
Abstract
Background
Urinary tract injuries occur in 3–10% of abdominal trauma, kidneys being the most commonly injured. Contrast-enhanced CT is the imaging technique of choice for renal trauma, since it can quickly and accurately demonstrate not only renal injuries, and also associated damage to other organs. CT can help detect active hemorrhage and urine leakage and is the most accurate screening test for high-grade injuries and is of great help in guiding transcatheter embolization and delineating preexisting disease entities.
Aim of the work
To demonstrate different traumatic lesions of the kidneys using multi-detector CT, and its use in staging and management of lesions.
Methods
Study was carried out on 41 patients with abdominal trauma and suspected renal injury. All patients were subjected to contrast-enhanced multiphasic renal CT study in correlation with surgical and conventional angiography data when available.
Results
All patients were classified after the American Association for the Surgery of Trauma grading system. Grade I injury was diagnosed in 2.4% of patients, grade II in 7.3%, grade III in 29.3%, grade IV in 53.7% and grade V in 7.3%. 80.5% of patients were managed conservatively, 12.2% of patients underwent total nephrectomy and 7.3% of patients died before management.
Conclusion
Multiphasic CT well demonstrated various traumatic renal lesions with proper diagnosis and staging of renal trauma and guiding management.
Abbreviations:
- AAST
- American Association for the Surgery of Trauma
- A-V fistula
- arterio-venous fistula
- CECT
- Contrast-Enhanced Computed Tomography
- CT
- computed tomography
- FAST
- Focused Assessment with Sonography in Trauma
- MDCT
- multi-detector computed tomography
- MPR
- Multi-Planar Reformatted
- RTRS
- Renal Trauma Risk Score
- VRT
- volume rendering technique
1 Introduction
Injuries to the urinary tract occur in 3–10% of abdominal trauma, and in these patients, the kidneys are the most commonly injured organ.Citation1–Citation4 About 80–90% of the urinary tract injuries occur due to blunt abdominal trauma,Citation2 and may be associated with injury to other major organs.Citation2,Citation3
Multi-detector computed tomography (MDCT) with IV contrast has been considered as the imaging technique of choice for the evaluation of renal trauma, especially that it is widely available in emergency units and is highly sensitive to demonstrate both the urinary tract injuries and also the associated extra-urinary injuries.Citation5,Citation6 Renal injury is the result from blunt or penetrating trauma to the back, flank, lower thorax, or upper abdomen.
Nowadays, the most widely accepted and used classification system for renal injuries is the American Association for the Surgery of Trauma (AAST) grading system.Citation1,Citation2,Citation6 This system is based on surgical findings (the standard for renal injury staging).
Renal trauma is divided into five categories (grades I–V), according to the severity and depth of injury and involvement of the vasculature or collecting system.Citation1
Grade I injuries are the most common type of renal injury (75–85% of cases)Citation7,Citation8 and include hematuria with no structural abnormalities, parenchymal contusions, and nonexpanding subcapsular hematomas.Citation3
Grade II renal injuries include perinephric hematomas and superficial cortical lacerations measuring less than 1 cm in depth. Grade III injuries include renal lacerations deeper than 1 cm extending into the medulla. In both grade II and grade III lacerations, the collecting system is intact.Citation1
Grade IV injuries include renal lacerations involving the collecting system, injuries to the main renal artery or vein, and segmental infarctions.Citation9
Grade V injuries are the most severe renal trauma that include shattered kidney, partial or complete laceration (avulsion) of the ureteropelvic junction, and thrombosis of the main renal artery or vein.Citation1
In addition to injury grade, another 3 primary radiographic features of the injured kidney are recorded as potential renal trauma risk factors, including (1) perirenal hematoma size (perirenal hematoma rim distance (PRD) 3.5 cm or greater), (2) intravascular contrast extravasation in the perirenal hematoma and (3) the site/complexity of lacerations in the parenchyma.Citation10
Patients are substratified by the number of these radiographic risk factors, Renal Trauma Risk Score (RTRS), into low risk group (grade 3 or 4a) with 0 or 1 risk factors and high risk group (grade 4b) with 2 or 3 risk factors.Citation10
The widespread use of CT has resulted into more conservative management of renal trauma, except in cases in which extensive urinary extravasation or devitalized areas of renal parenchyma are found and in those cases with associated severe injuries to other abdominal organs with high liability to complications and hence require surgery.Citation9
2 Aim of the work
In this study we aimed to demonstrate different traumatic lesions of the kidneys using multi-detector CT, and its use in staging and management of lesions
3 Methods and materials
The study was carried out on 41 patients with blunt and penetrating abdominal trauma with suspected renal injury; referred to the Radiodiagnosis Department at Alexandria Main University Hospital.
