters (hematoma), perihepatic moderate free fluid. (b) Marked pelvic free fluid mainly at the right iliac fossa. FAST examination performed after 12 h. (c) The right lobe of the liver subcapsular hypoechoic area measuring 3 × 1 cm in maximum diameter and increased perihepatic free fluid. (d) Increased amount of pelvic free fluid. Findings of liver injury and increased intra-abdominal and intrapelvic fluid (suggesting active bleeding). Management: Surgical treatment.
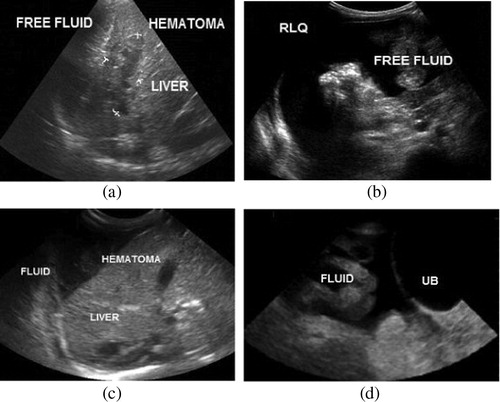
Figure 7 Male patient 55 years old presented to the ER with blunt abdominal trauma following Car accident. FAST examination performed at the time of presentation. (a) The right kidney showed hyperechoic area related to its anterior surface (mostly subcapsular) measuring 3 cm x 1 cm in its maximum diameter not reaching the renal medulla, minimal free fluid at the hepatorenal angle. (b) Minimal pelvic free fluid. FAST examination performed after 12 h. (c) The right kidney showed subcapsular hematoma of heterogenous echogenicity (less echogenic than in FAST) not reaching the renal medulla, decreased amount of free fluid at the hepatorenal angle. (d) Minimal pelvic free fluid. Findings of Right Renal injury and Decreased intra-abdominal and intrapelvic fluid (bleeding). Management: CECT, Conservative treatment.
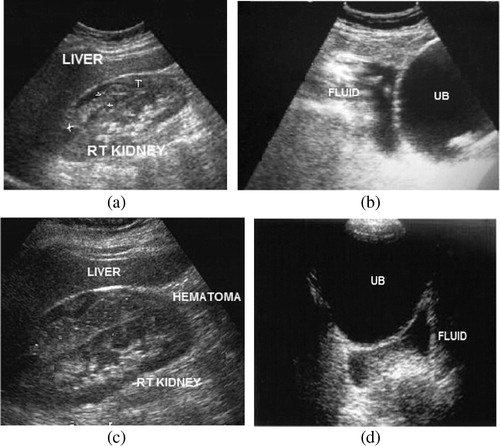
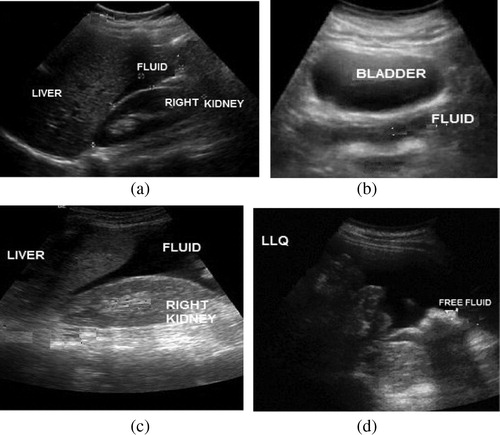
Figure 8 Male patient 35 years old presented to the ER with blunt abdominal trauma following car accident. FAST examination performed at the time of presentation. (a) Minimal free fluid at the hepatorenal angle, and (b) minimal pelvic free fluid. Findings of Positive FAST; however, no gross organ injury is detected. FAST examination performed after 12 h. (c) Increased free fluid at the hepatorenal area. (d) Increased pelvic free fluid. Findings suggestive of active intra-abdominal bleeding and organ injury; however, no gross organ injury is detected. Management: CECT abdomen and pelvis were performed just after FAST examination, and CECT revealed intestinal injury. Sigmoid colostomy was done.
Lee et al.Citation9 claimed that hypotensive patients screened in the emergency department with positive FAST findings may be transferred directly to laparotomy, depending on the results of the sonography examination, without the need for CT. In our study, 3 patients underwent laparotomy after FAST examination and the 3 patients had severe intra-abdominal hemorrhage and hypotension. One of them was 3 year old female with severe left renal lacerations and perirenal hematoma and marked pelvi-abdominal free fluid following car accident, and left total nephrectomy was performed. Another case was 25 year old male patient with large hematoma involving the lower pole and middle parts of the right kidney and marked abdominopelvic free fluid, the patient entered the operation room urgently after FAST examination for total right nephrectomy. The third case was 13 year old male patient with severe splenic lacerations and rupture, marked abdominopelvic free fluid, the patient entered the operation room urgently after FAST examination for splenectomy.
CT is not an option for patients who are clinically unstable to be transferred to the CT unit, pregnant females, patients with large body habitus. Sonography has some advantages over CT in trauma cases, it is a bedside, fast, reliable one and it uses no ionizing radiation. Furthermore, there is no use of iodinated contrast agents avoiding the associated risk of contrast reaction or nephrotoxicity.Citation10
Patients with small splenic or hepatic injuries who were hemodynamically stable do not need further investigations and are treated conservatively. Patients with major splenic or hepatic injuries and who are hemodynamically stable could perform CT abdomen for accurate characterization of their injuries. Jalli et al., suggested that CT scan is the modality of choice in hemodynamically stable patients who have major suspicions for renal injuries.Citation10
In cases of renal trauma, the exact extent of injury should be assessed for accurate therapy choice. Tears that expand into or through the pelvi-calyceal system (grade IV and higher) and ureteric injuries are not very obvious on sonography if there is no significant urinary leakage. Delayed contrast-enhanced CT performed 10 min after contrast injection can easily show extravasation from the pelvi-calyceal system or the ureters and, thus, delineate the location and extent of damage.Citation11
In our study, 3 cases of renal injury were reported, one of them had large renal hematoma, marked intra-abdominal bleeding and hemodynamic instability that urgent exploration and left total nephrectomy were done, the other 2 cases were hemodynamically stable, one of them had subcapsular hematoma while the other had perinephric hematoma and renal laceration; however, ultrasonography could not detect the exact extension of the injury and could not exclude injury of collecting system, CECT was performed, and the case of subcapsular hematoma was treated conservatively while the other case needed surgical treatment. In a study done by Sato and Yoshii,Citation12 they reported that ultrasonography was found to detect and classify parenchymal injuries efficiently, when done by experienced examiners despite disadvantages in detecting superficial and vascular injuries.
In our study, there was one case of intestinal injury, ultrasonography just detected the intra-peritoneal free fluid, injury could not be seen and CT abdomen with contrast was done and detected intestinal injury. In patients with negative initial FAST but sustained abdominal symptoms, repeated sonography after 12 to 24 h can facilitate a diagnosis of gastrointestinal tract injury.Citation2 Lee et al., reported that, bowel and mesenteric injuries are not associated with a significant amount of abdominal free fluid in hypotensive patients and may cause false-negative results on FAST; clinical follow up and CT scanning should be considered to prevent this probability.Citation9
5 Conclusion
Ultrasonography can be considered the initial imaging modality in evaluation of blunt abdominal trauma patients; it is noninvasive, readily available, and requires minimal preparation time. Hepatic lacerations or hematomas, pancreatic and gastrointestinal injuries are difficult to see by ultrasonography; however, presence of intra-abdominal fluid (positive FAST) suggests intra-abdominal injury, so CECT should be performed. Repeated ultrasonography in patients of blunt abdominal trauma and close clinical observation increases the sensitivity of ultrasonography for intra-abdominal bleeding to nearly 100%.
6 Conflict of interest
None declared.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 28 February 2015
References
- J.L.KendallA.M.KestlerK.T.WhitakerM.M.AdkissonJ.S.HaukoosBlunt abdominal trauma patients are at very low risk for intra-abdominal injury after emergency department observationWest J Emerg Med1242010496504
- A.MohammadiM.Ghasemi-RadEvaluation of gastrointestinal injury in blunt abdominal trauma “FAST is not reliable”: the role of repeated ultrasonographyWorld J Emerg Surg7120122
- C.L.TsuiH.T.FungK.L.ChungC.W.KamFocused abdominal sonography for trauma in the emergency department for blunt abdominal traumaInt J Emerg Med12008183187
- M.A.GadA.SaberS.FarragM.E.ShamsG.M.EllabbanIncidence, patterns, and factors predicting mortality of abdominal injuries in trauma patientsN Am J Med Sci432012129134
- S.FarrathJ.G.ParreiraJ.A.PerlingeiroS.C.SoldaJ.C.AssefPredictors of abdominal injuries in blunt traumaRev Col Bras Cir3942012295301
- T.L.HedrickR.G.SawyerJ.S.YoungMRI for the diagnosis of blunt abdominal trauma: a case reportEmerg Radiol1152005309311
- D.CokkinoE.AntypaK.StefanidisP.TserotasV.KostarasContrast-enhanced ultrasound for imaging blunt abdominal trauma – indications, description of the technique and imaging reviewUltraschall Med33120126067
- J.O.JansenS.R.YuleM.A.LoudonInvestigation of blunt abdominal traumaBMJ33676502008938942
- B.C.LeeE.L.OrmsbyJ.P.McGahanG.M.MelendresJ.R.RichardsThe utility of sonography for the triage of blunt abdominal trauma patients to exploratory laparotomyAJR18822007415421
- R.JalliN.KamalzadehM.LotfiS.FarahangizM.SalehipourAccuracy of sonography in detection of renal injuries caused by blunt abdominal trauma: a prospective studyUlus Travma Acil Cerrahi Derg15120092327
- M.KornerM.M.KrotzC.DegenhartK.J.PfeiferM.F.ReiserU.LinsenmaierCurrent role of emergency US in patients with major traumaRadioGraphics282008225242
- M.SatoH.YoshiiReevaluation of ultrasonography for solid-organ injury in blunt abdominal traumaJUM2312200415831596