3.1 Inclusion criteria
| (1) | Positive FAST examination for intraperitoneal or perinephric collection. | ||||
| (2) | Gross hematuria. | ||||
| (3) | Negative FAST examination and hypotension (systolic blood pressure <90 mmHg). | ||||
| (4) | All penetrating injuries to the abdomen, flank, or lower thorax. | ||||
3.2 Exclusion criteria: Severely shocked patients who could not be transported to CT unit
All patients included in the study were subjected to the following:
| 1. | Thorough history taking including mode of injury and present complaint e.g. abdominal pain, hematuria, etc. | ||||||||||||||||
| 2. | Full clinical examination including:
| ||||||||||||||||
| 3. | FAST sonographic assessment. | ||||||||||||||||
| 4. | Contrast-enhanced multiphasic renal CT study with correlation with surgical and conventional angiography data whenever available. | ||||||||||||||||
CT was performed using six detectors CT Somatom Emotion 6 (Siemens, Germany), and 16 detectors PHILIPS MX16 (Philips, Holland).
3.3 Imaging protocol
| (1) | Initial nonenhanced study was obtained for the whole abdomen to detect acute bleeding or intraparenchymal hematoma that may become isoattenuating relative to the normal renal parenchyma at postcontrast CT. | ||||
| (2) | Arterial phase 25 s after initiation of contrast injection of meglumine ioxitalamate 350 mgl/ml (Telebrex 35, Amoun Pharmaceuticals, Egypt) using a power injector (Medrad, Vistron CT) at the rate of 4–5 ml per second through an 18 gauge venous cannula to detect arterial injuries. | ||||
| (3) | Venous phase 45 s after injection to detect venous injuries. Both the arterial and venous phases are restricted to the renal regions as determined by non-contrast scans. | ||||
| (4) | Nephrographic phases (70–90 s) including the whole abdomen for renal parenchymal and other organs injuries. | ||||
| (5) | 5 min delayed scan of the whole abdomen was obtained to detect pelvicalyceal system injury and urinary extravasation. | ||||
3.4 Grading of injuries was performed according to the last modification of AAST grading system as published in Dayal et al.Citation11
In case of multiple injuries within the same kidney, grading is according to the highest injury.
3.5 Informed consent was obtained from all patients, with their privacy guaranteed
Informed consent was obtained from all patients, with their privacy guaranteed.
4 Results
The study was carried out on 41 patients with blunt and penetrating abdominal trauma and suspected renal injury. Thirty-six patients (87.8%) were males and five patients (12.2%) were females. The age of patients ranged from 4 years up to 66 years with a mean age of 27.83 years.
summarizes the types of trauma encountered in the study.
Table 1 Distribution of patients according to types of trauma.
Thirty-eight patients (92.7%) complained of abdominal pain, 35 patients (85%) presented with gross hematuria and six patients (14.6%) were shocked.
Twelve patients (29.3%) had isolated renal injury while 29 patients (70.7%) had other associated injuries as demonstrated in . Liver lacerations were the most associated organ injuries, found in 11 patients (26.8%).
Table 2 Other injuries associated with renal injury.
demonstrates different renal injury detected in the present study.
Table 3 Demonstration of different CT findings of renal injury that were detected in the present study.
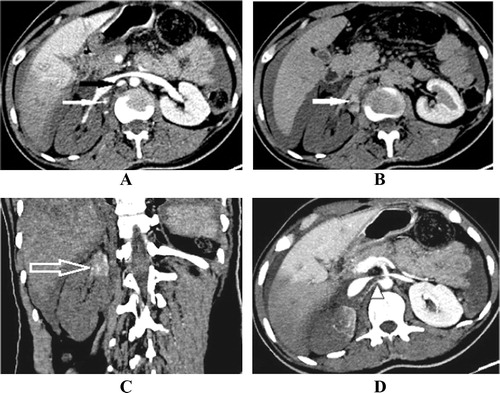
Regarding the AAST grading system, Grade I injury was diagnosed in five patients (14%) with small contusion without laceration or perinephric hematoma (n = 2) () and was managed conservatively, .
Figure 1 Twenty-seven year old male patient who sustained blunt trauma in a road traffic accident (A) axial contrast enhanced computed tomography (CECT) venous phase shows small contusion at the lower pole of the right kidney (white arrow) without associated perinephric hematoma (grade I renal injury). (B) Axial image at a higher level shows liver lacerations and contusions (black arrow) with free intraperitoneal collection (hemoperitoneum) (asterisk).
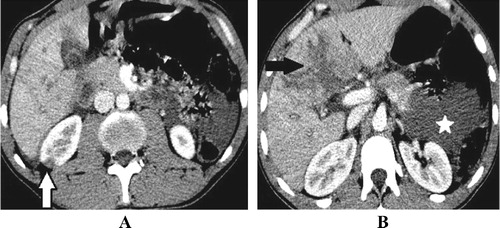
Table 4 Distribution of patients according to AAST grading and their management.
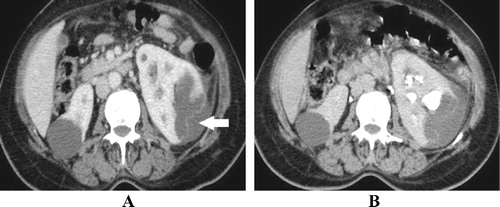
Grade II injury was diagnosed in three patients (7.3%), one of them had laceration (<1 cm), the second had ruptured cortical cyst () and the third had laceration (<1 cm) and hemorrhagic cortical cysts; all of them were managed conservatively.
Figure 2 Fifty-five year old female patient who sustained blunt trauma in a road traffic accident. (A) Axial CECT nephrographic phase, (B) axial delayed phase showing multiple bilateral pre-existing simple cortical cysts with ruptured left sided midzonal cortical cyst (solid arrow) not reaching the collecting system with minimal perinephric collection (grade II renal injury).
Grade III injury was diagnosed in 12 patients (29.3%), all of them had deep laceration (>1 cm) not reaching the collecting system as proven by the absence of contrast extravasation in the delayed phase ( and ); all of them were managed conservatively by follow-up.
Figure 3 Eighteen year old male patient who suffered gunshot. (A) Axial CECT nephrographic phase shows inlet of the bullet (solid white arrow). (B) Axial image at the level of DV12 shows deep midzonal right renal laceration (solid black arrow) (>1 cm) not reaching the collecting system (proved by the absence of contrast extravasation in the delayed phase, not shown), grade III renal injury. Also noted perinephric hematoma (open arrow) and hepatic laceration (black asterisk). (C) Axial image at the level of basal chest shows bilateral pulmonary contusions (white asterisk), right pleural collection (black arrow) and exit of the bullet (white arrow). (D) Axial cut with bone window shows fracture posterior arch of DV12 (solid white arrow) with intrathecal air.
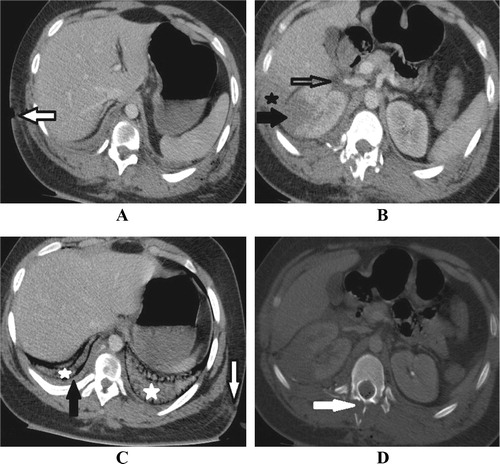
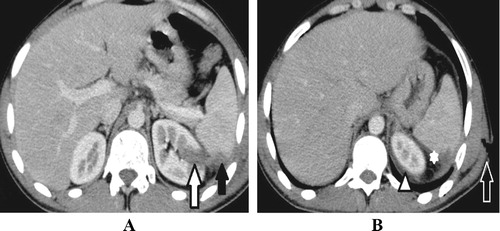
Figure 4 Twenty-three year old male patient who sustained stab injury. (A) Axial CECT venous phase shows left renal upper polar deep laceration (white arrow) (>1 cm) not reaching the collecting system (proved by the absence of contrast extravasation in the delayed phase, not shown), grade III renal injury, with splenic laceration (black arrow). (B) Axial cut at a higher level shows perinephric (arrow head) and perisplenic (asterisk) hematomas. The open arrow points to entry site of the stab.
Grade IV injury was diagnosed in 22 patients (53.7%):
| • | Ten patients (24.4%) had deep lacerations reaching the pelvicalyceal system proved by contrast extravasation in the delayed phase (). Eight patients were managed conservatively by follow-up, one patient underwent total nephrectomy and another one who was complicated by pseudoaneurysm and arteriovenous fistula formation was managed by angiographic embolization (). | ||||
| • | One patient (2.4%) had fractured kidney associated with pelvicalyceal system injury and contrast extravasation in the delayed phase and was managed conservatively by follow-up which revealed urinoma that was aspirated. | ||||
| • | Two patients (4.9%) had pelvic tear proved by contrast extravasation from the renal pelvis at the delayed phase without associated renal lacerations, one of them had pre-existing congenital pelviureteric junction obstruction and was managed by total nephrectomy while the other patient died before management due to brain injury. | ||||
| • | One patient (2.4%) had incomplete pelviureteric junction avulsion that was managed conservatively by double J insertion and follow-up. | ||||
| • | One patient (2.4%) had segmental lower polar infarction with other small subsegmental infarcts with neither renal laceration nor perinephric hematoma and was managed conservatively by follow-up. | ||||
| • | Three patients (7.3%) had shattered kidney that was associated with pelvicalyceal system injury in two patients who were managed conservatively by follow-up and active bleeding with pseudoaneurysm formation in the 3rd patient () who died before management due to hypovolemic shock. | ||||
| • | One patient (2.4%) had expanding subcapsular hematoma with active bleeding within the hematoma and was managed conservatively by follow-up. | ||||
| • | Three patients (7.3%) had vascular injury as follows: two patients had tear of the renal vein associated with IVC tear and multiple deep lacerations; one of them underwent total nephrectomy and the other was managed conservatively by follow-up due to hemodynamic stability, the 3rd patient had avulsed segmental artery with active bleeding and underwent total nephrectomy. | ||||
Figure 5 Twelve year old male patient who sustained blunt trauma in a road traffic accident. (A) Axial CECT nephrographic phase shows horse shoe kidney. (B) Axial image at a lower level and (C) coronal MPR image in the same phase show deep laceration involving its isthmus (white arrow) with mild perinephric collection. (D) Axial delayed phase shows extrarenal contrast extravasation (black arrow) denoting pelvicalyceal system injury (grade IV renal injury).
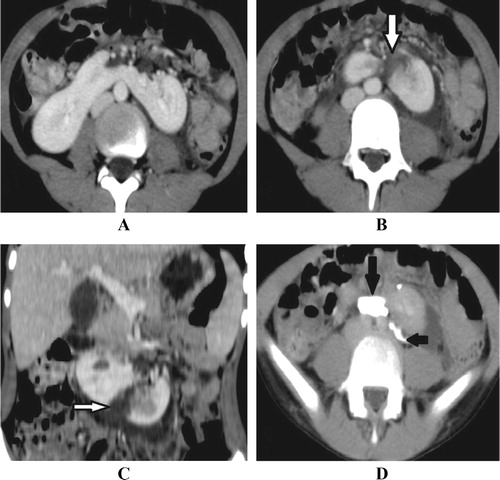
Figure 6 Twenty-two year old male patient with persistent hematuria following a stab injury, CECT revealed: (A) coronal MPR image nephrographic phase shows upper and lower deep left renal lacerations (white arrows). (B) Coronal MIP image in the delayed phase shows contrast extravasation (black arrows) denoting calyceal injury (grade IV renal injury). (C) Axial and (D) coronal MIP arterial phase show two pseudoaneurysms (open arrows) at the upper half of the left kidney with early rapid filling of the renal vein (arrow head) denoting arteriovenous fistula formation. (E) Selective left renal angiogram shows pseudoaneurysm (solid arrow) with arteriovenous fistula and rapid filling of the left renal vein (open arrow). (F) Selective left renal angiogram after successful embolization by five coils showing obliteration of the pseudoaneurysms and obstruction of the A-V fistula with no early filling of the renal vein.
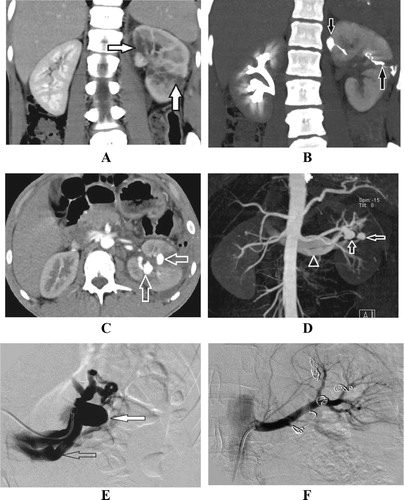
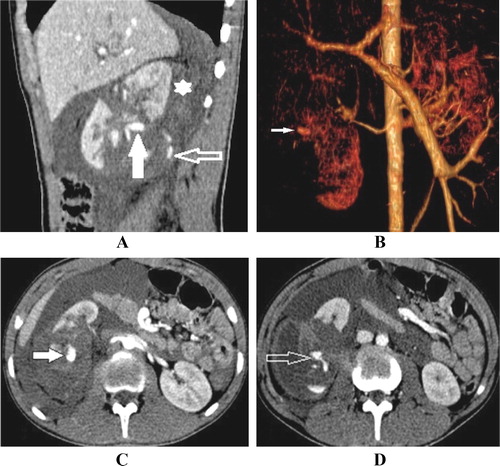
Figure 7 Eighteen year old male patient who sustained blunt trauma in a road traffic accident. (A) Sagittal MPR CECT venous phase shows shattered right kidney surrounded by moderate perinephric (asterisk) and paranephric hematoma (grade IV renal injury). (B) Volume rendering technique (VRT) image and (C) axial CECT arterial phase show pseudoaneurysm formation (white solid arrow) which is also noted in the coronal image. (D) Axial CECT arterial phase at a lower level demonstrates active arterial extravasation (open arrow) which again is noted in the coronal image.
Grade V injury was diagnosed in three patients (7.3%):
| • | One patient (2.4%) had renal vein avulsion associated with shattered kidney () and underwent total nephrectomy. | ||||
| • | One patient (2.4%) had thrombosis of the main renal artery with devascularization of the kidney sparing its lower pole that was supplied by accessory renal artery and was managed conservatively by follow-up. | ||||
| • | One patient (2.4%) had avulsion of the main renal artery with devascularization of the kidney () and died before management due to hypovolemic shock. | ||||
Figure 8 Thirty year old male patient who sustained blunt trauma in a road traffic accident. (A) Axial venous phase above the level of right renal vein and (B) axial cut below it demonstrate active contrast extravasation (open arrow) with moderate perinephric and paranephric hematoma (asterisk). (C) Axial venous phase at the level of right renal vein and (D) coronal MPR image show nonopacified right renal vein (solid white arrow) with normally opacified left one (arrow head). Right renal vein avulsion was found at surgery.
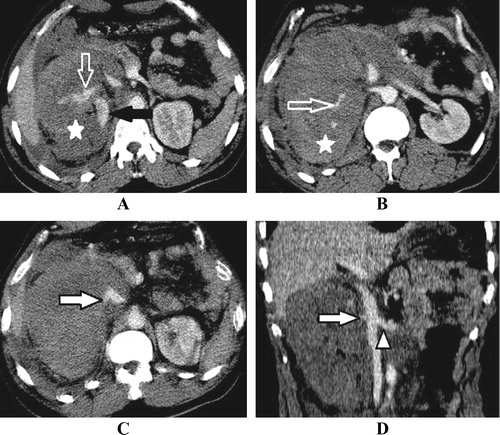
Figure 9 Twenty-eight year old female patient who sustained blunt trauma in a road traffic accident. (A) Axial CECT venous phase shows sudden interruption of right renal artery opacification (solid black arrow) with related foci of active contrast extravasation (solid white arrow) suggesting its avulsion, (grade V renal injury). This is associated with mild anterior pararenal hematoma. (B) Axial 5 min delayed phase at the same level shows increased extravasation of contrast, also noted, the absence of contrast excretion by both kidneys as the patient was shocked. (C) Coronal MPR CECT venous phase shows right sided total renal infarct sparing small enhancing area at the upper pole (open arrow). (D) Axial MIP image venous phase shows polar artery (arrow head) arising from the aorta supplying the remaining enhancing area.
Active bleeding was encountered in nine patients (22%), seven patients were classified as grade IV and two patients were classified as grade V of which four patients were managed conservatively, of whom one patient was complicated by pseudoaneurysm and arteriovenous fistula formation and underwent angiographic embolization, three patients underwent total nephrectomy and two patients died before management from severe hypovolemic shock.
RTRS was calculated for 34 patients with grades III and IV: ().
| • | All grade III patients were still stratified as grade III (low risk with 0 or 1 risk factor) who were managed conservatively. | ||||
| • | Thirteen patients with grade IV were substratified as grade IVa (low risk with 0 or 1 risk factor), 11 patients were managed conservatively, one patient underwent total nephrectomy and one patient died before management due to brain injury. | ||||
| • | The other nine patients with grade IV were substratified as grade IVb (high risk with 2 or 3 risk factors), four patients were managed conservatively, one patient underwent angiographic embolization, three patients underwent total nephrectomy and one patient died before management due to delayed transportation to hospital; however, he was in need to immediate intervention to stop bleeding. | ||||
Table 5 Distribution of patients with grades III and IV according to RTRS.
Regarding intervention for bleeding in the 34 patients with grade III and IV injuries, nine patients (26.5%) had RTRS of 2 or 3, so categorized as high risk, of whom five patients (55.5%) underwent intervention for bleeding versus only one of 25 patients (4%) with a RTRS of 0 or 1 ().
Table 6 Distribution of patients with grades III and IV according to risk category and intervention for bleeding after renal trauma.
Grade IV in the traditional AAST grading system had higher sensitivity (100%) and negative predictive value (100%) for intervention for bleeding than suggested high risk grade IVb classification while grade IVb classification had higher specificity (85.7%) and positive predictive value (55.5%) than traditional grade IV ().
Table 7 Sensitivity and specificity of grades IV and IVb for intervention for bleeding.
5 Discussion
This study included 41 patients with suspected renal injury following blunt and penetrating abdominal trauma. Twenty-eight patients (68.3%) suffered blunt abdominal trauma, with road traffic accidents being the most common cause that was encountered in 26 patients (63.4%) and fall from height was encountered in 2 patients (4.9%). The other thirteen patients (31.7%) suffered penetrating trauma, 11 patients (26.8%) had stab injury and the other two patients (4.9%) were gunshot.
Blunt abdominal trauma is responsible for most closed injuries of the genitourinary organs and accounts for up to 80–90% of all cases, with motor vehicle crashes being the most common cause while penetrating trauma accounts for approximately 10% of all renal injuries; however, its incidence is increasing.Citation12,Citation13
Serious renal injuries are frequently associated with injuries to other organs. Multiorgan involvement occurred in 78.5% of patients with blunt abdominal trauma and 54% of patients with penetrating abdominal trauma. This matched with Kawashima et al.Citation14 who mentioned that multiorgan involvement occurs in 75% of those with blunt trauma; however, it differs regarding its association with penetrating trauma that he mentioned that it occurs in 80% of patients with penetrating trauma. This may be due to the fact that most of patients with penetrating trauma included in this study had stab injury directed toward the flanks resulting in isolated renal injury.
The most commonly injured intraabdominal organ associated with renal injury was the liver (26.8%) followed by the spleen (22%), and this is consistent with Ramchandani et al.Citation13 who stated that the liver and the spleen are the most common intraabdominal organs to be injured with blunt trauma.
CECT examination was performed for all patients and they were classified according to the ASST grading system as follows: Grade I injury was diagnosed in one patient (2.4%) having small contusion without laceration nor perinephric hematoma, this contradicts Alonso et al.Citation12 and Smith et al.Citation15 who mentioned that Grade I injuries are the most common type of renal injury (75–85% of cases), which is explained by the fact that in case of blunt trauma, patients with grade I renal injuries are considered minor injuries that do not have perinephric collection and may lack also intraperitoneal collection if there is no other associated intra abdominal organ injury so exhibiting negative FAST examination; in addition, they are hemodynamically stable so CT examination will not be done except for gross hematuria if present. In our study, the only patient having grade I injury underwent CT examination due to the presence of mild to moderate intraperitoneal collection in FAST examination which was attributed to multiple liver lacerations after CT examination, while all patients with penetrating trauma included in our study had higher grade of renal injury.
Grade II injury was diagnosed in three patients (7.3%), one of them had laceration (<1 cm), the second patient had ruptured cortical cyst and the third patient had laceration (<1 cm) and hemorrhagic cortical cysts, while grade III injury was diagnosed in 12 patients (29.3%), all of them had deep laceration (>1 cm) not reaching the collecting system.
Grade IV injury was diagnosed in 22 patients (53.7%) being the most common injury included in our study, which may be attributed to the fact that grade IV injury is considered major renal injury that is mostly associated with considerable retroperitoneal hematoma in FAST examination and clinically the patient is mostly complaining of gross hematuria or hypovolemic shock so necessitating CT examination. Also, the last modification of the AAST grading system adds segmental arterial and venous injury, laceration to the renal pelvis or pelviureteric junction and shattered kidney from grade V to grade IV as mentioned by Dayal et al.Citation11
In the current study, grade IV injury included 10 patients (24.4%) with deep lacerations reaching the pelvicalyceal system, one patient (2.4%) with fractured kidney that was also associated with pelvicalyceal system injury, two patients (4.9%) with pelvic tear without associated renal lacerations, one patient (2.4%) with incomplete pelviureteric junction avulsion, one patient (2.4%) with segmental infarction and other small subsegmental infarcts without renal laceration nor perinephric hematoma, three patients (7.3%) with shattered kidney that was associated with pelvicalyceal system injury in 2 patients and active bleeding with pseudoaneurysm formation in the 3rd patient, one patient (2.4%) with expanding subcapsular hematoma, three patients (7.3%) with vascular injury, 2 patients had tear of the renal vein associated with IVC tear and multiple deep lacerations while the 3rd patient had avulsed segmental artery.
Grade V injury was diagnosed in three patients (7.3%), one patient (2.4%) had renal vein avulsion associated with shattered kidney, one patient (2.4%) had thrombosis of the main renal artery and one patient (2.4%) had avulsion of the main renal artery.
Dayal et al.Citation11 mentioned that although not detailed in the classification system, active arterial extravasation and pseudoaneurysm should suggest a higher grade injury and patients should be kept under close follow-up and be provided with early intervention if needed.
In the current study, active arterial extravasation was found in 9 patients (22%), 7 patients were classified as grade IV and two patients were classified as grade V. 4 patients were managed conservatively, 3 patients underwent total nephrectomy and 2 patients died before management from severe hypovolemic shock, while pseudoaneurysm was found in 2 patients (4.9%), one in the acute setting of trauma that was associated with active bleeding and the patient died before management, the other was found 2 weeks after conservatively managed trauma and the patient underwent angiographic embolization.
In the current study, all patients with grades I, II and III were managed conservatively. While as regarding grades IV and V, three patients (7.3%) died before management, 2 patients died due to severe hypovolemic shock resulting from renal as well as associated organ injuries and one patient died due to associated brain injury, 17 patients (41.5%) were managed conservatively by follow-up; however, one of them who had incomplete PUJ avulsion required double J insertion. Five patients (12.2%) underwent total nephrectomy, this is consistent with Alonso et al.Citation12 who stated that conservative management is now a widely accepted strategy for all but the most severe renal injuries in stable patients. And surgical intervention is performed in only 5–10% of renal injuries. The major benefit of nonsurgical treatment is the avoidance of iatrogenic nephrectomy.
From those who were managed conservatively, one patient who had fractured kidney was complicated by urinoma formation that was drained and another patient was complicated by pseudoaneurysm and arteriovenous fistula formation that was managed by angiographic embolization.
Total nephrectomy was done for five patients due to severe active bleeding and hemodynamic instability, and the only absolute indication for immediate exploratory surgery is the presence of “uncontrollable” active bleeding.Citation16
In a study of 102 trauma patients (73 patients with grade III (71.6%) and 29 patients with grade IV (28.4%)), urgent intervention was needed to achieve hemostasis in 18 patients (18.6%), including 8 of grade III (11%) and 10 of grade IV (35%). Angio-embolization was the most common hemostatic intervention (9 of 102 cases or 8.8%). Five patients (4.9%) underwent renorrhaphy and another 5 (4.9%) underwent nephrectomy.Citation17
The present study included 34 patients with grades III and IV renal injury, 12 patients (35.3%) with grade III and 22 patients (64.7%) with grade IV. Urgent intervention was needed to achieve hemostasis in 6 patients (17.6%), all of them were grade IV injury. Total nephrectomy was done for 4 patients (11.7%), one patient (2.9%) underwent angiographic embolization and one patient (2.9%) died before management due to delayed transportation to hospital; however, he was in need to immediate intervention to stop bleeding.
After calculation of RTRS, of our 34 patients, 9 patients (26.5%) had RTRS of 2 or 3, so categorized as high risk, of whom 5 patients (55.5%) underwent intervention for bleeding versus only one of 25 patients (4%) with a RTRS of 0 or 1; however, in our study, grade IV in the traditional AAST grading system had higher sensitivity (100% compared to 83% for grade IVb) and negative predictive value (100% compared to 96% for grade IVb) for intervention for bleeding than suggested high risk grade IVb classification while grade IVb classification had higher specificity (85.7% compared to 42.8% for grade IV) and positive predictive value (55.5% compared to 27.2% for grade IV) than traditional grade IV.
In the current study, renal artery thrombosis was found in one patient who was classified as grade V renal injury according to the traditional AAST grading system; however, he was managed conservatively, so this supported the opinion of Dugi et al.Citation17 who suggested that all thrombotic renal vascular injuries would best be categorized as grade IVa since they do not merit acute intervention and are typically not associated with significant perirenal hematoma.
We acknowledge limitations associated with this study including the relatively limited number of patients as well as the availability of follow-up assessment in only three patients. Despite these limitations, we emphasize the role of contract enhanced MDCT in the workup of patients with suspected renal trauma.
6 Conclusion
Contrast enhanced computed tomography (CECT) can help in the evaluation and management of renal trauma, and it provides the anatomic and functional information that is essential for accurate staging based on the AAST classification system. CT can help detect active hemorrhage and vascular injury including thrombosis, tear, avulsion and pseudoaneurysm formation and is very useful in guiding transcatheter embolization. It can detect urinary extravasation and pelvicalyceal system injury with its exact location as well as guiding its management. And so, it has an essential role in decision making regarding management of renal trauma either conservative or surgical based on CT findings and the AAST grading system.
Conflict of interest
None declared.
Notes
Peer review under responsibility of Alexandria University Faculty of Medicine.
Available online 10 July 2015
References
- Y.J.LeeS.N.OhS.E.RhaJ.Y.ByunRenal traumaRadiol Clin North Am4532007581592
- A.KawashimaC.M.SandlerF.M.CorlImaging of renal trauma: a comprehensive reviewRadioGraphics2132001557574
- J.K.SmithP.J.KenneyImaging of renal traumaRadiol Clin North Am415200310191035
- V.A.MasterJ.W.McAninchOperative management of renal injuries: parenchymal and vascularUrol Clin North Am33120062131
- A.C.HarrisC.V.ZwirewichI.D.LyburnW.C.TorreggianiL.O.MarchinkowCT findings in blunt renal traumaRadioGraphics21Special Issue2001S201S214
- S.M.GoldmanC.M.SandlerUrogenital trauma: imaging upper GU traumaEur J Radiol50120048495
- S.J.ParkJ.K.KimK.W.KimK.S.ChoMDCT findings of renal traumaAJR Am J Roentgenol18722006541547
- B.L.DunfeeB.C.LuceyJ.A.SotoDevelopment of renal scars on CT after abdominal trauma: does grade of injury matter?AJR Am J Roentgenol1905200811741179
- C.A.RaquelB.N.SusanaD.M.PatriciaS.G.AngelG.F.CarlosKidney in danger: CT findings of blunt and penetrating renal traumaRadiograghics29200920332053
- D.D.DanielF.M.AllenR.N.GeoffreyAmerican association for the surgery of trauma grade 4 renal injury substratification into grades 4a (low risk) and 4b (high risk)J Urol1832010592597
- M.DayalS.GamanagattiA.KumarImaging in renal traumaWorld J Radiol582013275284
- R.C.AlonsoS.B.NacentaP.D.MartinezA.S.GuerreroC.G.FuentesKidney in danger: CT findings of blunt and penetrating renal traumaRadiographics297200920332053
- P.RamchandaniP.M.BucklerImaging of genitourinary traumaAJR Am J Roentgenol1926200915141523
- A.KawashimaC.M.SandlerF.M.CorlO.C.WestE.P.TammE.K.FishmanImaging of renal trauma: a comprehensive reviewRadiographics2132001557574
- J.K.SmithP.J.KenneyImaging of renal traumaRadiol Clin North Am415200310191035
- G.SicaG.BocchiniF.GuidaM.TangaM.GuaglioneM.ScaglioneMultidetector computed tomography in the diagnosis and management of renal traumaRadiol Med11562010936949
- D.D.Dugi3rdA.F.MoreyA.GuptaG.R.NussG.L.SheuJ.H.PruittAmerican Association for the Surgery of Trauma grade 4 renal injury substratification into grades 4a (low risk) and 4b (high risk)J Urol18322010592597